Real prism use in ophthalmology
•
80 gostaram•17,675 visualizações

use of prism in optometry and ophthalmology

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Real prism use in ophthalmology
Semelhante a Real prism use in ophthalmology (20)
Mais de Bipin Koirala
Mais de Bipin Koirala (20)
Último
Último (20)
Real prism use in ophthalmology
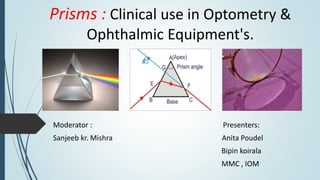
- 1. Prisms : Clinical use in Optometry & Ophthalmic Equipment's. Moderator : Presenters: Sanjeeb kr. Mishra Anita Poudel Bipin koirala MMC , IOM
- 2. Quote of the day…..
- 3. Presentation layout : Introduction Basic prism optics Prismatic effect on eye movement Prentice rule Instrumental use of prism Therapeutic use of prism Diagnostic use of prism Special cases Summary References
- 4. Introduction: Prism : A portion of a transparent isotropic substance included between two polished , nonparallel surfaces called refracting surfaces. A prism causes light to change direction without changing its vergence but the lens will change the vergence of light rays. Prism don’t necessarily have flat surface but may have curved surfaces as in ophthalmic lenses.
- 5. Some terminologies : Apex : The intersection of the refracting surfaces (extended if necessary) forms the apex of prism Refracting angle : The angle between two refracting surfaces is called as refracting angle. A.k.a Aptical and denoted by beta (β). Base of prism : The thick side of prism which substends the apical angle is called as base of prism. Angle of deviation : the angle between initial direction of light ray and final direction after refraction is called angle of deviation. It is denoted by epsilon (ε) Apex Base Refracting angle Angle of deviation
- 6. Contd.. Base apex line : If any point on the refracting edge is taken and principle section through that point intersects either refracting surfaces called base apex line Principle section : Any section of prism in a plane perpendicular to the edge is called as principle section. Fig : principle section of a prism with base apex line
- 7. Action of prism : A prism refracts the light rays towards base so the object is displaced towards apex. Image formed by prism is erect virtual and displaced towards apex. Object displaced towards apex
- 8. Refracting power of thin prism : Here, a = Angle of incidence in 2nd surface d = Angle of deviation I2’ =Angle of refraction n = Refractive index of prism n’ = Refractive index medium
- 9. Contd. From the previous figure we can say, Angle of incidence ( i2 ) = a Angle of refraction (i2’) = a + d Applying Snellen’s law at 2nd surface n sina = n’ sin ( a+d ) for small angles (< 10 degree ) n ( a ) = n’ ( a + d ) Finally ,if medium is air ( n’ = 1 ) then, final equation is with its unit in degree . d◦ = a ( n-1 ) Example , If the prism material is having refractive index of nearly 1.50 ( approx. of CR- 39 ) then d = (a/ 2)
- 10. Specification of power of ophthalmic prism Refracting power of a ophthalmic prism is specified in prism diopter ( ) . A prism diopter is defined as deviation of 1 unit at distance a distance of 100 units . For convenience amount of deviation is considered in centimeters (cm). d◦ d▲ x x 100 units 100 units Fig 1 Fig 2
- 11. Contd. We know , d◦ = a◦ ( n-1 ) From fig-1 tan d◦ = (x/100) i.e. x= 100 tan d◦ Now, if we can substitute x for prism diopter as we know amount of prism diopter is equal to the no of units deviation for 100 units of distance. d▲ = 100 tan d◦ i.e. d▲ = 100 tan a◦(n-1) Finally tan a◦ = d▲ / 100 (n-1)
- 12. Although angle of deviation can be stated in either degree or pd but refracting angle (d) is always stated in degrees Prism diopter differs from degree and radian because prism diopter is unit of tangent measurement but degree and radian are unit of arc measurment . 1 radian = (180◦/ π) = 57.5 degree 1degree = 0.0175 radian = 1.75 centrad ( because 100 centrad = 1 radian) For small angles 1 centrad is equal to 1 prism diopters so 1 degree = 1.75 prism diopters 1 radian Arc equal To radius
- 13. 1 centrad unit Less frequently used unit to specify prism power. Denoted by (▼) sign The difference between the two is that a prism diopter is measured on a flat plane 1 m away whereas the displacement of a centrad is measured on the arc of a circle having a 1-m radius
- 14. Ways to specify prism base directions: There are many ways used to specify prism orientations . But most commonly used notation are illustrated in figure. OD OS Method 1
- 15. Method 2
