
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Desquamative gingivitis
Semelhante a Desquamative gingivitis (20)
Último
Último (20)
Desquamative gingivitis
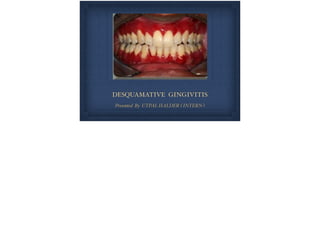
- 1. DESQUAMATIVE GINGIVITIS Presented By UTPAL HALDER ( INTERN )
- 2. Differential diagnosis is not easy as all oral mucosa lesion are the same , with short lived bullous vesicles which burst , causing ulcerations . Hence the name desquamative gingivitis
- 3. Etiology . Certain dermatoses . Hormonal influences .Abnormal responses to the irritation . Chronic infections . Idiopathic
- 4. Chronic Desquamative Gingivitis . Chronic desquamative gingivitis is characterised by intense redness and desquamative of the surface epithelium the attached gingiva . Clinical features of desquamative gingivitis vary in severity . Mild form . Moderate form . Severe form
- 5. . Erythema Mild form : . Painless .Age 17 - 23 years . Common in females
- 6. Moderate form : . Patchy distribution of bright red and grey areas . . Surface is smooth and shiny and soft in consistency . . Slight pitting on pressure . Nicolsky’s sign positive . Remainder of the mucosa is also extremely Smooth and shiny .Age : 30 - 40 years . . ℅ of burning sensation and sensitivity to the thermal changes .
- 7. Severe form : . Scattered , irregularly shaped areas - striking red appearance. .Areas is greyish blue giving an overall speckled appearance . . Surface epithelium - shredded and friable and can be peeled off in small patches . . Patient cannot tolerate coarse food , condiments and temperature changes . . Constant dry and burning sensation throughout the oral cavity .
- 8. Systemic approach to diagnosis of Desquamative gingivitis . Clinical History . . Clinical Examination . . Biopsy . . Microscopic Examination . Immunoflouroscence . 1. Direct & Indirect
- 9. Diseases clinically presenting as Desquamative Gingivitis ORAL LICHEN PLANUS Chronic inflammatory disease that affects skin and mucous membrane . . Wilson - 1869
- 10. Epidemiology . Prevalence : 1.5% . Women > Men . Predominant in adults > 40 years
- 11. Pathogenesis : . Current data suggest that OLP is a T cell - mediated autoimmune disease in which auto - cytotoxic CD8+ T cell trigger apoptosis of oral epithelial cells . . However , the precise cause of OLP is unknown .
- 12. Clinical features The skin lesion of OLP appears as small , angular , flat topped papule .
- 13. ORAL LESIONS : . Oral lichen planus presents as white striations , white papule , white plaques , erythema , erosions or blisters . . Presents in a variety of forms : 1. Reticular . 2.Atrophic . 3. Papular . 4. Ulcerative 5. Bullous Forms .
- 15. Plaque like Lichen Planus : Slightly raised or flat white area on the oral mucous membrane . Plaque type lesions may clinically similar to Homogenous Leukoplakia .
- 16. Erosive Lesions : These extensive erythematous areas with a patchy distribution may present as focal or diffuse hemorrhagic areas .
- 17. Vesicular or Bullous lesions : These lesions are raised , fluid - filled and are uncommon . Short lived on the gingiva , quickly rupturing and leaving an ulceration. Atrophic lesions : Atrophy of the gingival tissues with ensuing epithelial thinning results in erythema coffined to the gingiva .
- 18. Histopathology : Biopsy from the gingival lesions shows hyperkeratosis and mild hypergranulosis . Focal basal cell degeneration, lymphocytic exocytosis and thickening of basement membrane are apparent . The rate pegs exhibited a slight serrated configuration .
- 19. IMMUNOPATHOLOGY DI - Linear fibrillar deposits of fibrin in the basement membrane zone . Scattered immunoglobulin - staining cytoid bodies in the upper areas of the lamina propria . . Serum tests using indirect Immunofluorescence are negative in lichen planus .
- 20. Differential Diagnosis : . Lupus erythematous . Lichenoid reaction . Cicatrical pemphigoid . Chronic ulcerative stomatitis . Pemphigus vulgaris . Leukoplakia
- 21. TREATMENT : . The keratotic lesions of oral lichen planus are asymptomatic and do not require treatment . . The erosive , bullous , or ulcerative lesions of oral lichen planus are treated with high-potency topical steroid such as 0.05% fluocinonide ointment ( three times daily ) . . It can also be mixed 1:1 with carboxymethyl cellulose ( Orabase ) paste or other adhesive ointment . . SEVERE CASES - Intralesional injections of triamcinolone acetonide ( 10-20 mg ) or short term regimens of 40 mg prednisone daily for 5 days followed by 10 to 20 mg daily for an additional 2 weeks .
