
Recomendados
Mais conteúdo relacionado
Semelhante a Heart Failure.ppt
Semelhante a Heart Failure.ppt (20)
Mais de Sheik4
Mais de Sheik4 (20)
Último
Último (20)
Heart Failure.ppt
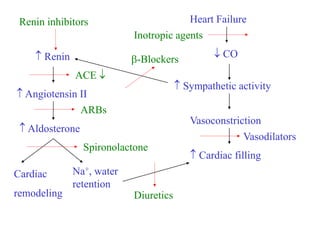
- 1. Heart Failure CO Sympathetic activity Vasoconstriction Cardiac filling Renin Angiotensin II Aldosterone Na+, water retention Cardiac remodeling Inotropic agents -Blockers Renin inhibitors ACE ARBs Spironolactone Diuretics Vasodilators
- 2. Diuretics: •Reduce extracellular fluid volume •Natriuresis and decrease in intravascular volume •Reduce preload on heart •Dietary sodium intake restriction •Loop diuretics – furosemide, bumetanide, torsemide- inhibit Na+-K+-2Cl- symporter in the ascending loop of Henle to increase Na+ and water delivery to distal tubule •Also increase K+ excretion •Thiazide Diuretics- chlorthiazide, hydrochlorthiazide- limited value in CHF •Act on Na+Cl- co-transporter in distal convoluted tubule
- 3. •K+ loss occurs more than that with loop diuretics •Often combined with loop diuretics when patient is refractory to loop diuretics •K+ Sparing Diuretics- Spironolactone, triamterene, amiloride are weak diuretics-for achieving volume reduction with minimal K+ loss •Usually, treatment is started with loop diuretics either orally (compensated) or i.v. (decompensated) patients •Diuretic resistance- due to compensatory increase in renal tubular reabsorption of Na+ •Diuretics do not improve upon the mortality rate in patients
- 4. Vasodilators: •Nitrosovasodilators •ACE inhibitors/ARBs •Nitrosovasodilators: NO donors which activate soluble guanylate cyclase in vascular smooth muscle cells to relax them Rapid acting nitroglycerine tablets or spray (sublingual) Short acting oral agents like isosorbide dinitrate Long acting oral agents like isosorbide mononitrate Topical like transdermal patches, ointments of nitroglycerine I.V. like nitroglycerine
- 5. How nitrates are helpful in CHF? •Reduce preload due to peripheral pooling •Reduction of pulmonary and systemic arterial resistance •Epicardial coronary artery dilatation- reperfusion •Given alone their efficacy is limited due to: limited effect on systemic resistance Nitrate tolerance •Often combined with other vasodilators for better results
- 6. Na Nitroprusside: During biotransformation of nitroprusside, cyanide is produced which is quickly converted to thiocynate in the liver and excreted by the kidney •ADR: Thiocynate or cyanide toxicity may occur following prolonged drug administration •Symptoms: unexplained abdominal pain, change in mental status, convulsions, lactic acidosis •Treatment: Sodium nitrite: It oxidizes some iron of haemoglobin to ferric state and converts it to methaemoglobin. Cyanide preferntially binds to methaemoglobin to form cyanmethaemoglobin. Administration of sodium thiosulphate converts cyanmethaemoglobin to thiocyanate, sulfite and haemoglobin. Thiocyanate is excreted by the kidney
- 7. Hydrocobalamin (B12): It binds to cyanide to form harmless vitamin B12acyanacobalamin that is excreted by the kidney 4-Dimethylaminophenol: It forms methaemoglobin in the body that binds to cyanide Dicobalt adetate: It chelates cyanide •ADR: Methaemoglobinemia: due to oxidation of haemoglobin by NO- •Treatment: Methylene blue: It acts as artificial electron acceptor for NADPH-methaemoglobin reductase and allows the enzyme to function again
- 8. Hydralazine: •Direct acting vasodilator •Mechanism of action not known •Reduces both right and left ventricular afterload by reducing pulmonary and systemic vascular resistance •Results in increased cardiac output and decreased ventricular wall stress during systole •Also has moderate direct positive inotropic activity independent of its afterload reducing effects •Reduces renal vascular resistance and increases renal blood flow •Increases renal blood flow more than any other vasodilator except ACE inhibitors •Preferred drug in CHF (ACE intolerant) with renal impairment
- 9. •Hydralazine is more often used in combination with isosorbide dinitrate •The combination is as effective in CHF as 1 blocker prazosin •ACE inhibitors are superior to hydralazine in reducing mortality in CHF •ADRs: withdrawal effect, lupus like syndrome •Oral/i.v. – oral is equally effective as i.v. • Has to be taken 3-4 times a day- patient compliance •I.V. hydralazine is used for its immediate effect only- urgency •10-25 mg/day orally increased gradually; maximum dose 100 mg 3-4 times a day
- 10. ACE Inhibitors: •Effects of angiotensin II: Potent vasoconstrictor Na+ and water reabsorption from renal tubule (effect on filtration pressure and secretion of aldosterone) Modulation of neural and medullary catecholamine release Arrhythmogenic Promotes vascular and myocardial hyperplasia Induces myocyte death Reduction of RAS leads to beneficial effects in CHF
