3. Vitamin D Deficiency
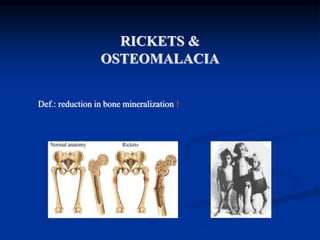
Osteomalacia & Rickets
Osteomalacia occurs in adults
Rickets occurs in children
Defective mineralization of the skeleton
4. VITAMIN D DEFICIENCY
Vitamin D deficiency leads to decreased absorptio
n of calcium by the GI tract.
As serum calcium starts to fall, secondary hyperpar
athyroidism occurs.
5. VITAMIN D DEFICIENCY
Elevated Pth levels may maintain serum calcium in
the normal range, but at the cost of phosphaturia,
hypophosphatemia and increased bone reabsorptio
n
Low serum phosphate results in inadequate bone
mineralization and osteopenia.
6. VITAMIN D DEFICIENCY
In severe cases, secondary hyperparathyroidism is
not adequate to maintain serum calcium levels, an
d hypocalcemia occurs.
7. OSTEOMALACIA,RICKETS
Regulation of Calcium & Phosphate Metabolism:
Peak bone mass at 16-25 years.
Bone loss 0.3- 0.5% per year (2-3% per year after 6th decade).
1. Parathyroid Hormone (PTH)
2. Vitamin D3
3. Calcitonin
4. Other Hormones: Est
rogen: Prevents bone loss
Corticosteroids: Increases bone loss
Thyroid hormones: Leads to osteoporosis
Growth hormones: Cause positive calcium balance
Growth factors
8. Biochemistry of Vitamin D3 – Bri
ef Review
Vitamin D3 (cholecalciferol) is synthesize
d in the skin, with UV light, from 7-dehy
drocholesterol
Vitamin D3 is hydroxylated twice – first i
n the liver, to 25-hydroxycholecalciferol, t
hen in the kidney, to 1, 25-dihydroxychol
ecalciferol, the most potent form of Vita
min D
9. Vitamin D (cont’)
Primary role of Vitamin D
Increase calcium and phosphate absorption from the
intestines
Other tissues that Vitamin D acts on
Parathyroid glands
Bone, Kidneys
Skin, Brain, Pituitary
Lymphocytes,Tumors
10. Other conditions that can cause Oste
omalacia
Hereditary or acquired disorders of vitamin D meta
bolism
Kidney failure and acidosis
Phosphate depletion associated with not enough ph
osphates in the diet
Cancer
Side effects of medications used to treat seizures (D
ilantin)
Liver disease
11. RICKETS, OSTEOMALACIA
PATHOLOGY:
Sufficient osteoid, poor mineralization
(Rickets is found only in children prior to the closure of the growt
h plates, while OSTEOMALACIA occurs in persons of any ag
e. Any child with rickets also has osteomalacia, while the rever
se is not necessarily true).
12. RICKETS, OSTEOMALACIA
CAUSES:
1. Nutritional deficiency
1. Vit D
2. chelators of calcium- phytates, oxalates, phosphorous
3. Antacid abuse, causing reduced dietary phosphate binding
2. GI Absorption defects
1. Post gastrectomy
2. Biliary disease (reduced absorption of Vitamins )
3. Small bowel disease
4. liver disease
3. Renal tubular defects
4. Renal osteodystrophy
5. Miscellaneous causes
13. Vitamin D Deficiency
Osteomalacia & Rickets (cont’)
Secondary to many things, including
Vitamin D deficiency as discussed above
Dietary calcium deficiency
Phosphorus deficiency
Aluminum toxicity
Hypophosphatasia
Fibrogenesis imperfecta ossium
14. Clinical features
Osteomalacia in adults starts insidiously as aches and pains in the lu
mbar (lower back) region and thighs, spreading later to the arms and
ribs.
Pain is non-radiating, symmetrical, and accompanied by tenderness i
n the involved bones.
Proximal muscles are weak, and there is difficulty in climbing up sta
irs and getting up from a squatting position.
Physical signs include deformities like and lordosis.
Pathologic fractures due to weight bearing may develop.
Most of the time, the only alleged symptom is chronic and bone ach
es are not spontaneous but only revealed by pressure or shocks.
15. RICKETS, OSTEOMALACIA
CLINICAL FEATURES:
Rickets - Tet
any , convulsions, failure to thrive, restles
sness, muscular flaccidity. Flattening of
skull (craniotabes), Thickening of wris
ts from epiphyseal overgrowth, Stunted growth,
Rickety rosary, spinal curvature, C
oxa vara, bowing, # of long bones
Osteomalacia, - Aches and pains, muscle weakness loss of hei
ght, stress #s.