- 22. PEMPHIGOID : 2. Cicatrical / mucous membrane pemphigoid . Types of pemphigoid that are as follows : 1. Bullous pemphigoid . 3.Antiepiligrin pemphigoid . Hippocrates was first to describe pemphigoid as a type of fever accompanied by blisters .
- 23. MUCOUS MEMBRANE PEMPHIGOID : Cicatrical pemphigoid : . Chronic , vesiculobullous , autoimmune disorder . It predominantly affects women in fifth decade of life . . The percentage of involvement is : . Oral mucosal bulls lesion : 85-90% . Occular lesions : 66% . Nasal lesions : 15-23% . Laryngeal involvement : 8- 12%
- 24. PATHOGENESIS : . The two major antigenic determinants for cicatrical pemphigoid are bullous pemphigoid 1& 2 ( BP1 &BP2 ) . Most cases of Cicatrical pemphigoid are the result of an immune response directed against BP2 and less commonly against BP1 and epiligrin .
- 25. CLINICAL FEATURES : . EXTRAORAL FEATURES : . Nasopharyngeal involvement is characterised by rupture of vesicles in nasal mucosa . . Dysphagia . . Dyspnea and laryngeal stenosis .
- 26. Occular Involvement : . Trichiasis . Entropion . .Ankyloblepharon . . Symblepharon .
- 27. ORAL MANIFESTATIONS : Vesiculo-bullous lesions are seen in gingiva . Severe erythema may remain for months .
- 28. HISTOPATHOLOGY : . Chronic inflammatory infiltrate . . Separation of epithelium and connective tissue . Sub epithelial vesiculation
- 29. IMMUNOFLUORESCENCE : Positive immunofluoresce nce . The main immunoreactants are IgG & C3 .
- 30. DIFFERENTIAL DIGNOSIS : 1. Bullous pemphigoid . 2. Bullous Lichen planus . 3. Pemphigus vulgaris .
- 31. TREATMENT : . Localized lesions : Fluocinonide ( 0.05% ) and clobetasol propionate ( 0.05% ) in an adhesive vehicle can be used three times a day for up to 6 months . . If occultar involvement exists , systemic corticosteroids are indicated . . When. Lesions do not respond to steroids , systemic Dapsone ( 4-4 diaminodiphenylsulfone ) has proven to be effective . SEVERE CASES : Intravenous immunoglobulins are another effective but expensive treatment option in high- risk patients
- 32. BULLOUS PEMPHIGOID : Chronic , autoimmune , sub epidermal blistering skin disease that rarely involves mucous membrane .
- 33. ORAL LESIONS : . Gingiva : Erythematous and Desquamate . Painful. . Nikolsky’s sign : Negative
- 34. HISTOPATHOLOGY : . No evidence of acantholysis . . Developing vesicles are sub epithelial rather than intraepithelial . . The epithelium separates from the underlying connective tissue at the basement membrane zone .
- 35. PEMPHIGUS VULGARIS : . Derived from Greek word pemphix ( bubble or blister ) . Pemphigus vulgaris is most common of pemphigus diseases, which also includes 1. P. foliaceous . 2. P. vegetens . 3. P. erythematous . . Pathogenesis : Circulating autoantibodies are responsible for disruption of Intercellular junctions and loss of cell to cell adhesion .
- 36. CLINICAL FEATURES : 1. Bullae . 2. Erosion . 3. Ulcers . 4. Nikolsky test is positive .
- 37. HISTOPATHOLOGY : Typical intraepithelial clefting with ‘Tombstone’ appearance of basal cells , which remain attached to Subjacent basement membrane and fibrous connective tissue . Acantholysis of epithelial cells with formation of “ Tzanck cells “ is seen in the intraepithelial cleft .
- 38. IMMUNOFLUORESCENCE : Direct immunofluorescence of oral pemphigus . Positive intercellular signal for immunoglobulin G ( IgG ) deposits is seen in keratinocytes of the stratified squamous epithelium .
- 39. DIFFERENTIAL DIAGNOSIS : 1. Pemphigoid . 2. Lichen planus . 3. Linear IgA disease . 4. Chronic ulcerative stomatitis .
- 40. CHRONIC ULCERATIVE STOMATITIS : . Condition presents with chronic oral ulcerations . Predilection for women ( 4th decade ) . Erosions and ulcerations in oral cavity - few cases with cutaneous lesions .
- 41. ORAL LESIONS : Painful , solitary , small blisters and erosions with surrounding erythema - mainly on gingiva and lateral border of the tongue : hard palate may also present similar lesions .
- 42. HISTOPATHOLOGY : . Hyperkeratosis , acanthosis , and liquefaction of the basal layer areas of sub epithelial clefting . . Underlyng lamina propia - lumphohistiocytic chronic infiltrate in a band like configuration .
- 43. IMMUNOFLUORESCENCE : Direct Immunofluorescence of chronic ulcerative stomatitis . Nuclear deposits of IgG are prominent in the basal cell layer and fade toward the superficial layers .
