Fungemia in the Setting of Acute Lymphocytic Leukemia (FINAL)-1
1. TA M A R A B Y S T R A K
P H A R M D C A N D I D AT E
2 0 1 7
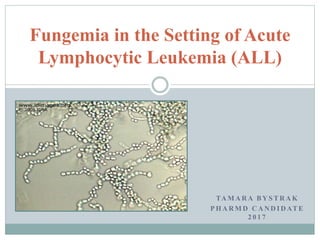
Fungemia in the Setting of Acute
Lymphocytic Leukemia (ALL)
2. Objectives
Evaluate a patient case
Understand the transition from empiric to organism
specific antifungal therapy
Learn about the increasing incidence of trichosporon
infection in immunocompromised patients
Review the mechanism of action, drug interactions,
pharmacokinetics, and adverse events related to treatment
with voriconazole
Apply voriconazole trough-based dosing to the patient
case
3. Initial
Presentation
A 6 y.o male patient with ALL on
protocol AALL1231 (Day 43 of
Delayed Intensification) admitted for
febrile neutropenia after receiving
vincristine
Wt: 20.5 kg
Induction chemotherapy:
Bortezomib1
Vincristine
Doxorubicin
IT methotrexate
Li J, Li Y, Huang B, Zheng D, Chen M, Zhou Z. Drug-induced modulation of T lymphocytes as a potential mechanism of susceptibility to infections in patients with
multiple myeloma during bortezomib therapy. Cell Biochem Biophys. 2015; 71(1):457-64.
11. Empiric Antifungal Treatment Plan
Amphotericin B (Liposomal)
6mg/kg/day IV
Non-aspergillus, non-candida fungal coverage
Micafungin
3mg/kg/day IV
Broad candida coverage
Cannot use an azole yet – worsens vincristine neurotoxicity via
inhibiting CYP3A4 metabolism1
van Schie RM, Brüggemann RJ, Hoogerbrugge PM, te Loo DM. Effect of azole antifungal therapy on vincristine toxicity in childhood acute
lymphoblastic leukaemia. J Antimicrob Chemother. 2011;66(8):1853-6.
12. Confirmed Fungemia
Cultures + for trichosporon spp.
Basidiomycetous yeast-like anamorphic organisms
Inhabit soil and colonize human skin/GI/resp tract
Can cause opportunistic infections, endocarditis, fungemia, or
hypersensitivity pneumonitis
38 species identified
Localized systemic as well as disseminated infections are frequently
T.asahii or T.mucoides
Second most common disseminating yeast in humans
Imaging shows cutaneous lesions in liver, kidney, and spleen
Disseminated trichosporon infection
Primary RF: Hematologic malignancy (63% of reported cases)
Additional risk factors: corticosteroid use, hemochromatosis, other
deficiencies of granulocyte function, HIV/AIDS, and ESRD
Maves RC. Medscape. Trichosporon infections. URL: http://emedicine.medscape.com/article/230705-overview [accessed 2016 Nov 16]
15. Iturrieta-González IA, Padovan AC, Bizerra FC, Hahn RC, Colombo AL. Multiple species of Trichosporon produce biofilms highly resistant to triazoles and amphotericin B. PLoS One.
2014;9(10):e109553.
Multiple Species of Trichosporon Produce Biofilms
Highly Resistant to Triazoles and Amphotericin B
Invasive infections caused by Trichosporon spp. have increased
considerably in recent years, especially in neutropenic and critically
ill patients using catheters and antibiotics
Trial tested n=54 clinical isolates of Trichosporon spp. obtained
from different patients between 2001 and 2010
T. asahii was the most frequent species identified (66.7%)
All species exhibited high adhesion and biofilm formation
capabilities, equal or greater to that of candida spp.
Limited sensitivity to antifungals due to incredibly resistant biofilm
producing cells
Triazoles are first line (voriconazole, fluconazole, itraconazole)
Voriconazole exhibited the best in vitro activity against all species
tested
16. Mitchell KF, Zarnowski R, Andes DR (2016) Fungal Super Glue: The Biofilm Matrix and Its Composition, Assembly, and Functions. PLoS Pathog 12(9): e1005828.
