Approach to anemia
•Transferir como PPTX, PDF•
30 gostaram•2,291 visualizações

this presentation includes a clinical approach to anemia .

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Approach to anemia
Semelhante a Approach to anemia (20)
Último
Último (20)
Approach to anemia
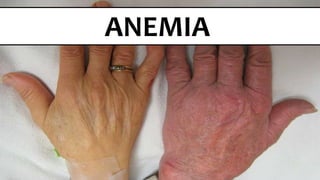
- 1. ANEMIA
- 11. DEFINITION ↓ RBCs Count Or Hb Content Or Packed red cell volume (HV)
- 12. ETIOLOGY
- 13. ↓ RBCs PRODUCTION Iron Folic acid Vit. B12 EPO Thyroxin Androgen
- 14. Aplastic anemiaSTEM CELLS Megaloblastic anemia Sideroblastic anemia ERYTHROBLASTS Myelodyplasia - Myelofibrosis - Tumor infiltration.INFILTRATION Drugs(chloramphenicol, sulphonamides, Carbimazole) Irradiation Chemotherapy SUPPRESSION
- 16. BLOODLOSS trauma, melena, hematemesis, menometrorrhagia OBVIOUS BLEEDING Slowly bleeding ulcer or carcinomaOCCULT BLEEDING repeated diagnostic testing , hemodialysis losses, excessive blood donation during surgical procedures IATROGENIC
- 18. DESTRUCTION
- 19. EXTRAVASCULAR DESTRUCTION OF RBCs INTRINSIC RED BLOOD CELL DEFECTS Enzyme deficiencies (eg, G6PD) Hemoglobinopathies (eg, sickle cell disease, thalassemias) Membrane defects (eg, hereditary spherocytosis) EXTRINSIC RED BLOOD CELL DEFECTS Liver disease Hypersplenism Infections (eg, malaria) Oxidant agents (eg, dapsone, nitrites, aniline dyes) Other agents (eg, lead, copper, snake and spider bites) Autoimmune hemolytic anemia (warm- or cold-reacting, drugs) IVIG infusion
- 20. INTRAVASCULARDESTRUCTION OF RBCs Microangiopathy (eg, aortic stenosis, prosthetic valve) Transfusion reactions (eg, ABO incompatibility) Infection (eg, severe malaria) Paroxysmal cold hemoglobinuria. Paroxysmal nocturnal hemoglobinuria IV infusion with hypotonic solutions
- 22. MICROCYTIC ANEMIA: MCV <80 FL Iron deficiency anemia Thalassemic disorders (# Globin) Anemia of inflammation/anemia of chronic disease (late) Sideroblastic anemia (eg, congenital, lead, alcohol, drugs; uncommon) (# Heme)
- 25. NORMOCYTIC ANEMIA (MCV 80 : 100 FL) Acute blood loss Iron deficiency anemia (early) Anemia of inflammation/anemia of chronic disease Bone marrow suppression (may also be macrocytic) Bone marrow invasion Aplastic anemia Chronic renal insufficiency Endocrine dysfunction (Hypothyroidism – Hypopituitarism)
- 26. MACROCYTIC ANEMIA: MCV >100 FL Alcohol abuse Folate deficiency Vitamin B12 deficiency Myelodysplastic syndromes Acute myeloid leukemias. Reticulocytosis (Hemolytic anemia - Response to blood loss - Response to appropriate hematinic (eg, iron, B12, folic acid) Drug-induced anemia (eg, Hydroxyurea, AZT, chemotherapeutics) Liver disease
- 31. MAJOR QUESTIONS? •Is the patient bleeding (now or in the past)? •Is there evidence for increased RBC destruction (hemolysis)? •Is the bone marrow suppressed? •Is the patient iron deficient? If so, why? •Is the patient deficient in folic acid or vitamin B12? If so, why?
- 32. Age, Gender, Race, Family history Menstrual history Dietary history Occupational history
- 34. Etiology (tarry stools - ulcer-type pain, R.A, R.F)? Urine color ? Stool (float – color ? – Bulk – offensive ? – easily flushed ?) Malabsorption Fever ? Drug history
- 36. B12 DEFICIENCY ? •Early greying of hair •Loss of proprioception ? •Sore tongue
- 39. Pallor (conjunctivae, nail beds, face, Palms) Jaundice Weight loss Lymphadenopathy Lower Limb edema Arthritis (Felty’s syndrome) GENERAL
- 40. Hypothyroidism Splenomegaly – hepatomegaly Bone tenderness (sternum- low back) Koilonychias Angular stomatitis - glossitis GENERAL
- 41. Ecchymosis. Piles. Early greying of hair (B12 ↓) Cardiac examination (enlarged – S3 – Murmur ?) GENERAL
- 44. CBC
- 45. CBC FemaleMale < 36 %< 41 %
- 46. CBC > 10080 - 100< 80 MacrocyticNormocyticMicrocytic Values in excess of 115 fL are almost exclusively seen in vitamin B12 or folic acid deficiency
- 48. CBC HighLow H.S. – SCA↓ MCV & MCH
- 50. CBC 0.5% to 2.5%
- 51. CBC Good BM response to Hemolysis or blood loss Anemia + Retics ↓ BM response e.g. Iron ↓ - Renal failure Stable anemia + ↓ Retics Aplastic crisis (Parvovirus B19) – BM failure Hemolytic anemia + ↓ Retics Aplastic anemia ↓ Retics + Pancytopenia Pure red cell aplasia ↓ Retics + Anemia + Normal platelets & WBCs
- 52. CBC neutrophils: Bacterial infection monocytes: myelodysplasia eosinophils: parasitic infections Anemia + Leucocytosis bone marrow suppression or replacement, hypersplenism, or deficiencies of B12 or folate Anemia + Leucopenia
- 53. CBC Bone marrow suppression or replacement, Hypersplenism, or Deficiencies of B12 or folate Anemia + Thrombocytopenia Infection Essential thrombocytosis Iron deficiency anemia Anemia + Thrombocytosis
- 55. CBC RDWNormal RDW Early iron, vitamin B12, or folate deficiency Dimorphic anemia (Iron & folate deficiency) Anemia of chronic disease Acute blood loss or hemolysis Anemia of renal disease Normocytes Iron deficiency Sickle cell-β-thalassemia Anemia of chronic disease Heterozygous thalassemiaMicrocytes Folate or vitamin B12 ↓ Aplastic anemia Chronic liver diseaseMacrocytes
- 56. BLOOD SMEAR
- 57. BONE MARROW EXAMINATION PANCYTOPENIA. PRESENCE OF ABNORMAL CELLS IN CIRCULATION, e.g. BLASTS. MEGALOBLASTIC ERYTHROPOIESIS (FOLATE OR B12 DEFICIENCY), ABSENCE OF RBC PRECURSORS (PURE RED CELL APLASIA)
- 67. CONDITION SERUM IRON TIBC FERRITIN COMMENT Iron deficiency ↓ ↑ ↓ Responsive to iron Chronic inflammation ↓ ↓ Unresponsive to iron Thalassemia major ↑ N N Reticulocytosis and indirect bilirubinemia Thalassemia minor N N - ↓ N fetal Hb & Hb A2, target cells Lead poisoning N N N Basophilic stippling of RBCs Sideroblastic anemia ↑ N Ring sideroblasts in marrow Hemoglobin N N N Hemoglobin electrophoresis
- 68. ↓ HB RETICS
- 70. ↓ HB BM