Presentation1.pptx, radiological imaging of lower limb ischemia.
•Transferir como PPTX, PDF•
75 gostaram•9,160 visualizações


Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Presentation1.pptx, radiological imaging of lower limb ischemia.
Semelhante a Presentation1.pptx, radiological imaging of lower limb ischemia. (20)
Mais de Abdellah Nazeer
Mais de Abdellah Nazeer (20)
Presentation1.pptx, radiological imaging of lower limb ischemia.
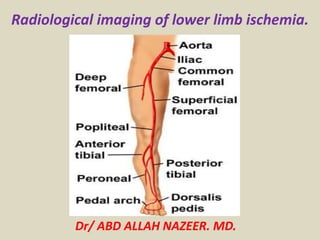
- 1. Radiological imaging of lower limb ischemia. Dr/ ABD ALLAH NAZEER. MD.
- 2. Acute limb ischemia is defined as “Any sudden decrease in limb perfusion causing a potential threat to limb viability”. By convention this usually refers to patients presenting with symptoms for less than 2 weeks. The spectrum of acute limb ischemia therefore ranges from the patient with a few hours history of a painful cold white leg, to the patient with a few days history of short distance claudication or the patient with a sudden increase in ischemic symptoms on a background of peripheral arterial disease. Acute limb ischemia. Pathophysiology An embolus is defined as a material (gas, solid or liquid) that is carried within the circulation and lodges in a blood vessel in another part of the circulation, causing occlusion of the blood vessel. Radiologically the upper border of an embolus is classically concave, known as the “meniscus” sign. Acute : varies but up to 2 weeks Chronic : > 2 weeks Acute on Chronic : Sudden and rapid deterioration in symptoms
- 3. Common etiologies 1. Embolic – Causes 15% of ALI cases • 80% from cardiac source - valve, mural thrombus • 20% non-cardiac source - thrombosed aneurysm, ulcerated atherosclerotic plaque • Decreasing incidence with fewer cases of rheumatic heart disease • Most commonly lodged at: Femoral artery bifurcation, aortoiliac arterial system, brachial artery • Unique condition = Blue Toe Syndrome -Sudden appearance of cool, painful foot with cyanosis/petechaie of toes and plantar foot - Paradoxically: normal pedal pulses - Etiology: emboli to the digital arteries of the foot - Management: Requires imaging for more proximal atherosclerotic lesion - Should consider popliteal artery aneurysm - Treatment: Antiocoagulation alone +/- surgical bypass of atherosclerotic lesion 2. Thrombotic – Causes 85% of ALI cases • Of native or aneurysmal artery • Most commonly located at: Bypass grant, common femoral artery, popliteal artery • Of indwelling bypass graft
- 4. Less common etiologies 1. Extrinsic compression of arterial lumen • Aortic or vascular dissection, creating pseudo lumen which compromises true lumen • Compartment syndrome • Thoracic outlet syndrome 2. Vasospasm • Raynaud’s disease - Vasospastic condition causing well-demarcated ischemia to fingers and toes - Three stages: Pallor (hypoperfusion), then cyanotic (hypoxemia), then hyperemia (reperfusion) - Usually bilateral limb involvement 3. Vasculitis • Buerger’s disease (Thromboangiitis obliterans) - Segmental, inflammatory vaso-occlusive disease of small and medium arteries -Heavy tobacco use is a significant risk factor -• Temporal arteritis (Giant cell arteritis) - Inflammatory condition of medium and large arteries • Takayasu’s arteritis - Chronic, inflammatory, large-vessel disease of aorta and its large branches -Predominantly found in young women (age 20-30) -4. Low intravascular volume +/- mild peripheral vascular disease (PVD) • Congestive heart failure, dehydration, sepsis 5. Trauma
- 5. Imaging options 1. Digital subtraction angiography (DSA) • Gold standard for limb ischemia imaging • Advantages: During angiography, may be able to immediately start therapeutic intervention (intra-arterial lysis) without losing time • Disadvantages: 8% incidence of contrast nephrotoxicity . - Relatively invasive 2. Duplex ultrasonography: • Ultrasound with color flow and Doppler waveform information regarding vascular flow and patency. • Advantages: - Noninvasive and non-nephrotoxic -Fairly accurate for infrainguinal arterial occlusive disease, especially of bypass grafts in this location • Disadvantages: - Time intensive (30-40 min) - Suprainguinal arterial occlusions and distal run-off vessels not well-visualized -Calcifications of arterial walls (in diabetic patients, especially) can create artifacts and obscure visualization. • Comparisons between duplex ultrasound versus angiography pre-operatively for chronic limb ischemia showed a high correlation rate between the two. • May be considered as a second-line approach to ALI imaging if angiography is not possible for infrainguinal arterial occlusion.
