Communication in nursing
•Transferir como DOCX, PDF•
3 gostaram•1,334 visualizações

communication,meaning, process, communication in nursing services by the nurses.

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Communication in nursing
Semelhante a Communication in nursing (20)
Mais de anjalatchi
Mais de anjalatchi (20)
Último
Último (20)
Communication in nursing
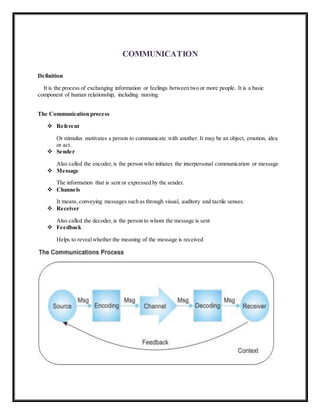
- 1. COMMUNICATION Definition It is the process of exchanging information or feelings between two or more people. It is a basic component of human relationship, including nursing. The Communication process Referent Or stimulus motivates a person to communicate with another. It may be an object, emotion, idea or act. Sender Also called the encoder,is the person who initiates the interpersonal communication or message Message The information that is sent or expressed by the sender. Channels It means, conveying messages such as through visual, auditory and tactile senses. Receiver Also called the decoder,is the person to whom the message is sent Feedback Helps to revealwhether the meaning of the message is received
- 2. Modes ofCommunication Verbal communication– uses the spoken or written word 1. Pace and Intonation The manner of speech,as in the pace or rhythm and intonation, will modify the feeling and impact of the message. For example, speaking slowly and softly to an excited client may help calm the client. 2. Simplicity Includes the use of commonly understood words, brevity, and completeness. Nurses need to learn to select appropriate, understandable terms based on the age, knowledge, culture and education of the client. For example, instead of saying to a client, “the nurses will be catheterizing you tomorrow for a urinalysis”, I would be more appropriate to say, “Tomorrow we need to get a sample of your urine, so we will collect it by putting a small tube into your bladder”. 3. Clarity and Brevity A message that is direct and simple will be more effective. Clarity is saying precisely what is meant, and brevity is using the fewest words necessary. The goal is to communicate clearly so that all aspects of a situation or circumstances are understood. To ensure clarity in communication, nurses also need to speak slowly and enunciate carefully. 4. Timing and Relevance No matter how clearly or simply words are stated or written, the timing needs to be appropriate to ensure that words are heard. This involves sensitivity to the client’s needs and concerns. E.g.,a client who is enmeshed in fear of cancer may not hear the nurse’s explanations about the expected procedures before and after gallbladder surgery. 5. Adaptability What the nurse says and how it is said must be individualized and carefully considered. E.g., a nurse who usually smiles, appears cheerful, and greets his clients with an enthusiastic “Hi, Mrs. Jones!” notices that the client is not smiling and appears distressed. It is important for the nurse to then modify his tone of speech and express concern in his facial expression while moving toward the client. 6. Credibility Means worthiness of belief, trustworthiness, and reliability. Nurses foster credibility by being consistent, dependable, and honest. Nurses should convey confidence and certainly in what they are saying, while being to acknowledge their limitations (e.g.,“I don’t know the answer to that, but I will find someone who does”. 7. Humor The use of humor can be a positive and powerful tool in nurse- client relationship, but it must be used with care. When using humor, it is important to consider the client’s perception of what is considered humorous. Non-verbal Communication– uses other forms, such as gestures or facial expressions, and touch. 1. PersonalAppearance When the symbolic meaning of an object is unfamiliar the nurse can inquire about its significance, which may foster rapport with the client. How a person dresses is often an indicator of how person feels. E.g. For acutely ill clients n hospital or home care settings, a change in grooming habits may signal that the client is feeling better. A man may request a shave, or a woman may request a shampoo and some makeup. 2. Posture and Gait
- 3. The ways people walk and carry themselves are often reliable indicators of self-concept, current mood, and health. Erect posture and an active, purposeful stride suggest a feeling of well being. Slouched posture and slow, shuffling gait suggest depression or physical discomfort. The nurse clarifies the meaning of the observed behavior, e.g. “You look like it really hurts you to move. I’m wondering how your pain is and if you might need something to make you more comfortable?” 3. Facial Expression No part of the body is as expressive as the face Although he face may express the person’s genuine emotions, it is also possible to control these muscles so the emotion expresses does not reflect what the person is feeling. When the message is not clear, it is important to get feedback to be sure of the intent of expression. Nurses need to be aware of their own expressions and what they are communicating to others. It is impossible to control all facial expression, but the nurse must learn to control expressions of feelings such as fear or disgust in some circumstances. Eye contact is another essential element of facial communication 4. Gesture Hand and body gestures may emphasize and clarify the spoken word, or they may occur without words to indicate a particular feeling or give a sign Electronic Communication– many health care agencies are moving toward electronic medical records where nurses document their assessments and nursing care. E-mail Most common form of electronic communication. Advantage: It is fast, efficient way to communicate and it is legible. It provides a record of the date and time of the message that was sent or received. Disadvantage: risk of confidentiality When Not to Use Email: a. When information is urgent b. Highly confidential information (e.g. HIV status,mental health, chemical dependency) c. Abnormal lab data Agencies usually develop standards and guidelines in use of e-mail Factors Influencing the Communication Process 1. Development Language, psychosocial, and intellectual development move through stages across the lifespan. 