- 16. Effects of prism on eye movement Monocular effect A person is watching distant object monocularly A prism is introduced in front of his open eye at any orientation The image of object is displaced towards apex So to look the image of object persons eye moves by an amount equal to angle of deviation. Orientation Direction of eye movement Base up Downward Base down Upward Base in Outward( abduction) Base out Inward ( adduction) nose
- 17. Binocular effect When a person fixates an object with both eye open And prism ( suppose equal power ) is introduced infront of both eyes If base is in same direction in both eyes ( base in in both eye or base out in both eyes then it produces vergence movement. If base are in opposite direction in both eyes ( base in in one and base out in next it produce version movement. Vergence Version
- 18. Resultant prismatic effects: Horizontal prismatic effect: 1. Prism placed before each eye with their bases in same direction for each eye i.e. both base in or both base out then resultant prismatic effect will be additive 2. But if bases are in opposite direction resultant effect will be difference b/w the power of two prism with resultant base towards stronger prism. Additive effect Subtractive effect
- 19. Vertical prismatic effect 1. Vertical prisms before each eye in same base direction will give net resultant effect after subtraction of weaker prism from stronger one and base direction remains same as overall base direction. 2. If prism before each are indifferent base direction net effect will be additive and net base direction can be specified with respect to each eye . Subtractive effect Additive effect
- 20. Prentice rule: An spherical lens can be considered as being made up of infinite number of prisms stacked together. Prism are stacked base to base for plus lens and stacked apex to apex for minus lens. So both positive and negative lens show prismatic properties that gradually increases towards periphery from the pole of lens. Prismatic effect depends not only in the distance from pole also depends on the power of the the lens.
- 21. Prentice rule contd.. Prismatic effect(P)= c F Where c is displacement away from pole of lens in (cm) and F is power of lens in diopters.
- 22. Prism positioning: Prentice position. Glass prisms are calibrated for use in this position, so the line of sight makes a right angle with one of the surfaces( usually back surface). Ophthalmic glass prism are calibrated for prentice positioning. Minimum deviation position. Plastic prisms, including plastic prism bars, are calibrated in this position, so the line of sight makes an equal angle with each prism surface. Difficult to obtain in clinical practice.
- 23. Frontal plane positioning. Holding plastic prisms in this position, with the back surface flat to the face of the patient, closely approximates the minimum deviation position, which would otherwise be difficult to estimate in clinical practice
- 25. Types of prism : Dispersive : Abbes , Triangular Polarizing : Nicol , Wollaston Reflective : Penta , Porro , Dove prism
- 26. Nicol prism 1. Made from a piece of calcite crystal cut diagonally in half with the two halves cemented together with Canada balsam or a low refractive index optical cement. 2. Incident light is split into ordinary and extra- ordinary linearly polarized rays in the prism: - the ordinary rays reaches the interface and is totally reflected, - the extra-ordinary ray is transmitted. 3. Best for Haidinger’s Brushes (Nowadays : dichoric filter) 26
- 27. Wollaston prism 2 right-angled prisms of equal angle made of a double refracting surface such as quartz or calcite cemented together by their hypotenuse faces to form a rectangular unit. A beam of unpolarized light incident on it will emerge as two diverging beams which are oppositely polarized and almost free of dispersion. 27
- 28. Porro prism • Type of reflection prism used to alter the orientation of image. • A image travelling through the prism is rotated by 180º • Exit in the opposite direction offset from its entrance point. • In slit lamp double porro prism are used , net effect is beam parallel to but displaced from its original direction with image rotated 180º
- 29. Prism in ophthalmic instruments Slit lamp Applanation tonometry Indirect Ophthalmoscope Keratometer Phoropter Synaptophore Exophthalmometer Pupilometer Haidinger's brushes Koppes Gonio lens Operating microscope
- 30. Slit lamp Two Porro prisms Set of 45-45-90 Porro prism Overcome the problem of inverted image produced by compound microscope Brighter image
- 31. Ophthalmoscope May prism Made up of solid glass Consists of convex lower end , acting as condenser and angled upper portion serving as reflector