- 6. 3. CT angiography (CTA) • Advantages: - Noninvasive -Can concurrently evaluate for aortic dissection while looking at runoff vessels in the extremities. -Promising literature regarding usefulness in staging severity of chronic peripheral arterial disease (PAD): Sensitivity of CTA = 96% and specificity = 97% • Disadvantages: - Time intensive (30-40 min) -Exposure to IV contrast –> If going to angiography after CTA for intra-arterial lysis of clot, patient will now receive a 2nd contrast bolus, increasing the risk of renal failure. • Not well-studied in acute limb ischemia 4. MR angiography (MRA) • Advantages: - Less contrast load than angiography -Gadolinium IV contrast is safe for the kidneys -No ionizing irradiation • Disadvantages: - Very time intensive and often unavailable during weekend and night hours. -Promising literature regarding usefulness in staging severity of chronic PAD in the femoral/popliteal system:
- 9. Thrombosis or embolism at femoral artery. FA lumen is filled with hypoechoic thrombus or embolus . Normal flow in adjacent FV.
- 10. Occlusion of the CIA with reserved flow in IIA (blue) to supply flow to EIA(red).
- 11. Short occlusion of the mid-SFA(large arrow) with large collateral at both end of occlusion(small arrow).
- 13. Tardus et parvus = small amplitude + slow rising pulse
- 16. Color Doppler imaging: thrombosis of the left common iliac artery. Arteriography: severe stenosis of the left common iliac artery.
- 17. Complete occlusion of the aorta and proximal iliac arteries
- 20. Angio-imaging of the popliteal trifurcation before and after selective balloon embolectomy.
- 21. Thrombus of the left atrium with complete popliteal artery occlusion.
- 22. Angiogram showing bilateral occlusions of superficial femoral arteries in thighs. Collaterals arising from the profunda femoris artery can functionally bypass this occlusion.
- 23. Obstruction of the CFA with engorgement of the collateral vessels.
- 24. Acute thrombosis of the femoropopliteal and trifurcation vessels in an 84-year-old woman with an acutely cool right leg. The patient refused angiography. (a) Transverse CT angiographic image at the level of the adductor canal shows rounded filling defect in the right popliteal artery (arrow). The contralateral left popliteal artery (P) is patent at this level. (b) Large field of view multipath CPR and (c) enlarged image of popliteal region show the extent of right-sided thrombus (arrowheads). In addition to the popliteal artery (POP), the anterior tibial artery (AT), tibioperoneal trunk (TPT), and posterior tibial artery (PT) are occluded. F, femoral condyle. High-grade left popliteal stenosis (asterisk) is also noted.
- 25. No flow at the PT artery
- 26. Images of adventitial cystic disease in a 55-year-old patient. (a) Axial source image from peripheral CT angiography shows marked compression of the popliteal artery (P) by an ovoid fluid- density lesion (arrowheads). Note the predominant transverse compression of the flow lumen. F, fabella. (b) Corresponding sagittal thin- slab MIP image shows craniocaudal extent of fluid- density lesion in the popliteal arterial wall (arrowheads). (c) VR image viewed obliquely from the posterior direction demonstrates severe narrowing of the right popliteal artery (arrows).