16. Manifestations of Osteomalacia
Localized bone pain
Difficulty walking
Low back pain
Fractures are common, and delayed healing occu
rs
Muscular weakness
Weight loss
Progressive deformities of the spine (kyphosis)
17. Rickets, clinical manifestations
Skeletal findings:
1. Delay in closure of the fontanelles.
2. Parietal & frontal bossing.
3. Craniotabes ( soft skull bones).
4. Enlargement of the costochondral junction (rachitic rosary).
5. The development of Harrison sulcus ( caused by pull of the diaphragmatic attachments
to the lower ribs).
6. Enlargement of the wrist & bowing of the distal radius & ulna.
7. Progressive lateral bowing of the femur & tibia.
19. RICKETS, OSTEOMALACIA
XRAY FINDINGS:
OSTEOMALACIA
Loosers zones - incomplete str
ess # with healing lacking ca
lcium, on compression side
of long bones.
Codfish vertebrae due to press
ure of discs
Trefoil pelvis, due to indentatio
n of acetabulae stress #s
20.
21. Osteomalacia & Rickets – Clinica
l Manifestations
Asymptomatic at onset
Muscle weakness, especially of pe
lvic girdle
Bone pain
Atraumatic fractures
X-rays assist in diagnosis
22. RICKETS, OSTEOMALACIA
INVESTIGATIONS:
BLOOD TESTS Calci
um Reduced, Phosphate r
educed Alkalline Phosph
atase increased Urinary excretion of c
alcium diminished
Calcium phosphate products (= serum [Ca] x serum [PO4]) norm
ally 30. In rickets and osteomalacia is less than 24
23. Osteomalacia & Rickets - Diagno
sis
Other laboratory abnormalities may include
Hypocalcemia
Hypophosphatemia
Elevated serum alkaline phosphatase
24. Biochemical findings in rickets
Alkaline phosphatase usually is ↑in all forms of rickets.
Serum phosphorus concentrations usually are↓ in both hypocalcemic and hyp
ophosphatemic rickets.
Serum Ca is ↓only in hypocalcemic rickets.
Serum parathyroid hormone typically is ↑in hypocalcemic rickets, in contrast i
t is N in hypophosphatemic rickets.
25-OH vitamin D reflect the amount of vitamin D stored in the body, and is
↓in vit D deficiency.
1,25-OH2 vitamin D can be↓, N or ↑in hypocalcemic rickets and usually is N
or slightly ↑in hypophosphatemic rickets.
25. Osteomalacia & Rickets - Diagno
sis
Bone biopsy is diagnostic
Serum 25-hydroxycholecalciferol <50nmol/L in
dicates Vitamin D deficiency
26. OSTEOMALACIA:
EVALUATION
Careful diet and sunlight history
Renal function
Fecal fat determination
Anti IgA tissue transglutaminase antibodies.
Small bowel biopsy
27. RICKETS, OSTEOMALACIA
MANAGEMENT:
Depends on the cause
Nutritional Vitami
n D deficiency Dietary che
lators of calcium
Phytates
Oxalates Phospho
rus deficiency (unusual)
Antacid abuse
Treatment- vitamin D (50000u/w`/up to 3-12 w) and Calciu
m (1.5-2g/day)
28. RICKETS, OSTEOMALACIA
MANAGEMENT:
Depends on the cause
Gastro-intestinal absorption defects Po
st-gastrectomy Biliary
disease Enteric abs
orption defects
Short bowel syndrome
Rapid onset (gluten-sensitive enteropathy) Inflamm
atory bowel disease
Crohns
Celiac
29. RICKETS, OSTEOMALACIA
MANAGEMENT:
Depends on the cause
Renal tubular defects Vita
min D dependant
type I
type II
Treatment; High levels of vit D
Vitam
in D resistant (familial hypophosphatemic rickets)
Treatment; Phosphate 1-3 gm daily, Vit D3 high dose
Fanconi syndrome I, II, III R
enal tubular acidosis
30. Vitamin D Deficiency - Treatmen
t
50,000 IU of oral Vitamin D2, once or twic
e weekly for 6 – 12 w, followed by 1000 IU
/day
Appropriate exposure to sunlight
Phosphate and Calcium replacement, if nee
ded
Notas do Editor
Diffuse (not pinpointed to one location) bone pain, especially in the hips
Muscle weakness
Bone fractures that happen with very little trauma
Symptoms associated with low calcium including:
Numbness around the mouth
Numbness of extremities
Spasms of hands or feet
Abnormal heart rhythms