- 32. Applanation tonometry GAT uses Bi prism Two prism with their bases in opposite direction are placed in head Split the applanated area into 2 and two half images by 3.06mm
- 33. Keratometer 1. Wollaston prism 2. Light passing cornea is reflected through obj lens . Diaphragm with 4 aperture 3. Light passing through one of the horizontal aperture also pass through Base up prism vertically displaced image Base out horizontally displaced image
- 35. Phoropter Risley prism (Rotary prism) Knob oriented vertically BI /BO prism power introduced horizontally BU/BD prism power Measure phoria , fusional vergence
- 36. Indirect ophthalmoscope 1. Reflecting prism 2. Erect the inverted image 3. To maintain binocularity reducing IPD
- 37. Gonioscope 1. Reflecting prism 2. Overcome the problem of TIR easy viewing of AC angle Synaptophore 1. Reflect ray in right angle
- 38. Exophthalmometer Haidinger's brushes
- 39. Prism in low vision A) Half eye prism reading microscope 1. Convex spherical lenses which allow BV 2. Early aid prescribed to reading 3. Prism power = power of microscope + 2 4. Prescribed in power from +5 to +16
- 40. B) Fresnel prism 1. Plastic sheet of parallel tiny prism of identical refracting angle 2. Overall prismatic effect is same as of single prism 3. 1 mm plastic polyvinyl chloride material , applied to base surface of spec 4. Prism placement side of defect , base towards the defect
- 41. Condition in which we can prescribe are Bitemporal hemianopia RP Glaucoma Brain injury Stroke Patients may benefit from placement of a Fresnel or ground-in prisms in their spectacles. It can be used as a definitive treatment for small amounts of strabismus or as a temporary treatment while waiting for the strabismus to stabilize.
- 42. Advanced glaucoma and RP patients with tubular vision have to restrict the eye movement to a limited range. Prisms help to displace peripheral blind area of visual field toward the straight ahead position to the seeing area of visual field. Small segment of Fresnel prism 5 mm from the center of pupil with its BI the same direction of restricted visual field will help the patient.
- 43. Pros Cons Lighter – more comfortable VA Cosmetically superior contrast Should be chief to manufacture distortion and chromatic aberration Convenient Difficult to keep clean High power possible (0.5 to 30 prism diopter) discolor with time inferior optically
- 44. C) Field expanding channel lenses 1. lens system composed of two12 p.d. lateral prism and one 8pd inferior prism 2. Apex toward central non prismatic channel 3. Distance Rx can be upto +/-8DS and +/-7DC and also bifocals if needed 4. Designed for various degree of peripheral field loss by having pts use specific size of peripheral field that is remaining 5. Lens channel be aligned with the peripheral edge of functional retina so that as field ( ) size so too does the width of channel
- 45. Designed for improved mobility , pts. viewing object through channel while having advantage of temporal ,nasal , Inferior awareness Recommended for glaucoma, RP Field loss Recommended size of channel(mm) Beyond 20 degree 14 To 20 degree 12 To 15 degree 10 To 10 degree 8 To 6 degree 6
- 47. Prism in ARMD Used for Image relocation Prisms were added to prescription glasses to produce IR to the presumed preferred retinal locus Main outcome measures were best-corrected visual acuity (BCVA) improved. This effect is probably created by facilitation of oculomotor functions resulting from direct reduction of fixation instability. 2006 Jun;41(3):313-8. Image relocation with prisms in patients with age-related macular degeneration. Al-Karmi R1, Markowitz SN.
- 48. Prism in hemi spatial neglect due to stroke. Patients who experience right hemisphere strokes often experience left hemi spatial neglect. Recent studies have shown that yoked prisms which move both visual fields to the opposite side (to the right) improve function in these patients.
- 49. Prism in ankylosing spondylitis Patients with head or neck positioning problems, such as patients with severe ankylosing spondylitis, may benefit from prisms. In patients with an orthopedic chin-down posture, for example, bilateral equal-power, base-up “yoked” prisms can allow for improvement in straight-ahead vision and thereby facilitate mobility.
- 50. Prism in keplerian telescope Used to erect the image
- 51. Prism reading spectacle: Bedridden patients are forced to read or watch television in extreme downgaze. If they are provided with 15– 30 Δ , base-down prism in the form of recumbent spectacle will allow the patient to read comfortably. Prisms in Fresnel form are given temporarily till the patients recover.