17. Head-to-Head Comparison of Inhibitory and Fungicidal Activities
of five triazoles against Trichosporon asahii
N=90 clinical isolates tested
Results suggest that azoles display
fungistatic activity (based on
MIC) but lack fungicidal effect
(based on MFC) against T. asahii
Killing activity is dose dependent
and occurred at concentrations not
reached in serum
Hazirolan G, Canton E, Sahin S, Arikan-Akdagli S. Head-to-head comparison of inhibitory and fungicidal activities of fluconazole, itraconazole, voriconazole, posaconazole, and
isavuconazole against clinical isolates of Trichosporon asahii. Antimicrob Agents Chemother. 2013;57(10):4841-7.
By rank order, the most active triazoles:
Voriconazole
Itraconazole,
Posaconazole,
Isavuconazole
Fluconazole
18. Trichosporin Specific Treatment
Start voriconazole
Literature supports efficacy of triazoles in Trichosporon spp.
Can give an azole now that vincristine is on hold
Patient cultures also show susceptibility
Weekly ultrasounds of liver/spleen to assess progression
D/C amphotericin and micafungin
Amphotericin B frequently displays inadequate fungicidal
activity and there have been cases of resistance reported
Echinocandins have no meaningful antifungal effect against
this genus
20. Azole
Antifungals
Mechanism of
Action (MOA)
• Competitively inhibits fungal cytochrome P-450
enzymes (14-sterol demethylase)
• Accumulation of 14-methylsterols
• Prevents ergosterol synthesis. Ergosterol is needed
in fungal cell membranes
https://www.studyblue.com/notes/note/n/anti-fungal/deck/5772604
DRUGDEX® System (electronic version). Voriconazole. Truven Health Analytics, Greenwood Village, Colorado, USA. Available at: http://www.micromedexsolutions.com/ (cited:
11/11/2016).
21. Voriconazole Dosing
1 mo. – 12 yr.
Patient = age 6
12+ yr
(NO phenytoin or
efavirenz)
12+ yr, phenytoin, or
efavirenz
Loading Dose 7-8 mg/kg/dose
q 12hr
6 mg/kg/dose q 12hr
for 2 doses
6 mg/kg/dose q 12hr
for 2 doses
Maintenance
Dose
7-8 mg/kg/dose
q 12hr
4 mg/kg/dose q 12hr 5 mg/kg/dose q 12hr
Connecticut Childrens Medical Center. Voriconazole dosing and monitoring in pediatric patients requiring treatment doses. BeST statement. June 2013.
22. (VFEND) Voriconazole Prescribing Information
Available IV, PO tablets, and oral suspension
Safety & efficacy not established in age < 12
Max: 350 mg/dose
The pharmacokinetics of voriconazole are non-linear
(dose dependent) due to saturation of its metabolism
• Increasing the oral dose from 200 mg BID to 300 mg BID leads to a
2.5-fold increase in exposure (AUC)
• Increasing the intravenous dose from 3 mg/kg BID to 4 mg/kg BID
produces a 2.3-fold increase in exposure
VFEND (voriconazole)[package insert]. Pfizer Inc. New York (NY) 2015.
23. ADME
Absorption
Tmax: 1-2 hrs (immunocompromised children: 1.3 - 2.8 hr)
Oral bioavailability, pediatrics: 65% to 66%
High-fat meals reduce the mean Cmax and AUC by 34% and 24%
(tablet) and by 58% and 37% (oral suspension)
Advise to take at least 1hr before/after meal
Distribution
Vd, Children: 1.852 L/kg
Protein binding: 58% PO
VFEND (voriconazole)[package insert]. Pfizer Inc. New York (NY) 2015.
