Presentation1.pptx. radiological imaging of bronchogenic carcinom.
•Transferir como PPTX, PDF•
38 gostaram•6,217 visualizações


Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Presentation1.pptx. radiological imaging of bronchogenic carcinom.
Semelhante a Presentation1.pptx. radiological imaging of bronchogenic carcinom. (20)
Mais de Abdellah Nazeer
Mais de Abdellah Nazeer (20)
Último
Último (20)
Presentation1.pptx. radiological imaging of bronchogenic carcinom.
- 1. Radiological imaging of bronchogenic carcinoma. Dr/ ABD ALLAH NAZEER. MD.
- 2. Bronchogenic carcinoma, (or frequently known as lung cancer) is the most common cause of cancer in men, and the 6th most frequent cancer in women worldwide. It is the leading cause of cancer mortality worldwide in both men and women and accounts for approximately 20% of all cancer deaths. Epidemiology. The major risk factor is cigarette smoking which is implicated in 90% of cases. Other risk factors include radon, asbestos, uranium, arsenic, chromium, COPD and lung fibrosis. Nearly 90% of lung cancer are related to smoking. 226,000 are newly diagnosed: 160,000 die of lung cancer per year. The average 5 years is > 15% survival. Introduction.
- 9. Squamous and adenocarcinoma have about the same 5-year survival probability. It is worse for large cell carcinoma, and oat cell carcinoma has almost no 5-year survival probability with a mean lifespan of months from the time of diagnosis. Overall 8% of lung cancer cases live past 5 years. Squamous (epidermoid) carcinoma derived from reserve cells that differentiate into squamous cells. Most commonly found centrally in the lung, usually in the major lobar or first segmental bronchus. Growth of the tumour occurs distally and proximally from site of origin, destroying normal tissue and structures. Squamous carcinomas tend to grow very large, and may kill by local growth. These tumours often cavitate and resemble abscesses on radiographic studies grossly. The tumour may be surgically resected but cure rate depends on the clinical stage at the time of diagnosis. Early diagnosis is possible by cytologic examination of a sputum sample.
- 10. Adenocarcinoma: Most adenocarcinoma are insidious and asymptomatic for a long time. Adenocarcinoma tend to occur more peripherally in the lung. Adenocarcinoma is the one cell type of primary lung tumour that occurs more often in nonsmokers. Treatment is surgical and involves removal of the entire lobe with associated lymph nodes.. Bronchiolo-alveolar carcinoma A subtype of adenocarcinoma. The tumour grows on the underlying supportive structure of the lung parenchyma without causing much damage to that structure. A rapid ‘pneumonic’ spread occurs to other areas of the lung. Thus, on CXR it resembles a pneumonia-like infiltrate rather than a mass. Small cell carcinoma (‘oat cell’ carcinoma) A highly malignant form of ‘neuroendocrine’ tumour. Derived from reserve cells, differentiate towards neuroendocrine (Kulchitsky) cells. Occur almost exclusively in smokers.
- 11. Often associated with paraneoplastic syndromes e.g. hormonal effects - Ectopic ACTH production - Inappropriate ADH secretion. Small cell carcinomas arise centrally and tends to spread diffusely along and into the bronchial wall. Extensive necrosis within the tumour is common due to its rapid growth outgrowing the blood supply. Small cell carcinomas are not generally considered resectable cancers since dissemination is likely to have occured by the time they are discovered. They are responsive to chemotherapy. Radiotherapy is also useful, but they are rarely curable. Large Cell Carcinoma Carcinomas which are so poorly differentiated that by routine light microscopy they cannot be placed into either the epidermoid or glandular groups. Ultrastructurally, however, these tumours frequently demonstrate features of either epidermoid cells or glandular cells or both. Arise centrally in lung. Highly aggressive tumours.
- 12. Spread of lung carcinoma Local. Lymphogenic to regional lymph nodes: - hilar, mediastinal, supraclavicular. Hematogenous: Adrenal glands, brain, bones, liver. Local infiltration Bronchial obstruction ⇒ pneumonia, atelectasis, bronchiectasis distal to obstruction. Infiltration of lung parenchyma, pleura, pericardium, chest wall, vertebrae. Infiltration of superior vena cava ⇒ SVC syndrome (swelling of face, fullness of neck veins). Apical tumours may infiltrate: -Cervical sympathetic nerves ⇒ Horner’s syndrome (ptosis, miosis, anhydrosis on same side of lesion). -Brachial plexus ⇒ Pancoast syndrome (neurological manifestations e.g. pain in upper extremity).
- 21. New T-staging according to the 7th edition of the TNM-staging of lung cancer
- 26. Stage I Non-Small Cell Lung Cancer. Cancer is found only in the lung, usually less than 3 cm and not invading the bronchi. Surgical removal recommended. Radiation therapy and/or chemotherapy may also be used.