- 52. Prism in contact lenses Prism in CL are used in Toric CL for the stabilization of lens ,they are a) Prism ballast b) Peri ballast c) Reverse prism
- 53. a) Prism ballast 1. 1 to 1.5 pd BD 2. stabilized by prism induced thickness diff
- 54. b) Peri ballast Minus carrier is converted into BD effect Uses thickness diff as the stabilizing component To create BD effect , superior carrier is slabbed – off or chamfered superiorly
- 55. c) Reverse prism 1. incorporate both prism( BD) and the inferior chamfer (BU) 2. Base-to- base line is located below the geometric center 3. Cyl component limited to optical zone which is prism less
- 56. Prism in nystagmus Prismo therapy in nystagmus may be useful as a) BO prism : stimulate fusional convergence thus improve VA dampening nystagmus b) Prism with base opp to preferred dirn of gaze correcting head posture eg. If head turn is in left , null position is in dextroversion BI before RE, BO before LE
- 58. Therapeutic uses of prism in Optometric practice
- 59. Prism types for therapeutic uses. Prism Reliving prism Over corrective prism Inverse prism Yoked prism Rotating prism Regional prism Corrective prism
- 60. Relieving prism: Aim : Optically reduces the demand to fusional vergence and stabilizes the sensory motor fuison Amount prescribed: Less than the deviation( phoria or dissociated deviation in strabismus) Commonly prescribed for phorias and intermittent deviations. Way to prescribe : Type of deviation Prism position Exo deviation Base in Eso deviation Base out Hyper deviation Base down Hypo deviation Base up
- 61. Contd… Mechanism : 1. when base in prism is prescribed the retinal image moves nasally and amount of convergence needed to obtain bifoveal fixation of real object is optically reduced for exo deviation. 2. And eye will turn outward with base in prism. 3. When base out prism is prescribed retinal images are moved temporally and amount of divergence needed to obtain bifoveal fixn object of regard is optically reduced for esodeviation. 4. And eye will turn inward with base out prism. 5. Similar is for hyper deviations.
- 62. Relieving prism position A A’ A’ A Exophoria Esophoria
- 63. Reliving prism prescription criteria's: Criteria for prescribing reliving prism can be grouped into 3 groups. 1. Minimum prism criteria 3. Associated prism criteria a. Fusion prism criteria b. Sheard’s criteria c. Percival’s criteria d. Fixation disparity criteria 2. Dissociated prism criteria a. Percentage prism criteria b. Residual vergence demand ( RVD )
- 64. Corrective prisms: Aim: Optically eliminates the oculomotor deviation so residual vergence demand is zero Amount prescribed: Equal to the size of oculomotor deviation so that retinal images are centered in fovea. Problematic for incomitant deviation Ways to prescribe : Type of deviation Prism position Exo deviation Base in Eso deviation Base out Hyper deviation Base down Hypo deviation Base up
- 65. Contd.. Mechanism : With the use of prism stimulation of corresponding retinal points with eye remaining in deviated position is possible Best for basic esotropia of recent onset and infantile esotropia to establish normal visual development before surgical procedure.
- 66. Over corrective prisms: Aim: Optically changes the direction of deviation. Amount to prescribe: larger than the deviation and commonly prescribed amount is (deviation +10 pd ). Way of prescription: Type of deviation Prism position Exo deviation Base in Eso deviation Base out Hyper deviation Base down Hypo deviation Base up
- 67. Mechanism: Over corrective prism moves the retinal image beyond fovea in the opposite hemi retina than that was previously stimulated. Example : In an esodeviation with application of over corrective prism esotropic eye changes to optically exo deviated eye as temporal hemi retina is stimulated Uses : 1. To eliminate existing suppression zone in retina. 2. Change ARC to NRC especially in constant esotropes 3. A change in direction of deviation of eye is seen with OCP during prism cover testing. Also called as disruptive prism
- 68. Figure of over correcting prism Ray diagram for Esotropic eye Ray diagram after overcorrection
- 69. Inverse prism: Aim : Optically increases the demand to controlling fusional vergence. Amount to prescribe: Usually 2-6 pd is prescribed initially with gradually increment in the strength of prism for constant wear or certain visual activities. Way to prescribe: Type of deviation Prism position Exo deviation Base out Eso deviation Base in Hyper deviation Base up Hypo deviation Base down
- 70. Mechanism: Optically increases the strength of controlling fusional vergence. Uses : 1. Acts as passive therapy method to improve fusional vergence ability when prescribed for constant wear with spectacles. 2. For cosmesis in small angle constant strabismic patient (amount usually given : 5 – 10 p.d. ) 3. Used to eliminate ARC 4. Used to eliminate eccentric fixation 5. Used as training prism or exercising prism. 6. Also called disruptive prism