- 27. CT Angiography. Digital Subtraction Angiography
- 28. CT angiography showing the presence of an intraluminal aortic (short arrow) and iliac (long arrow) saddle embolus.
- 29. CT angiography of the lower limbs showing distal posterior and anterior tibial artery occlusion of the left side and three-vessel occlusion of the right side.
- 30. Digital subtraction angiogram (DSA) illustrates a high-grade short- segment stenosis of the lumen of the right superficial femoral artery (a).
- 31. (MRA) of the lower extremities was obtained by using the bolus-chase technique. A short-segment high-grade stenosis is present in the middle of the left superficial femoral artery. Note the collateral arterial supply.
- 32. Occlusion of the left common femoral artery.
- 36. Acute right lower extremity pain and absent popliteal and pedal pulses. There is an occlusion of the popliteal artery caused by an embolus. Acute limb ischemia with occlusion of the SFA by embolus.
- 37. Occlusion of the popliteal artery caused by an embolus. Anterior tibial artery occluded proximally with limited contrast filing of ATA distally. The TPT and PTA are patent
- 39. Peripheral vascular disease, (chronic limb ischemia).
- 49. ABI Interpretation 1.00–1.29 Normal 0.91–0.99 Borderline 0.41–0.90 Mild-to-moderate disease ≤0.40 Severe disease ≥1.30 Non compressible Interpreting the Ankle-Brachial Index.
- 50. Segmental Pressures (mm Hg).
- 52. ABI in diabetics patient with calcification of vessel wall and beaded appearance of color flow.
- 53. Severe stenosis of the SFA with area of color flow disturbance and aliasing(Arrows).
- 54. Calcified atheroma of the SFA with drop-out of color flow signal in parts of the lumen.
- 55. This elderly male diabetic patient had severe pain in the right leg. Colour Doppler ultrasound and spectral Doppler tracing reveal severe diffuse stenotic disease of the arterial system starting from the right popliteal artery to the dorsalis pedis artery. This kind of a picture is seen in long-standing diabetes mellitus resulting in severe arterial disease or arteriopathy. The waveform of the arteries affected including the popliteal artery, the anterior and posterior tibial arteries show loss of tri-phasic spectral waveform which is replaced with spectral broadening and an almost venous like flow pattern. This is known as severe dampening of the waveform and this also known as tardus parvus flow.
- 61. Peripheral CT angiogram of a 62-year-old man with abdominal and bilateral common iliac artery aneurysms and subacute onset of right foot pain. (a) Oblique (45° left anterior oblique) MIP image of entire data set. Box indicates magnified views. (b–d) axial CT images through the right proximal calf show embolic filling defects in the anterior tibial artery (arrowheads) and the tibioperoneal trunk (arrows). (e,f) Corresponding CPR images from the popliteal artery through the anterior tibial artery (e) and posterior tibial artery (f) display intraluminal filling defects. DSA confirms CT angiography findings (g).
- 62. Peripheral CT angiogram in an 83-year-old man with right side–dominant calf and foot claudication. Acceptable image noise level in the abdomen and unprecedented spatial resolution down to the plantar arch and metatarsal branches. MIP of the entire data set (a); VR views of the abdomen (b) and right leg runoff (c–f) show distal aortic calcific plaque and patent renal arteries (b) occlusion of the right popliteal trifurcation with reconstitution of the peroneal artery (c), which reconstitutes the right posterior tibial artery above the ankle via a communicating branch (d), and supplies the foot through the common and lateral plantar arteries (e) which fill the plantar arch (f).