- 27. Stage II Non-Small Cell Lung Cancer. The cancer has spread to lymph nodes in the lung, more than 3 cm, reaching pleura or bronchi, but away from carina more 2 cm. Treatment is surgery to remove the tumor and nearby lymph nodes. Chemotherapy recommended; radiation therapy sometimes given after chemotherapy.
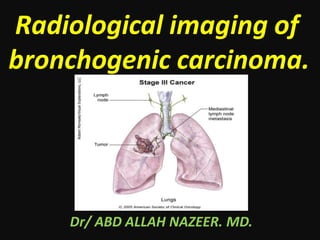
- 28. Stage III Non-Small Cell Lung Cancer. The cancer has spread to the lymph nodes located in the center of the chest, outside the lung . Stage IIIA cancer has spread to lymph nodes in the chest, on the same side where the cancer originated. Stage IIIB cancer has spread to lymph nodes on the opposite side of the chest, under the collarbone, or the pleura (lining of the chest cavity). Surgery or radiation therapy with chemotherapy recommended for stage IIIA . Chemotherapy and sometimes radiation therapy recommended for stage IIIB.
- 29. Stage IV Non-Small Cell Lung Cancer. The cancer has spread to different lobes of the lung or to other organs, such as the brain, bones, and liver. Stage IV non-small cell lung cancer is treated with chemotherapy.
- 30. Small Cell Lung Cancer–All Stages. Patients with limited stage (confined to one area of the chest) small cell lung cancer are treated with simultaneous radiation therapy and chemotherapy. Patients with extensive stage (not confined to one area of the chest) small cell lung cancer are treated with chemotherapy only. Because small cell lung cancer can spread to the brain, preventative radiation therapy to the brain is routinely recommended to all patients whose tumors disappear following chemotherapy and radiation therapy.
- 38. Left upper lobe bronchogenic carcinoma.
- 39. Peripheral bronchogenic carcinoma(T1 tumour).
- 40. T1 tumor.
- 41. T2 tumor
- 42. Adenocarcinoma in a 41-year-old man with right shoulder pain for several months. (a) Apical lordotic chest radiograph demonstrates a right apical mass with poorly marginated borders. (b) Chest CT scan (lung window) shows a homogeneous peripheral right upper lobe mass with irregular borders. There is tumor involvement of a posterior rib (arrow).
- 47. Undifferentiated large cell carcinoma.
- 49. Central lung cancer and atelectasis.
- 50. T3 tumor with invasion of the chest wall.
- 51. T4 tumor with invasion of the mediastinum.
- 52. T4 tumor constricting the right pulmonary artery (blue arrow)
- 53. Pancoast tumor in the right upper lobe with displacement of the superior mediastinum and trachea.
- 54. T4N2-tumor
- 56. Chest wall invasion. MRI advantages. Multiplanar imaging. Can differentiate tumor tissue from chest wall muscles. Cine MRI during breathing can assess the tumor movement against the pleural surface. In Pancoast’s tumors, MR can assess invasion of the brachial plexus and subclavian vessels. The accuracy of MRI versus CT in this domain in 94% for MRI compared to 63% for CT.
- 58. Pancoast tumor
- 60. Peripheral bronchogenic carcinoma with positive axillary and mediastinal nodes by PET Scan.
- 62. Pulmonary lymphoma refers to lung parenchymal involvement with lymphoma. It can be broadly divided as primary or secondary. primary pulmonary lymphoma - (rare) usually non- Hodgkin lymphoma which is limited to the lung with or without mediastinal lymph node involvement and with no evidence of extrathoracic dissemination for at least 3 months after the initial diagnosis. low-grade B-cell lymphoma (MALToma) – commonest 80% of primary pulmonary lymphoma high grade B-cell lymphoma - most commonly B-cell, occasionally anaplastic and peripheral T-cell types primary pulmonary plasmacytoma (rare)pulmonary intravascular lymphoma (rare) angiocentric immunoproliferative lesion (lymphomatoid granulomatosis) secondary pulmonary lymphoma - relatively common Hodgkin disease, non-Hodgkin lymphoma Two additional categories have also been described which include lymphoma in patients with post-transplant lymphoproliferative disorders (PTLD) AIDS-related pulmonary lymphoma (ARL - ARPL).
- 63. Radiographic features HRCT - chest A number of features may be present on HRCT which include, a mass or mass-like consolidation greater than 1 cm with or without cavitations or bronchograms - most common finding according to one study masses of pleural origin nodules less than 1 cm alveolar or interstitial infiltrates peribronchial or perivascular thickening with or without atelectasis pleural effusions, hilar or mediastinal lymphadenopathy Pulmonary lymphoma in immune compromised patient.
- 64. Pulmonary metastases are common and the result of metastatic spread to the lungs from a variety of tumours. Spread can occur via blood, or lymphatics. The remainder of this article concerns itself with hematogenous pulmonary metastases. Lymphangitis carcinomatosis is discussed separately. Pulmonary metastases from testicular cancer.