Presentation1.pptx, imaging modalities of intra cerebral lymphoma.
•Transferir como PPTX, PDF•
34 gostaram•3,053 visualizações


Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Presentation1.pptx, imaging modalities of intra cerebral lymphoma.
Semelhante a Presentation1.pptx, imaging modalities of intra cerebral lymphoma. (20)
Mais de Abdellah Nazeer
Mais de Abdellah Nazeer (20)
Último
Último (20)
Presentation1.pptx, imaging modalities of intra cerebral lymphoma.
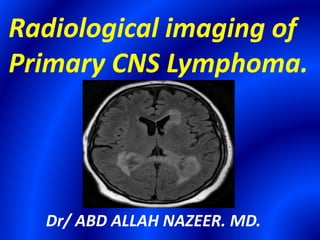
- 1. Radiological imaging of Primary CNS Lymphoma. Dr/ ABD ALLAH NAZEER. MD.
- 2. Primary CNS Lymphoma (PCNSL) refers to the isolated involvement of the craniospinal axis in the absence of primary tumor elsewhere in the body. Facts about Primary CNS lymphoma. 1)1%-5% of all brain tumors. 2)1% of all Non Hodgkin's Lymphoma (NHLs). 3)Incidence increasing in immunocompetent patients. 4)Most are Diffuse Large B-cell Lymphoma (DLBCLs) 5)Hodgkin's - 0.5%. 6)Metastatic CNS lymphoma, B-cell type - 5-9%. 7)Primary T-cell lymphoma of the CNS- CSF usually negative. Etiology: Precise etiology not known as CNS devoid of lymphatics, lymphocytes
- 3. Risk increases in patients with. 1)Autoimmune diseases like Sjögren syndrome, and systemic lupus erythematosus. 2)Viruses: Epstein-Barr virus (10-15%) and HIV/AIDS (Patients on HAART in later stage of disease). 3)Congenital immunodeficiency syndromes. 4)Severe immunosuppression (chemotherapy, long-term steroids).
- 4. Imaging findings OR Procedure details. Typical Appearance in Immunocompetent Patients: Imaging Characteristics: 1)Usually solitary mass( 40-60%) hyperdense on CT with no hemorrhage, necrosis or calcification. 2)Intermediate to low signal intensity on T1W images. 3)Isointense or hypointense signal relative to the gray matter on T2W images. 4)Restricted Diffusion with intense homogeneous post-contrast enhancement . Location: Supratentorial frontoparietal white matter, Periventricular regions , Deep gray nuclei and Corpus callosum (Common) Posterior fossa, Hypothalamus, Infundibulum and Pituitary gland (Uncommon). Primary dura-based lymphomas (Rare).
- 5. Unsual Findings, especially in Immuno-compromised Patients: Multiplicity . Hemorrhage. Lack of enhancement. Necrosis. Calcification. Atypical location. Age Group. IMMUNOCOMPETENT IMMUNOCOMPROMISED Age (Mean) 60 yrs. 30 yrs. Multiple lesions 30-50%. 63-81%. Necrotic change Rare. Common. CT Density. Hyperdense. Hyperdense. Enhancement . Homogenous Heterogeneous. MR Imaging. T1 signal . Iso-Hypo. Iso-Hypo. T2 signal . Iso- Hypo. Iso-Hypo. Enhancement. Homogenous. Heterogeneous.
- 6. PCNSL - Advanced techniques. Perfusion: Low relative Cerebral Blood Volume (rCBV). MR Spectroscopy (MRS) : High Cho/Cr ratio, low NAA, high lipid pea. PET: Increased uptake of DG/methionine. Primary CNS lymphoma subtypes. 1) Intravascular(Angiocentric)lymphoma . Small/medium-sized vessels filled with tumor. Multiple T2/FLAIR hyperintensities with linear/punctate enhancement oriented along perivascular spaces. 2) Lymphomatosis cerebri . Middle-aged or elderly with rapidly progressive dementia and ataxia. Patchy and confluent T2/FLAIR hyperintensities with no enhancement.
- 7. Typical Appearance in Immunocompetent Patients(B-Cell Type). Imaging Characteristics: 1)Usually solitary mass( 40-60%) hyperdense on CT with no hemorrhage, necrosis or calcification. 2)Intermediate to low signal intensity on T1W images. 3)Isointense or hypointense signal relative to the gray matter on T2W images. 4)Restricted Diffusion with intense homogeneous post-contrast enhancement. Location: Supratentorial frontoparietal white matter, Periventricular regions , Deep gray nuclei and Corpus callosum (Common). Posterior fossa, Hypothalamus , Infundibulum and Pituitary gland (Uncommon) Primary dura-based lymphomas(Rare). Imaging findings.
- 20. Multiplicity of Primary CNS Lymphoma(immunocompromized)
- 24. Atypical Appearance and Location of Lymphoma(Follow-up Study)
- 40. Differential Diagnosis: 1)Glioblastoma multiforme (GBM):Relatively homogeneous and strong enhancement in immunocompetent patients with PCNSL while peripheral irregular ring with central nonenhancing necrosis is more typical of GBM. Hemorrhage and necrosis are rare in PCNSL. 2)Metastasis: Second most common differential diagnosis of PCNSL especially hyperdense metastasis from Renal Cell Carcinoma or Mucinous primary. Metastasis are hyperperfused with high rCBV 3)High Grade Glioma: Hyperperfused with heterogeneous enhancement. 4)Progressive multifocal leukoencephalopathy (PML): a) Large multifocal asymmetric predominantly white matter non- enhancing lesions extending to involve the subcortical U-fibers b) Absent mass effect with restricted diffusion along the advancing edge of demyelination. c) Increase Cho levels with increase in mI suggestive of PML.
- 41. 5)Toxoplasmosis: especially in Immumocompromised patients. a)Solitary ring-enhancing lesion in an HIV/AIDS patient, most often lymphoma. b)Multiple lesions are characteristic of toxoplasmosis. c)Toxoplasmosis is hypometabolic on PET. d)MRS: Important lipid peak. NAA. Cho, Cr & mI nearly absent. 6) Immune reconstitution inflammatory syndrome( IRIS): Immune reconstitution inflammatory syndrome (IRIS) occur days to weeks after commencing patient on highly active anti-retroviral therapy (HAART) Bizarre-looking parenchymal masses and progressively enlarging enhancing lesions are typical of IRIS. 7)Lymphomatoid granulomatosis and PTLD in transplant patients.
- 44. Conclusion. 1)Once a rare neoplasm; PCNSL is now amongst the common CNS tumors. 2) Increasing incidence in immunocompetent individuals noted. 3) Contrast enhanced MR with diffusion weighted is modality of choice. 4) Advanced imaging techniques have a definite role as problem solving tool in PCNLS, especially in cases with unusual imaging characteristics and location.
- 45. Thank You.