- 71. Yoked prism: Aim : To move both eyes synergistically away from primary gaze into different field of gaze to stabilize binocular vision . Amount to prescribe : Differs from patient to patient but usually 5 -10 p.d. are prescribed Way to prescribe: Prisms with bases parallel in two eyes with both prisms bases right or left or up or down
- 72. Mechanism : Yoked prism optically moves the retinal images of a fixed target in parallel direction towards the base of prism the apparent target towards the apex of the prism. Uses : 1. Combined with reliving prism for non comitant deviations , DRS , gaze palsies 2. In patients with homonymous field loss. 3. To dampen nystagmus by directing eyes to null zone 4. Also applicable for bedridden ( vertical yoked ) and people with certain physical disabilities A.K.A Version prism
- 73. Yoked prism : Before After
- 74. Rotating prism: Aim : To change ARC to NRC Amount to prescribe: Vary from person to person but 10 pd is most preferred amount Way to prescribe : Base of prism is rotated at certain time interval (1 wk ) from base out to base in to base up and same sequence is repeated and prism is given as Fresnel form Mechanism: Provides a method of changing sensory input for constant strabismic patient Uses: 1. Monocular viewing rotating prism applicable for amblyopia therapy 2. Binocular viewing rotating prism applicable for treating ARC
- 75. Regional prism: Aim : To stabilize BSV in different gaze or at different distance. Way to prescribe : Prescribed as reliving prism often combined with yoked prism and given in Fresnel form. Mechanism : Reduces demand for controlling fusional vergence in more than one gaze or distance Also called as Sector prism
- 76. Vision therapy in optometry with prisms: Types of prism used for therapy Risley prism Prism flipper Prism bar Loose prism
- 77. Prism therapy can be given monocularly as well as binocularly. Monocular therapy are used to improve the patient awareness of his or her eye movement to enhance fixation and saccade ability. Binocular prism therapy are used to create vergence demands in free spaces.
- 78. Types of therapy procedures: Monocular prism saccade therapy. Binocular prism jump with loose prism or prism bar For patient with saccadic deficiency also used to improve fixation in amblyopic eyes. For Heterophores and well controlled intermittent deviation to increase fusional vergence ability and vergence facility.
- 79. Contd.. Binocular prism jump with prism flipper To increase smoothness and speed of fusion.
- 81. Diagnostic uses of prism can be explained under following subheadings: Assessment of torsion Test for retinal correspondence Correction of deviation Measurement of angle of deviation Investigation of BSV and its components Test for malingering Pre operative diplopia test Diagnostic uses of prism
- 82. 1. Measurement of angle of deviation . Prism cover test 1. Objective method 2. Materials required : Prism bar , Occluder , (Near + Distance) targets 3. Prism placement: Apex towards deviation. 4. Alternate cover test is performed until neutralization. For large angled deviation and combined horizontal & vertical deviation prism can be divided b/w two eyes
- 83. Prism reflex test ( krimsky’s corneal reflex test) 1. Objective method 2. Performed at near with point light as fixing target. 3. Materials required: prism bar , pen light 4. Useful in large squint , deeply amblyopic as well as blind eye
- 84. Prism placement: Prism is placed before fixing eye with Apex towards deviation. Prism power is gradually increased till corneal reflex is centered in squinting eye
- 85. Simultaneous prism cover test. 1. Objective method and special form of cover test 2. Used to measure tropia without dissociating phorias. 3. Useful for small angled tropia (<10▲) and larger phoria i.e. monofixation syndromes. 4. Occluder ( in front of fixing eye) and prism ( in front of deviating eye are placed simultaneously until neutralization of eye movement 5. Prism placement : Apex towards deviation
- 86. Maddox rod test: 1. Subjective method to access the angle of deviation. 2. Can detect horizontal , vertical as well as torsional deviation. 3. It is an dissociating test based on principle of diplopia. 4. Materials required: Maddox rod , occluder , spot light target , prism bar.
- 87. Contd.. 5. Placement of Maddox rod : Axis of rod is placed parallel to axis of deviation. 6. Then prism of successive increasing power is placed in front of rod until red streak crosses the spot . 7. Prism placement : Apex towards deviation . Limitations of Maddox rod test: 1. Cannot be done in suppression 2. Difficult to perform in large angled deviations. 3. Error may occur in ARC.