2. Gender Girls tend to use language to seek confirmation, minimize differences,and establish intimacy. Boys use language to establish independence and negotiate status within a group. 3. Values and Perception Values are the standards that influence behavior, and perceptions are the personal view of event. 4. PersonalSpace Personalspace is the distance people prefer in interactions with others. Proxemics is the study of distance between people in their interactions Communication 4 distances: a. Intimate: Touching to 1 ½ b. Personal: 1 ½ to 4 feet
- 4. c. Social: 4 to 12 feet d. Public: 12 to 15 feet 5. Territoriality Is a concept of the space and things that an individual considers as belonging to the self 6. Roles and Relationships Choice of words, sentence structure,and tone of voice vary considerably from role to role. (E.g. nursing student to instructor, client and primary care provider, or parent and child). 7. Environment People usually communicate most effectively in a comfortable environment. 8. Congruence The verbal and nonverbal aspects of message match. E.g.,when teaching a client how to care for a colostomy, the nurse might say, “You won’t have any problem with this.” However,if the nurse looks worried or disgusted while saying this, the client is less likely to trust the nurse’s words. 9. Interpersonal Attitudes Attitudes convey beliefs, thoughts, and feelings about people and events. Caring and warmth convey a feeling of emotional closeness Respect is an attitude that emphasizes the other person’s worth and individuality. A nurse coveys respect by listening open mindedly even if the nurse disagrees.Acceptance emphasizes neither approval nor disapproval .The nurse willingly receives the client’s honest feelings. COMMUNICATION IN NURSING Communication 1. Is the means to establish a helping-healing relationship. All behavior communication influences behavior. 2. Communication is essential to the nurse-patient relationship for the following reasons: 3. Is the vehicle for establishing a therapeutic relationship. 4. It the means by which an individual influences the behavior of another, which leads to the successful outcome of nursing intervention. Basic Elements ofthe Communication Process 1. Sender – is the person who encodes and delivers the message 2. Messages – is the content of the communication. It may contain verbal, nonverbal, and symbolic language. 3. Receiver – is the person who receives the decodes the message. 4. Feedback – is the message returned by the receiver. It indicates whether the meaning of the sender’s message was understood. Modes ofCommunication 1. Verbal Communication – use of spoken or written words. 2. Nonverbal Communication – use of gestures,facial expressions, posture/gait, body movements, physical appearance and body language Characteristics ofGood Communication 1. Simplicity – includes uses of commonly understood, brevity, and completeness.
- 5. 2. Clarity – involves saying what is meant. The nurse should also need to speak slowly and enunciate words well. 3. Timing and Relevance – requires choice of appropriate time and consideration of the client’s interest and concerns. Ask one question at a time and wait for an answer before making another comment. 4. Adaptability – Involves adjustments on what the nurse says and how it is said depending on the moods and behavior of the client. 5. Credibility – Means worthiness of belief. To become credible, the nurse requires adequate knowledge about the topic being discussed. The nurse should be able to provide accurate information, to convey confidence and certainly in what she says. Communicating With Clients Who Have Special Needs 1. Clients who cannot speak clearly (aphasia, dysarthria, muteness) a. Listen attentively, be patient, and do not interrupt. b. Ask simple question that require “yes” and “no” answers. c. Allow time for understanding and response. d. Use visual cues (e.g.,words, pictures, and objects) e. Allow only one person to speak at a time. f. Do not shout or speak too loudly. g. Use communication aid:Pad and felt-tipped pen, magic slate, pictures denoting basic needs, call bells or alarm. 2. Clients who are cognitively impaired a. Reduce environmental distractions while conversing. b. Get client’s attention prior to speaking c. Use simple sentences and avoid long explanation. d. Ask one question at a time e. Allow time for client to respond f. Be an attentive listener g. Include family and friends in conversations, especially in subjects known to client. 3. Client who are unresponsive a. Call client by name during interactions b. Communicate both verbally and by touch c. Speak to client as though he or she could hear d. Explain all procedures and sensations e. Provide orientation to person, place, and time f. Avoid talking about client to others in his or her presence g. Avoid saying things client should not hear 4. Communicating with hearing impaired client a. Establish a method of communication (pen/pencil and paper, sign-language) b. Pay attention to client’s non-verbal cues c. Decrease background noise such as television d. Always face the client when speaking e. It is also important to check the family as to how to communicate with the client f. It may be necessary to contact the appropriate department resource person for this type of disability 5. Client who do not speak English a. Speak to client in normal tone of voice (shouting may be interpreted as anger) b. Establish method for client o signal desire to communicate (call light or bell) c. Provide an interpreter (translator) as needed
