Salivary glands – anatomy and physiology
•Transferir como PPTX, PDF•
184 gostaram•33,978 visualizações

Detailed anatomy and physiology of major and minor salivary glands including applied aspects and various pathologies

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Salivary glands – anatomy and physiology
Semelhante a Salivary glands – anatomy and physiology (20)
Último
Último (20)
Salivary glands – anatomy and physiology
- 1. Salivary Glands – Anatomy and Physiology Saurabh Roy 11.11.151
- 2. Overlay : Introducing Glands Salivary Glands Classifying Salivary glands Embryology of Salivary glands Anatomy and Clinical implications Parotid Submandibular Sublingual Minor Physiology and Clinical implications Conclusion References 2
- 3. Introduction – What are Glands?: A cell, group of cells, or organ that selectively removes materials from the blood, concentrates or alters them, and secretes them for further use in the body or for elimination from the body Typically, a gland consists of either cuboidal or columnar epithelium resting on a basement membrane and is surrounded by a plexus, or meshwork, of blood vessels. http://www.britannica.com/science/gland 3
- 4. Types of Glands: Endocrine, or ductless, glands (e.g., pituitary, thyroid, adrenal) secrete substances known as hormones directly into the bloodstream rather than through ducts. Exocrine glands (e.g., salivary, sweat, digestive) discharge their products through ducts. 4
- 5. Types of Exocrine glands : Exocrine glands. Max sweat glands, Salivary glands, Lacrimal glands Sweat glands around lips and arm pits Sebaceous glands, Meibomian glands 5
- 6. Types based on Ductal Pattern : Exocrine glands. 6
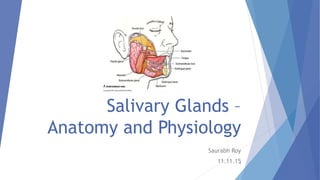
- 7. Salivary Glands: Salivary glands are a group of exocrine, merocrine, simple/compound tubulo-acinar type of glands secreting saliva The saliva forms a film of fluid coating the teeth and mucosa thereby creating and regulating a healthy environment in the oral cavity Oral fluid, which is referred to as mixed or whole saliva, includes the secretion of major glands, the minor glands, desquamated oral epithelial cells, microorganisms and their products, food debris and serum components and inflammatory cells that gain access through the gingival crevice 7
- 8. Classifying Salivary Glands: Based on size Histochemical nature of fluid Ductal system 8
- 9. Classifying Salivary Glands: According to size : Major salivary glands : Parotid, Submandibular , Sublingual Minor salivary glands : Carmalt’s glands, Glands of Von ebner 9
- 10. Classifying Salivary Glands: According to nature of secretion: Pure Serous – Parotid, Glands of Von Ebner Pure Mucous – Anterior lingual Glands of Blandin and Nuhn Mixed – Submandibular and Sublingual 10
- 11. Classifying Salivary Glands: According to ductal systems : Simple – Minor Salivary glands Compound – Major Salivary glands 11
- 12. Embryology: 12
- 13. Embryology: The individual salivary glands arise as a proliferation of oral epithelial cells, forming a focal thickening that grows into the underlying ectomesenchyme Continued growth results in the formation of a small bud connected to the surface by a trailing cord of epithelial cells, with mesenchymal cells condensing around it Formation of clefts occurs; forming 2 or more buds Continuation of this process, called Branching Morphogenesis produces successive generations of buds and a hierarchic ramification of the gland Branching morphogenesis, defined as growth and branching of epithelial tubules during embryogenesis, is a fundamental feature of renal, lung, mammary gland, submandibular gland, and pancreatic morphogenesis in mammals. Hu MC, Rosenblum ND ;Genetic regulation of branching morphogenesis: lessons learned from loss-of-function phenotypes. Pediatric Res. 2003 Oct;54(4):433-8. Epub 2003 Aug 6. 13
- 14. Embryology: 14
- 15. Embryology: The cells of secretory end pieces and ducts attain maturity during the last 2 months of gestation 15
- 16. Microstructure of Glands: Secretory units(Acini): • Serous cells • Mucous cells Myoepithelial cells Ductal units • Intercalated ducts • Striated ducts • Excretory ducts Connective Tissue: Surrounding capsule Tissue septae Tissue elements 16
- 18. Serous cells: Pyramidal with a broad base on the basement membrane, apex facing the lumen Secretory granules – Zymogen granules present in the apical cytoplasm Abundance of RER Mature zymogen granules expelled from the cell surface by exocytosis 18