- 88. Double Maddox rod test: Used to identify and quantify cyclodeviation Materials required : 2 Maddox rods ( red + white) , spot light target , and 6 ▲ prism Maddox rod are placed with axis in vertical direction in both eyes. Prism placement and use : Base down or up in front of one eye so that two colored streak can be differentiated easily 2. Assessment of torsion
- 89. Maddox double prism test: Qualitative test for cyclodeviation. Materials required: Two prisms( 4 ▲ ) , Horizontal line target. Can be done only at near 33cm. Procedure: 1. Prism are mounted base to base and placed before one eye ( say right if left is being tested) 2. Pts asked to view horizontal line target at 33cm. 3 . Patient will see 3 lines middle line by left eye and upper and lower by right. 4 . Based on orientation of central line with respect to two outer line interpretation is made. RE LE
- 90. Contd.. Orientation of central line Interpretation No tilt No cyclodeviation Tilted outward Left eye incyclodeviation Tilted inward Left eye excyclodeviation
- 91. 3. Investigation of BSV and its components Prism reflex test ( induced tropia test ) 1. Used to investigate BSV and find small angled deviation in infant and children's. 2. Fixation pattern of fixing eye is studied with horizontal BO prism in front of fellow eye. 3. Same procedure is repeated for next eye too. 4. Commonly used prism is (10▲ BO – 25 ▲ BO) 5. By inducing tropia , fixation preference is studied.
- 92. Interpretation of prism reflex test. Result 1 : If BSV is present with normal motor fusion , after placing prism diplopia will be induced and both eye will make version movement and fellow eye will show refixation movement. (Hering’s law obeyed) Result 2 : If BSV is not present ,on placing prism over suppressed eye no version movement will be seen but if placed over non suppressed eye version movement is seen but no refixation or fusional movement is noted. Result 3: In some cases of alternate deviation b/w two eyes alternate fixation preference is seen b/w two eyes Vertical prism superior to horizontal prism
- 93. Prism 4▲ test 1. Performed to detect small angled deviation and presence of central suppression scotoma. 2. Can be performed for both near and far . 3. Materials required : 4 p.d. prism , fixation light for near and distance. 4. Procedure : 4 p.d. BO prism is place in front of each eye alternately and necessary interpretation is made
- 94. Interpretation of 4 ▲ test When BO prism is placed in front of Rt. Eye (say) then : Result 1 : If normal biphasic corrective movement of left eye is seen then pts has normal BSV. Result 2 : Absence of normal biphasic movement indicates presence of central suppression scotoma Mechanism : Prism displaces image towards its base i.e towards a point in temporal half nearly 2 degree . So the relaxation movement of right eye will induce conjugate movement of left eye ( levoversion) , If right eye has no suppression . This displaces the image in left towards temporal retina from fovea ,thus left eye now makes fusional movement in opposite direction, if no foveal suppression is present. Central suppression scotoma
- 95. Fusional vergence amplitude: Prism bar / Risley prism can be used to measure fusional vergence amplitude . Measured for both near (33cm)and distance(6m). Horizontal ( positive and negative ) vergence amplitude as well as vertical vergence amplitude can be measured. Prism bar of increasing strength is placed in front of eye with patient instructed to look at fixing target at certain distance. Three points i.e. Blur point , Break point and Recovery point are noted . Fusional vergence amplitude measured by prism bar is step fusional vergence.
- 96. Contd.. Normal values: Category Normal values Base out ( distance) Blur 9 p.d. Break 11 p.d. Recovery 7 p.d. Base out (near) Blur 17 p.d. Break 19 p.d. Recovery 14 p.d. Base in ( distance ) Blur - Break 7 p.d. Recovery 4 p.d. Base in ( near ) Blur - Break 13 p.d. Recovery 10 p.d. Source : Clinical management of Binocular vision 4th edition by Mitchell scheiman & Bruce wick
- 97. Vergence facility test: Important test used to detect binocular vision disorders. Done at near i.e. 40 cm . Purpose : Test ability of vergence system to respond rapidly and accurately to changing vergence demand. Measure as cycle per minutes Normal value is 15 cpm . Prism flipper with 12 ▲ BO and 3 ▲ BI prism is used.
- 98. Contd.. Testing procedure: 1. Pts views an vertical target ( 20 / 30 ) at 40 cm . 2. Prism power of 12 ▲ BO and 3 ▲ BI are alternately placed in front of pts one eye . 3. Pts is instructed to make single and clear view of target and immediately prism is flipped to next power . 4. And the numbers of complete cycles per minute is noted. 5. Absence of eye movement indicates suppression.