- 11. •ACE inhibitors: Suppress angiotensin II and aldosterone production Decrease sympathetic activity Potentiate effects of diuretics in CHF •Angiotensin II escape: After chronic therapy with ACE inhibitors, angiotensin II levels return to normal but effect of ACE inhibitors persists- the normalization of angiotensin II is called “escape” •Suggests that other mechanisms besides ACE inhibition also play a role in their effects •Bradykinin and other kinins- stimulate production of NO, cyclic GMP, vasoactive eicosanoids that dilate the blood vessels, oppose angiotensin II effect on smooth muscle cells of blood vessels and fibroblasts proliferation & extracellular matrix deposition in heart
- 12. •ACE inhibitors are preferential arterial vasodilators • Left ventricular afterload by PVR & cardiac output •HR remains unchanged probably due to sympathetic activity •Acts via AT1 receptors so ARBs are more effective than ACE inhibitors •Both beneficial and deleterious effects are due to activation of AT1 receptors •AT2 receptor activation appears to counterbalance deleterious effects of AT1 activation •Increase in circulating levels of angiotensin II in response to ARBs results in relative increase in AT2 receptor activation •Combination therapy with ACE inhibitors and ARBs is under trial
- 13. •ACE inhibition alone is not sufficient for optimal attenuation of angiotensin II induced CV dysfunction in patients of CHF •Reasons: ACE independent pathways that convert Ang I to Ang II Activation of ACE homologs like ACE2 occurs that are insensitive to conventional ACE therapy Suppression of negative feed back effect on renin secretion •Thus, some amount of angiotensin like activity persists that is deleterious to CV functions •Inhibition of renin secretion prevents conversion of angiotensinogen to angiotensin I due to which angiotensin II formation does not occur, directly or through alternate routes •Under trial
- 14. Nesiritide: •Introduced recently for treatment of CHF •Recombinant form of human natriuretic peptide •Naturally secreted by the ventricles, increases cGMP in vascular smooth muscles and reduces arteriolar and venous tone •Causes natriuresis •Short t½ of 18 min •Administered as bolus dose 2 µg/kg i.v. followed by continuous i.v.infusion of 0.01 to 0.03 µg/kg/min •Used in acute decompensated heart failure associated with dyspnoea at rest •ADR: hypotension
- 15. Vasopressin receptor antagonists: •Vasopressin or ADH is released in response to: Increased plasma osmolality Decreased arterial pressure Reduced cardiac filling •Two types of vasopressin receptors- V1 and V2 •V1 mediate vasoconstrictor while V2 mediate antidiuretic action •Conivaptan is mixed V1 and V2 antagonists and Tolvaptan is V2 antagonist •Conivaptan is given i.v. while tolvaptan is given orally •Though beneficial, they donot reduce mortality so long term usefullness is doubtful
- 16. Role of sympathetic activation in CHF CHF Sympathetic activation Inotropy ( contractility) Lusitropy ( Ventricular relaxation & filling) Chronotropy ( Heart rate)
- 17. -Adrenoceptor antagonists: • agonists dobutamine as also dopamine provide relief in CHF but their long term use increases mortality •Long term administration of -antagonists reduce mortality rate in CHF •Initially the systolic function decreases but over 2-4 months it recovers and improvement beyond baseline occurs •Mechanism of beneficial effects in CHF not clear By preventing myocardial ischemia without significantly influencing serum electrolytes, they may decrease frequency of unstable tachyarrhythmias Betterment of left ventricular morphology by decreasing left ventricular size and increasing ejection fraction
- 18. By inhibiting sustained sympathetic discharge, they reduce catecholamine induced cardiomyote toxicity and prevent or delay myocardial contractile dysfunction Decrease cardiomyocyte apoptosis May induce positive myocardial remodeling by decreasing oxidative stress on myocardium •Drugs used: metoprolol, carvedilol, bisoprolol- other -blockers are not effective •Combined and blocker is preferred •Carvedilol has additional advantages that it reduces free radical induced lipid peroxidation and prevents cardiac and vascular smooth muscle mitogenesis independent of its or receptor blocking activity
- 19. • Adrenoceptor blockers have proven utility in improving symptoms, hospitalization and mortality in patients of CHF •They are recommended for use in patients along with ACE inhibitors or ARBs •Recommended only when the ejection fraction of heart is <35% to counter the deleterious effects of circulating catecholamines •They are usually given in small doses initially, less than 1/10th of the final dose and gradually titration of dose is done •Not recommended for use in patients with severe, new onset or acutely decompensated CHF