- 19. Mucous cells: Typically have a tubular configuration Mucous end pieces in some cases have serous cells associated with them in the form of a demilune The most prominent feature of mucous cells is the accumulation in the apical cytoplasm of their secretory product – mucus Have a large Golgi complex, located basal to the mass of secretory granules 19
- 21. Myoepithelial cells: Contractile elements associated with the secretory end pieces and intercalated ducts Stellate shaped, numerous branching processes which envelop the secretory end piece Fusiform shaped with fewer processes These processes are filled with actin and soluble myosin Contraction of these processes provides support to the end pieces during active secretion of saliva Recent evidence also suggests that these cells provide signals to acinar units to maintain cell polarity and structural organization of acini 21
- 22. Ductal Elements: Acini Intercalated ducts Striated ducts Excretory ducts Stenson’s/ Wharton’s ducts22
- 23. Ductal elements: • Single layer of cuboidal cells • Secretory units may also secrete lysozyme and lactoferrin Intercalated ducts: • Constitute largest portion of ductal system; Columnar cells • Modification of primary saliva by reabsorbtion and secretion of electrolytes Striated ducts: • Pseudostratified columnar epithelium • Other types of cells viz. Tuft cells, lymphocytes and macrophages may be present within Terminal Excretory ducts: 23
- 24. Anatomy and Clinical Implications : 24
- 25. Parotid Gland : Largest serous salivary gland Weighs around 15 gms Resembles a 3 sided pyramid with apex directed downwards 4 surfaces: Superior Superficial Anteromedial Posteromedial Separated by 3 borders: Anterior Posterior Medial 25
- 26. Parotid Capsule : Formed by Investing layer of deep cervical fascia Fascia splits to enclose the gland Superficial lamina – Thick and adherent is attached to the zygomatic arch Deep lamina – Thin; attached to the styloid process, the angle & posterior border of ramus and tympanic plate A portion of the deep lamina thickens to form the stylomandibular ligament which separates the parotid from the submandibular gland 26
- 27. Parotid Gland - Relations : 27
- 28. Parotid Gland - Relations: Superior Surface Concave, Related to Cartilaginous part of ext acoustic meatus Post. Aspect of temperomandibular joint Auriculotemporal Nerve Sup. Temporal vessels Apex Overlaps posterior belly of digastric and adjoining part of carotid triangle Superficial Surface; Covered by Skin Superficial fascia containing facial branches of great auricular N Superficial parotid lymph nodes and post fibres of platysma 28
- 29. Parotid Gland - Relations : Anteromedial Surface Grooved by posterior border of ramus of mandible Related to Masseter Lateral Surface of temperomandibular joint Medial pterygoid muscles Emerging branches of Facial N 29
- 30. Parotid Gland - Relations : Posteromedial Surface is related to Mastoid process with sternomastoid and posterior belly of digastric. Styloid process with structures attached to it. External Carotid Artery which enters the gland through the surface Internal Carotid Artery which lies deep to styloid process 30
- 31. Parotid Gland – Structures within: Arteries : 31
- 32. Parotid Gland – Structures within: Veins: 32
- 33. Parotid Gland – Structures within: Nerves: 33
- 34. Patey’s Faciovenous plane: Large superficial and small deep part of the gland interconnected by an isthmus Facial nerve divides along this plane 34
- 35. Patey’s Faciovenous plane:- Clinical Significance The facial nerve must be traced from behind forwards as it emerges from the stylomastoid foramen and enters the parotid gland The nerve is surrounded by a leash of veins called the neuro-venous plexus of Patey which must be followed with fine dissection, preferably under a microscope, to surgically divide the isthmus. 35
- 36. Parotid duct/Ductus parotideus/Stenson’s Duct: Thick walled and about 5 cm long Emerges from the middle of the anterior border of the gland Superior relations: Accessory parotid Transverse facial vessels Upper Buccal branch of facial nerve Inferior relations: Lower buccal branch of facial nerve 36
- 37. Parotid duct/ ductus parotideus/ Stenson’s Duct: At the anterior border of the masseter, the parotid duct turns medially and pierces: Buccal fat pad Buccopharyngeal fascia Buccinator The duct runs forwards for a short distance between the buccinator and the oral mucosa. Finally, the duct opens into the gingivobuccal vestibule opposite the crown of the maxillary 2nd molar tooth 37