- 99. Prism are also use to measure AC/A & CA /C ratio
- 100. 4. Test of retinal correspondence. Prism bar and red filter test. Materials required : prism bar , red filter , spot light for fixation at 6 m . Firstly amount of deviation is estimated for distance by PBCT ( objective angle ) Prism is placed in front of fixing eye . Red filter is placed in front of deviating eye and patient is asked to describe what he sees.
- 101. Interpretation of result: Result 1 : Patient doesn’t sees red light then eye is suppressed. Result 2 : Patient sees light as blend of red and white then , NRC. Result 3 : Pts sees two lights i.e. white and red light then, ARC 1. Paradoxical diplopia is appreciated. 2. For eso deviation cross diplopia & for exo uncrossed diplopia. 3. To find subjective angle of deviation prism bar is gradually reduced until diplopia disappears or changes its nature. 4 . By difference b/w SA and OA angle of anomaly is obtained .
- 102. Prism use in suppression: Prism for investigation of suppression : Area of suppression can be measured with prism. Measured by displacing image nasally, temporally, Vertically ( up and down ) Diplopia will be appreciated when image falls outside scotoma zone .
- 103. Contd.. Prism as a part of Anti suppression exercise (Diplopia exercise by prism): 1. Used to make patient aware of physiological diplopia in intermittent deviations. 2. Vertical prism (BU or BD ) sufficient enough to displace image out of suppression scotoma is placed in front of one eye 3. Gradually prism power is reduced until finally patient appreciates diplopia without any vertical prism. 4. In this way patient is taught to appreciate diplopia for both near and distance.
- 104. 5. Test for malingering Prism base down test : 1. Prism of power (4-6) ▲ BD is palced before good eye 2. If patient sees diplopia at the fixation target. 3. It proves malingering. Prism base out test . 1. Prism of power (10- 16) ▲ BO is taken 2. Prism placed before alleged blind eye 3. If eye moves inwards i.e. to avoid diplopia 4. It indicates gross vision is present and malingering is proved.
- 105. 6. Pre-op diplopia test. Some portion of adult people suffer from intractable diplopia. Prism adaptation test is pre-op diagnostic test to identify potential for BSV and predict risk of post op diplopia. Done before strabismus cosmetic surgery. Patient may experience post op diplopia due to poor motor alignment. Prism bar is used for this purpose and test should be done for both near & distance. Firstly deviation is neutralized with prism bar by Alt .prism cover test .
- 106. Contd.. Then at neutralization point pts is asked whether diplopia is seen or not . Then prism bar is removed and again started from zero prism diopter till deviation is over corrected by 5 - 10 p.d. and pts is instructed to inform If he reports diplopia at any position . Interpretation: Result 1 : If Pts reports diplopia then prism power is increased and decreased several times if any position where diplopia is eliminated i.e. if position of fusion is not obtained ( pts has chance of post-op diplopia) Result 2 : If pts doesn’t report diplopia i.e. any position for fusion is obtained then probably he won’t have post-op diplopia
- 107. Post operative prism use Prism is also used to eliminate post operative intractable diplopia by increasing the image separation or maintaining BSV . Fresnel prism is used for this purpose . Some examples Surgically over corrected exotropia ( consecutive esotropia) 1. Mostly pts develop good fusional divergence with in certain day of surgery 2. If stable esotropia persists over 1 months of surgery the BO prism are prescribed to prevent diplopia 3. For larger overcorrection re-surgery is needed
- 108. Surgically under corrected exotropia 1. Use of BI prism immediately after surgery is helpful to establish good fusion 2. Usually overcorrecting prism are used ( 10 p.d. greater than deviation) 3. But it has been reported to be unsuccessful for most of the time. Surgically overcorrected convergence insufficiency 1. May spontaneously develop post op diplopia 2. During this period prism therapy may be useful.
- 109. Prism prescription in convergence and divergence anomalies Convergence insufficiency 1. Convergence exercise with prism bar to increase amplitude of fusional convergence. 2. Base in reliving prism for near work fitted in bifocal. Convergence paralysis 1. Base in prism are prescribed especially for near work. 2. Plus lens with near add may be required for associated accommodative anomalies.
- 110. Contd.. Divergence insufficiency. 1. Base out prism is prescribed to give comfortable BSV at distant. 2. Not mostly practiced , prism is gradually reduced and avoided. Divergence paralysis 1. Same as above.