- 63. Peripheral CT angiography in a 72- year-old woman with non healing left forefoot ulcer. (a) VR image of the left superficial femoral artery shows excessive vessel wall calcifications, precluding the assessment of the flow channel. Cross-sectional views were required to visualize the vessel lumen. Axial CT images (b,c) through the mid-superficial femoral artery (dotted line in a and d) with viewing window settings (level/width) of 200 HU/600 HU (b) does not allow us to distinguish between opacified vessel lumen and vessel calcification, which can be distinguished only when an adequately wide window width (300 HU/1,200 HU) is used (c). Similar wide window settings are also used for a CPR through the same vessel (d), displaying several areas of wall calcification with and without stenosis.
- 64. Peripheral CT angiography (16 0.75 mm, 2.0 mm/1.0 mm) in a 73- year-old woman with intermittent claudication bilaterally. MIP (a) shows long right femoropopliteal occlusion (curved arrow) and diffuse disease of the left superficial femoral artery with a short distal near-occlusion. CPR (b) through left iliofemoral arteries demonstrates multiple mild stenosis of the external iliac artery (arrowheads), a diffusely diseased left superficial femoral artery, and short (3 cm) distal left superficial femoral artery occlusion. Corresponding selective DSA images of the left external iliac artery (c) and the distal left superficial femoral artery (d) were obtained immediately before angioplasty/stent implantation.
- 65. Peripheral CT angiography (16 0.75 mm, 2.0 mm/1.0 mm) of a diabetic male patient with bilateral claudication. MIP (a) shows arterial calcifications near the aortic bifurcation (arrow), as well as in the right (arrowheads) and left common femoral arteries, in the right femoropopliteal region, and in the crural vessels. A long stent is seen in the left femoropopliteal segment (curved arrow).Frontal view (b) and magnified 45° left anterior oblique (c) multipath CPR images provide simultaneous CPRs through the aorta and bilateral iliac through crural arteries. Note that prominent calcifications cause luminal narrowing in the proximal left common iliac artery (arrow) and in the right common femoral artery (arrowheads). The left common femoral artery is normal; the long femoropopliteal stent is patent (curved arrow). Mixed calcified and non calcified occlusion of the right distal femoral artery is also seen (open arrow).
- 66. Intermittent left leg claudication in a 62-year-old woman with a history of tobacco use and aortobifemoral bypass grafting. The ankle-brachial index was 0.65. (a– d) MIP images with bone segmentation; (e– h) DSA images obtained before treatment. (a) Oblique MIP image shows high- grade stenosis (arrows) at the origin of the left profunda femoris artery (P); a previously placed aortobifemoral graft (G) is noted, as is a patent superficial femoral artery (SFA). (b) Coronal MIP of the left thigh demonstrates multifocal moderate to severe stenosis in the SFA (arrowheads). The SFA is small in caliber with soft and calcified plaque present. (c) Coronal MIP of the calf shows a one- vessel runoff (peroneal; PER) to the left foot. Mild venous contamination (V) is present. (d) Sagittal MIP image of the left foot shows collateral vessel reconstitution (arrowheads) of the dorsalis pedis (DP) above the ankle from the peroneal artery. (e) DSA image from selective catheterization of the left profunda femoris artery corroborates the CT angiographic finding of high-grade profunda femoris artery (P) stenosis (arrows). (f) DSA image of left superficial femoral artery shows multiple focal stenoses (arrowheads) in the same segment of the superficial femoral artery as demonstrated by CT angiography. Note the lack of calcium visualization on the subtracted image from DSA. (g) DSA image of the calf confirms single peroneal vessel runoff. (h) DSA image of left foot confirms reconstitution of the dorsalis pedis artery (DP) from the peroneal artery (arrowheads).
- 67. Magnetic Resonance Angiography (MRA) show occlusion of the left CIA with filling of the SFA from collateral.
- 68. (MRA) of the lower extremities was obtained by using the bolus-chase technique. Atherosclerotic disease involves the bilateral superficial femoral arteries. Note the multiple lesions, which are primarily in the middle portions, and the large collateral arterial supply.
- 69. 67-year-old man with more than 10-year history of diabetes mellitus presented with symptoms of limb ischemia.
- 70. Thank You.