- 38. Parotid duct/ ductus parotideus/ Stenson’s Duct : Surface anatomy: Corresponds to middle third of a line drawn from lower border of tragus to a point midway b/w nasal ala and upperlabial margin 38
- 39. Parotid Gland – Blood Supply : Arterial supply: External carotid artery and its branches within the gland Venous drainage: External & internal jugular vein 39
- 40. Parotid Gland – Nerve Supply: • Secretomotor • Reach through auriculotemporal nerve Parasympathetic 40
- 41. Parotid Gland – Nerve Supply: • Vasomotor • Derived from the plexus around the middle meningeal artery Sympathetic nerves • Derived from the auriculotemporal nerve but the parotid fascia is innervated by the sensory fibres of Great Auricular nerve(C2,C3) Sensory nerves 41
- 42. Parotid Gland – Lymph Nodes: Lie partly in the superficial and partly in the deep fascia over the parotid gland Drainage: Temple Side of the scalp External acoustic meatus Middle ear Parotid gland Upper part of the cheek Parts of eyelids and orbit 42
- 43. Anatomy – Clinical implications : Parotid swellings are extremely painful due to the unyielding nature of parotid fascia – Acute Parotitis 43
- 44. Anatomy – Clinical implications : A Parotid abscess may be caused by spread of infection from the opening of parotid duct in the oral cavity Else it may present as a slight swelling with redness on the surface of the swelling accompanied by acute, excruciating pain It results from bacterial parotitis with the spread of pathogen in a retrograde manner Does not show fluctuation due to unyielding nature of parotid capsule Best drained by Horizontal incision known as Hilton’s Method below the angle of the mandible 44
- 45. Anatomy – Clinical implications : Parotidectomy is the surgical removal of the parotid gland Injury to the auriculotemporal nerve can occur at a site where it turns around the neck of the mandible Because of the injury, postganglionic parasympathetic fibres from the Otic ganglion unite with sympathetic fibres of superior cervical ganglion which supplies vessels and sweat glands over skin overlying parotid region 45
- 46. Anatomy – Clinical implications : This causes stimulation of the sweat glands and hyperemia in its area of distribution, producing redness and sweating in the area of the skin supplied by the nerve This clinical entity is called Frey’s Syndrome/Auriculotemporal Syndrome 46
- 47. Anatomy – Clinical implications : Diagnosis : Minor’s Starch iodine test Prevention: Physical barrier between the skin and parotid bed by using muscle flaps from temporalis or SCM Treatment: Reassurance, aluminium chloride – antiperspirant(astringent) Denervation by tympanic neurectomy Injection of botulinum toxin into the affected skin 47
- 48. Anatomy – Clinical implications : During parotidectomy, the facial nerve is preserved by removing the gland in 2 parts, superficial and deep separately. Plane of cleavage is defined by tracing the nerve from behind forwards 48
- 49. Anatomy – Clinical implications : Swellings of parotid may either be due to inflammation or due to tumours (benign or malignant) Since the gland is positioned below, behind and in front of the lobule of the ear its swellings obliterate the normal hollow just below the lobule of the ear, which is invariably lifted in the parotid swellings A painless slow growing tumour is usually benign in nature which does not damage the facial nerve On the contrary, the malignant growth is characterized by rapidly growing painful swelling which involves the facial nerve producing facial palsy. Fixity with hardness and enlargement of cervical lymph nodes are other features 49
- 50. Submandibular Gland : Location : Anterior part of Digastric triangle Size of a walnut, roughly J-shaped Superficial Part: Larger part, filling up the digastric triangle Extends up till the mylohyoid line It has inferior, medial and lateral surfaces Partially enclosed between 2 layers of deep cervical fascia 50
- 51. Submandibular Gland : Superficial Part: - Relations : Inferiorly: Skin Platysma Cervical branch of facial nerve Deep fascia Facial vein Submandibular Lymph Nodes Medially: Mylohyoid Hyoglossus Styloglossus Laterally: Submandibular fossa on the mandible Insertion of medial pterygoid Facial Artery 51