- 111. Guidelines for prism prescription to avoid diplopia Lowest prism amount that makes pts is comfortable. Prism power can be divided into two eyes for good cosmesis and weight. Step wise guidelines: 1. First measure amount of deviation vertical as well as horizontal in primary gaze. 2. If both H and V deviation are present resultant oblique prism power is estimated 3. Starting prism power is equal to = larger deviation + (smaller deviation/2)
- 112. Examples: If pts is 20 p.d. eso and 10 p.d. left hypertropia then starting prism will be: 20 + (10/2) = 25 p.d. 4. So 25 p.d. prism is taken as starting prism. 5. And 25 p.d. will be placed before non-dominating eye always 6. Prism positioning will be b/w base out and slightly base down before left eye. 7. Prism is slightly rotated in clockwise and anticlockwise direction to find oblique prism position in which diplopia is eliminated at least at primary position .
- 113. 8. If diplopia is not eliminated with starting prism then prism of slightly small or higher power are taken and same procedure is repeated as point 7. 9. Finally prism power and its oblique orientation ( angle) is noted and prism is prescribed In the form of Fresnel prism. How to Prescribe a Prism for Combined Vertical and Horizontal Strabismus Written By: J. Scott Kortvelesy, MD Edited by Ingrid U. Scott, MD, MPH, and Sharon Fekrat, MD Q) If right eye is 16 p.d. exo and 6 p.d hypo then what would be necessary prism amount???
- 114. Summary : Prism has wide application in the field of ophthalmology and optometry . And its uses can be categorized into instrumental , therapeutic & diagnostic use.
- 115. References: Squint and orthoptics by A.K. khurana System of ophthalmic dispensing Binocular vision by G.K von noorden Clinical management of Binocular vision 4th edition by Mitchell scheiman Clinical optics Internet
- 116. Hillary Clinton with Fresnel prism in her spectacle
Notas do Editor
- When prism is placed in front of eye the image previously centered on fovea will get displaced by equal amount to the effective power of prism so to gain refixation eye will make duction movement.
- Although angle of deviation can be stated in either degree or pd but refractiong angle (d) is always stated in degrees Prism diopter differs from degree and radian because prism diopter is unit of tangent measurement but degree and raduian are unit of arc measurment .
- Method 1 similar to cylinder axis Method 2 is based in orientation of base of prism.
- bThe amount of strabismic deviation produced or measured by a prism depends on the position in which it is held. It is thus critical to understand how to hold prisms correctly. Ophthalmic prisms made of glass are calibrated for use in the Prentice position and should be held with one surface, usually the back surface perpendicular to the patient's line of sight [Figure 3a]. Plastic prisms, including plastic prism bars, on the other hand, are calibrated for use in the minimum deviation position, in which, as the name implies, the least amount of total deviation is produced, with equal amounts of bending occurring at each prism surface [Figure 3b]. In clinical practice, it may be difficult to position prisms accurately according to the angle of minimum deviation, but holding them in the frontal plane position, with the back surface flat to the face of the patient, closely approximates the minimum deviation position for distant fixation objects [Figure 3c].4 For near fixation objects, the back prism surface should be angled in slightly, so that it is perpendicular to the fixation object.5 In general, if plastic prisms are held with the back surface perpendicular to the direction of the fixation object, essentially equal angles of bending occur at both surfaces, serving as an ideal surrogate for the minimum deviation position at all times.
- Fuisonal vergence will control the deviation and results in bifixation of viewed target.
- So sensory fuison can occurs without fusional vergence needed is zero. Assuming deviated eye is not suppressed.
- To eliminate arc slightly greater amount ie 2pd more is prescribed in eye with EF with good eye occluded and prismmis for constant full time wear. Base out for temporal EF and viceversa.
- Reliving will reduce vergence controlling demand and yok will move eye to direction in which binocularity is possible . Dispalces target from non seeing area to the seeing area . Reduces AHP and abnormal head nodding.
- Varying type power can be incorporated so fresnal prism is used.
- For large deviation loose prism can also be used .
- Both with and with out eccentric fixation can be evaluated.
- Not applicable for larger phorias because it doesn’t permit fusion
- Can be done only for near.
- Vertical prism is superior to horizontal prism because vertical prism can easily break prephiral fusion and central suppression scotoma comlex so it avoids misinterpretation in cases of amblyopia and monofixation syndromes.
- CIP changed image position
- Ca/c ration by Binocular cross cyl method and dynamic retinoscopy method.
- In suppression eye test is of no use. NRC because two eye has common visual direction . Diplopia is called paradoxical diplopia .
- In cases of surgical overcorrections , palsies