24. ADME
Metabolism
Hepatic via CYP2C19 (CYP2C9 and CYP3A4)
CYP2C19 exhibits genetic polymorphism
It is recommended that the standard loading dose regimens be used, but
maintenance dose be halved in patients with mild to moderate hepatic
cirrhosis
Excretion
less than 2% unchanged
Renal clearance, children:141.9 mL/hr/kg
No adjustment is necessary for oral dosing in patients with renal impairment
Intravenous voriconazole should be avoided in patients with moderate to
severe renal impairment (CrCl < 50 mL/min)
Dialyzable
VFEND (voriconazole)[package insert]. Pfizer Inc. New York (NY) 2015.
26. Voriconazole Side Effects
DRUGDEX® System (electronic version). Voriconazole. Truven Health Analytics, Greenwood Village, Colorado, USA. Available at: http://www.micromedexsolutions.com/ (cited:
11/11/2016).
Visual (21%) Photophobia, blurriness
CNS (3-16%) hallucination, HA, chills
GI (12%) N > V > D
Hepatotoxicity (3-12%)
Rash (7%)
Fever (6%)
QTc
< 2%
27. Voriconazole Trough Monitoring
BeST Statement
Measure just prior (within 30min) of
dose on Day 5 of therapy
Trough Goal: 1.0 - 5.5 mcg/mL
Measure weekly thereafter once
therapeutic
Connecticut Childrens Medical Center. Voriconazole dosing and monitoring in pediatric patients requiring treatment doses. BeST statement. June 2013.
28. Trough Adjustment
Initial Trough < 1 mcg/mL Increase daily dose 50%
Repeat Trough < 1 mcg/mL Increase BID TID
Any Trough > 5.5 mcg/mL Hold until < 5.5 mcg/mL
Then decrease dose 50%
Adverse Event Contact Attending
Voriconazole Trough Monitoring
BeST Statement Cont.
Connecticut Childrens Medical Center. Voriconazole dosing and monitoring in pediatric patients requiring treatment doses. BeST statement. June 2013.
29. Patient Dosing/Trough Record
Original Dose Trough Level (mcg/mL) Dose Change
9mg/kg IV BID 20.3 (not true trough) Hold dose
4.5mg/kg IV BID Re-test and get 2.0 Back to 9mg/kg IV BID
9mg/kg IV BID 0.7 (Low) 9mg/kg IV TID
9mg/kg IV TID 1.2 None
9mg/kg IV TID 5.7 (High) 8mg/kg IV TID
8mg/kg IV TID 6.8 (High) Hold dose
Restart at 7mg/kg IV BID 0.4 (Low) 7mg/kg IV TID
30. Patient Dosing/Trough Record Cont.
Original Dose Trough Level (mcg/mL) Dose Change
7mg/kg IV TID 1.7, 1.5, 3.6, 1.5, 0.9 None
7mg/kg IV TID 0.5 (Low) 10mg/kg IV TID
10mg/kg IV TID 0.2 (Low) 15mg/kg IV TID
15mg/kg IV TID 11 (High) 12.5mg/kg IV TID
12mg/kg IV TID 1.6, 1.6, 4.4, 3.4, 2.1, 1.7 12.5mg/kg PO TID
31. 4 Months Later…
The patient has survived 5 transfers to and from the PICU.
Imaging and clinical signs show steady improvement. Six
voriconazole troughs in a row are within the therapeutic range.
He is discharged on voriconazole 12.5mg/kg PO suspension TID
given through his G tube.
He has also restarted chemotherapy with 2 rounds of NECTAR
for his relapsed ALL.
NECTAR = Nelarabine, Etoposide and Cyclophosphamide in
T-ALL Relapse
32. Summary
Immunocompromised patients are at a much higher risk
for opportunistic fungal infection
Trichosporon spp. are often resistant to antifungal therapy
due to the production of biofilm
Voriconazole has the greatest inhibitory effect against
Trichosporon spp.