- 6. d. Avoid using family members, especially children, as interpreters. e. Develop communication board, pictures or cards. f. Have dictionary (English/Spanish) available if client can read. Reports Are oral, written, or audiotape exchanges of information between caregivers. Common reports 1. Change-in-shift report 2. Telephone report 3. Telephone or verbal orders – only RN’s are allowed to accept telephone orders. 4. Transfer report 5. Incident report Documentation 1. Is anything written or printed that is relied on as record or proof for authorized person. 2. Nursing documentation must be: accurate comprehensive flexible enough to retrieve critical data, maintain continuity of care,track client outcomes, and reflects current standards of nursing practice 3. Effective documentation ensures continuity of care saves time and minimizes the risk of error. 4. As members of the health care team,nurses need to communicate information about clients accurately and in timely manner 5. If the care plan is not communicated to all members of the health care team,care can become fragmented, repetition of tasks occurs, and therapies may be delayed or omitted. 6. Data recorded,reported, or communicated to other health care professionals are CONFIDENTIAL and must be protected. Confidentiality 1. Nurses are legally and ethically obligated to keep information about clients confidential. 2. Nurses may not discuss a client’s examination, observation, conversation, or treatment with other clients or staff not involved in the client’s care. 3. Only staff directly involved in a specific client’s care has legitimate access to the record. 4. Clients frequently request copies of their medical record, and they have the right to read those records. 5. Nurses are responsible for protecting records from all unauthorized readers. 6. When nurses and other health care professionals have a legitimate reason to use records for data gathering, research,or continuing education, appropriate authorization must be obtained according to agency policy. 7. Maintaining confidentiality is an important aspect of profession behavior. 8. It is essential that the nurse safe-guard the client’ right to privacy by carefully protecting information of a sensitive, private nature. 9. Sharing personal information or gossiping about others violates nursing ethical codes and practice standards. 10. It sends the message that the nurse cannot be trusted and damages the interpersonal relationships. Guidelines ofQuality Documentation and Reporting 1. Factual a. A record must contain descriptive, objective information about what a nurse sees,hears,feels, and smells.
- 7. b. The use of vague terms, such as appears,seems,and apparently, is not acceptable because these words suggest that the nurse is stating an opinion. 1. Example:“The client seems anxious” (the phrase seems anxious is a conclusion without supported facts.) 2. Accurate a. The use of exact measurements establishes accuracy. (example: “Intake of 350 ml of water” is more accurate than “ the client drank an adequate amount of fluid” b. Documentation of concise data is clear and easy to understand. c. It is essential to avoid the use of unnecessary words and irrelevant details 3. Complete a. The information within a recorded entry or a report needs to be complete, containing appropriate and essential information. 1. Example:The client verbalizes sharp, throbbing pain localized along lateral side of right ankle, beginning approximately 15 minutes ago after twisting his foot on the stair. Client rates pain as 8 on a scale of 0-10. 4. Current a. Timely entries are essential in the client’s ongoing care. To increase accuracy and decrease unnecessary duplication, many healthcare agencies use records kept near the client’s bedside, which facilitate immediate documentation of information as it is collected from a client 5. Organized a. The nurse communicates information in a logical order. 1. Example: An organized note describes the client’s pain, nurse’s assessment, nurse’s interventions, and the client’s response Legal Guidelines for Recording 1. Draw single line through error, write word error above it and sign your name or initials. Then record note correctly. 2. Do not write retaliatory or critical comments about the client or care by other health care professionals. Enter only objective descriptions of client’s behavior; client’s comments should be quoted. 3. Correct all errors promptly Errors in recording can lead to errors in treatment Avoid rushing to complete charting, be sure information is accurate. 4. Do not leave blank spaces in nurse’s notes. Chart consecutively, line by line; if space is left, draw line horizontally through it and sign your name at end. 5. Record all entries legibly and in blank ink Never use pencil, felt pen. Blank ink is more legible when records are photocopied or transferred to microfilm. Legal Guidelines for Recording 6. If order is questioned, record that clarification was sought. If you perform orders known to be incorrect, you are just as liable for prosecution as the physician is. 7. Chart only for yourself Never chart for someone else. You are accountable for information you enter into chart. 8. Avoid using generalized, empty phrases such as “status unchanged” or “had good day”. Begin each entry with time, and end with your signature and title. Do not wait until end of shift to record important changes that occurred severalhours earlier. Be sure to sign each entry. 9. For computer documentation keep your password to yourself.
- 8. Maintain security and confidentiality. Once logged into the computer do not leave the computer screen unattended. References J.Q. Udan, RN, MAN 2004. Mastering Fundamentals of Nursing 2nd ed. Educational Publishing House Erbs & Kozier, Fundamentals of Nursing, 7th edition