- 44. DIAGNOSIS : Direct and indirect immunofluorescence required to arrive at correct diagnosis . TREATMENT : Mild cases : Topical steroids ( flucononide , clobetasol propionate ) and topical tetracycline . Severe cases : Systemic steroids . Hydroxychloroquinine sulphate 200-400 mg/day .
- 45. LINEAR IgA DISEASE : Uncommon mucocutaneous disorder with predilection in women . CLINICAL FEATURES : Pruritic vesiculobullous rash during middle to late age . Plaques or crops with an annular presentation surrounded by a peripheral rim of blisters . Skin of upper and lower trunk , shoulders , groin and lower limbs - face and perineum may also be affected .
- 46. ORAL LESIONS : Mucosal - oral involvement - 50-100% of cases . Vesicles . . Erosive gingivitis / chelitis . . Hard and soft palate commonly affected - tonsillar pillars , buccal mucosa , tongue and gingiva . . Painfull ulcerations or erosions . Occasionally oral lesion only manifestation for several years before cutaneous lesions .
- 47. IMMUNOFLUORESCENCE : Linear deposits of IgA are observed at the epithelial tissue- connective tissue interface . Differential Diagnosis : 1. Erosive lichen planus . 2. Chronic ulcerative stomatitis . 3. Pemphigus vulgaris . 4. Bullous pemphigoid . 5. Lupus erythematosus .
- 48. TREATMENT : . Combination of Dapsone and Sulfones . . Small amount of Prednisone ( 10 - 30 mg/ day) can be added if the initial response is inadequate .
- 49. LUPUS ERYTHEMATOSUS : . It is an autoimmune disease with three different clinical presentations . . 1. Systemic Lupus Erythematosus . . 2 . Chronic Cutaneous Lupus Erythematosus . . 3 . Subacute Cutaneous Lupus Erythematosus .
- 50. SYSTEMIC LUPUS ERYTHEMATOSUS : 1. Females : Males - 10:1 2.Affects kidneys , skin and mucosa . 3. Fever , weight loss and arthritis . 4. Rash on malar area . 5. Oral lesions are present in up to 40% of patients .
- 51. CHRONIC CUTANEOUS LUPUS ERYTHEMATOSUS : Chronic cutaneous lupus erythematosus . Multiple facial lesions with irregular hyperpigmented borders , some of which exhibit central scarring with cutaneous atrophy . Other lesions consists of hyperpigmented cutaneous patches .
- 52. IMMUNOFLUORESCENCE : Direct immunofluorescence of the lesional tissue reveals immunoglobulins and C3 deposits at the dermal - epidermal junction of the lesional and perilesional tissue but not in the normal tissue . TREATMENT : . Topical and intralesional corticosteroids . . Systemic corticosteroids alone or in combination with other Immunosuppressive agents such as cyclophosphamide .Antimalarial drugs may topical or systemic retinoids may be beneficial . . Gold salts and cyclosporin .
- 53. ERYTHEMA MULTIFORME : .An acute bullous and or macular inflammatory mucocutaneous disease where a series of immunopathologic mechanisms occur . CLINICAL FEATURES : 1. Herpes simplex infections . 2. Mycoplasma infection . 3. Drug reactions : sulphonamides , penicillin’s , phenylbutazone and phenytoin . 4. Hemorrhagic crusting of the vermillion border of lips common .
- 54. 5 . Presence of crusting Important in arriving at diagnosis . 8. Lesions - so painful that chewing and swallowing is impaired 6. Target or iris lesions with central clearing 9. Erythema multiforme minor - lasts approx 4 weeks . 11. Stevens-Johnson syndrome - lasts month or longer . Involves skin , conjunctiva , oral mucosa and genitalia requiring more aggressive therapy . 7. Multiple , large , shallow , painful ulcers with an erythematous birders . 10. Moderate cutaneous and mucosal involvement .
- 55. ERYTHEMA MULTIFORME : Large , shallow and painful ulcers involving the labial and buccal mucosa . Hemorrhagic crusting of the mandibular vermilion border of the lips is observed .
- 56. HISTOPATHOLOGY : 1. Liquefaction degeneration of upper epithelium and intraepithelial micro-vesicles but without acantholysis . 2. Pseudoepitheliomatous hyperplasia and nearotic keratinocytes . 3. Degenerative changes in the basement membrane . 4. Dense inflammatory cell infiltrate at the junction of epithelium and lamina propria , which becomes indistinct . 5. Edema of the lamina propria . Vascular dilation and congestion are also present .
- 57. IMMUNOFLUORESCENCE : Negative in Erythema Multiforme . TREATMENT : . No specific treatment for Erythema Multiforme . . For mild symptoms , systemic and local anti histamines together with topical anesthetics and debridement of the lesions with an oxygenating agent are required . . In the patients with bullous or ulcerative lesions and severe symptoms , corticosteroids are considered the drug of choice .
- 58. THANK YOU