Voriconazole trough levels can be extremely
unpredictable due factors such as genetic variability,
nonlinear metabolism, and drug-drug interactions
The benefits of treatment typically outweight the risks in
patients with fungemia
34. References
1. Li J, Li Y, Huang B, Zheng D, Chen M, Zhou Z. Drug-induced modulation of T
lymphocytes as a potential mechanism of susceptibility to infections in patients
with multiple myeloma during bortezomib therapy. Cell Biochem Biophys. 2015;
71(1):457-64
2. Konstantinos Leventakos et al. Clin Infect Dis. 2010;50:405-415
3. van Schie RM, Brüggemann RJ, Hoogerbrugge PM, te Loo DM. Effect of azole
antifungal therapy on vincristine toxicity in childhood acute lymphoblastic leukaemia.
J Antimicrob Chemother. 2011;66(8):1853-6.
4. Maves RC. Medscape. Trichosporon infections. URL:
http://emedicine.medscape.com/article/230705-overview [accessed 2016 Nov 16]
5. Iturrieta-González IA, Padovan AC, Bizerra FC, Hahn RC, Colombo AL. Multiple
species of Trichosporon produce biofilms highly resistant to triazoles and
amphotericin B. PLoS One. 2014;9(10):e109553.
6. Mitchell KF, Zarnowski R, Andes DR (2016) Fungal Super Glue: The Biofilm Matrix
and Its Composition, Assembly, and Functions. PLoS Pathog 12(9): e1005828
7. Hazirolan G, Canton E, Sahin S, Arikan-Akdagli S. Head-to-head comparison of
inhibitory and fungicidal activities of fluconazole, itraconazole, voriconazole,
posaconazole, and isavuconazole against clinical isolates of Trichosporon asahii.
Antimicrob Agents Chemother. 2013;57(10):4841-7.
8. DRUGDEX® System (electronic version). Voriconazole. Truven Health Analytics,
Greenwood Village, Colorado, USA. Available at:
http://www.micromedexsolutions.com/ (cited: 11/11/2016).
9. Connecticut Childrens Medical Center. Voriconazole dosing and monitoring in
pediatric patients requiring treatment doses. BeST statement. June 2013.
10. VFEND (voriconazole)[package insert]. Pfizer Inc. New York (NY) 2015.
Notas do Editor
-Retrospectively analyzed the clinical data of 143 patients who had received bortezomib therapy for MM
-Bortezomib therapy was associated with higher incidence rates of viral and fungal infections (15.8%, p < 0.05 vs. conventional chemotherapy). In addition, patients with the IgG immunophenotype showed higher bacterial and viral infection rates (respectively, p = 0.008 and 0.009).
JD received 4 doses, the last one a month before he presented to the ED
https://www.ncbi.nlm.nih.gov/pubmed/25343940
-Prolonged neutropenia is a key risk factor for acquiring invasive mold infection, especially invasive aspergillosis (IA)
-In the 1980s, candidiasis emerged as the prominent mycosis. However, since the widespread use of azole prophylaxis in the early 1990s in leukemia units, candidiasis has become less common
20 pediatric patients with ALL were included. Functioned as own control.
Patients receiving vincristine in combination with azole treatment experienced significantly more constipation and peripheral neurotoxicity (P=0.001 and P<0.001, respectively). Combination could be life threatening
MRI – lumbar spine, possible brain lesion
assess the liver along with spleen in weekly US
Biofilms are complex surface-associated cell populations embedded in an ECM that possess distinct phenotypes compared to their planktonic cell counterparts
http://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1005828/
D/C flagyl since he is on meropenem
Also still has vancomycin
In patients with creatinine clearance <50 mL/min, accumulation of the intravenous vehicle (solubilizing agent) sulfobutylether-ß-cyclodextrin sodium (SBECD) occurs. Accumulation of high doses of SBECD in the blood has caused liver necrosis and renal tubular obstruction in animal studies.
Moriyama B, Henning SA, Leung J, Falade-Nwulia O, Jarosinski P, Penzak SR, Walsh TJ. Adverse interactions between antifungal azoles and vincristine: review and analysis of cases. Mycoses. 2012 Jul;55(4):290-7.
Voriconazole inhibition often leading to cardiac toxicity
7-8 mg/kg IV BID is typical. 9 slightly high
Repeat Level < 1 BID TID
Level > 5.5 Hold dose
Already at TID, increase dose 50% to 10
Already at TID, increase dose 50%