- 52. Submandibular Gland : Deep part: Small sized, lies deep to Mylohyoid, superficial to hyoglossus and styloglossus Relations: Laterally: Mylohyoid Medially: Hyoglossus Superiorly: Lingual nerve with submandibular ganglion Inferiorly: Hypoglossal Nerve 52
- 53. Wharton’s Duct: Thin walled, about 5 cm long Emerges at the anterior end of the deep part of the gland Crossed by the lingual nerve at the region of anterior border of the hyoglossus Opens on the floor of the mouth, on the summit of the sublingual papilla, at the side of tongue frenulum 53
- 54. Blood and Lymph Supply: Supplied by the facial artery Veins drain into the common facial or lingual vein Lymph passes into submandibular lymph nodes 54
- 55. Nerve Supply: Submandibular ganglion: Secretomotor fibres Vasomotor sympathetic fibres from facial artery plexus Sensory fibres from lingual nerve 55
- 56. Submandibular Gland – Clinical Implications: The chorda tympani supplying secretomotor fibres to submandibular and sublingual glands lies medial to the spine of sphenoid The auriculotemporal nerve supplying secretomotor fibres to parotid is related to the lateral aspect of the sphenoid Injury to spine may involve both these nerves with loss of secretion from all 3 salivary glands 56
- 57. Submandibular Gland – Clinical Implications: Chronic Submandibular Sialadenitis : Obstruction Trauma to floor of mouth 57
- 58. Submandibular Gland – Clinical Implications: Sialadenitis due to calculi : Disease starts with acute bacterial Sialadenitis which occurs secondary to obstruction Submandibular gland has a poor capacity for recovery following obstruction 58
- 59. Submandibular Gland – Clinical Implications: Sialadenitis due to calculi : Calculi are more common in the submandibular gland because of the following reasons Higher mucin content Higher Calcium and phosphate content Non dependent drainage Kinking of Wharton’s duct 59
- 60. Submandibular Gland – Clinical Implications: Sialadentis due to calculi : Clinical features: Salivary colic Lingual colic H/O Enlargement of glands during meals Palpable calculi within the gland, the duct or the orifice Progression into severe septic Sialadentis mimicking Ludwig’s 60
- 61. Submandibular Gland – Clinical Implications: Sialadentis due to calculi : Treatment: 1. Stone in duct : removed by incising the mucosa over floor of mouth and/or milking the stone, followed by a gush of blocked contents 2. Chronic Sialadentis : Excision of submandibular gland Complications : Damage to lingual nerve, marginal mandibular nerve, hypoglossal nerve Seroma and infection 61
- 62. Sublingual Gland : Smallest of the 3 salivary glands Almond-shaped and weighs 3-4 g About 15 ducts emerge from this gland Most open directly onto the floor of the mouth while some join the submandibular duct 62
- 63. Sublingual Gland : Blood supply: Lingual and submental arteries Nerve supply: Similar to submandibular gland Relations: Anteriorly: Meets with gland on opposite side Posteriorly: Contacts with deep part of Submandibular Gland Superiorly: Mucous membrane of the mouth Inferiorly: Mylohyoid muscle Laterally : Sublingual fossa Medially: Genioglossus muscles 63
- 64. Clinical Implications: Ranula : Translucent cystic swelling with a bluish tinge situated on one side of frenulum linguae Almost always unilateral Painless, slow growing ,soft, movable mass located at the floor of the mouth When a ranula herniates through the mylohyoid & extends into the neck so that it can be palpable in the submandibular triangle, its called a Plunging Ranula 64
- 65. Minor Salivary Glands: They are located beneath the oral epithelium in almost all parts of the oral cavity except in the gingiva, ant. Hard palate and ant. 2/3rd of tongue dorsum 600 – 1000 in number present in small clusters of secretory units Classified according to their anatomic location Continuous slow secretory activity Often supersede the activity of major salivary glands at night 65
- 66. Minor Salivary Glands: Glands of Blandin and Nuhn Mostly Located near apex of tongue, some also found posteriorly Chiefly mucous Anterior glands open on ventral surface near lingual frenum Posterior glands open on tongue dorsum 66
- 67. Minor Salivary Glands: Glands of Von ebner Located on posterior aspect of tongue Exclusively serous Functions: Washout of trough papillae Readying taste receptors for a new stimulus Antibacterial activity (lysozyme and peroxidase) Lipolytic activity (lingual lipase) with significant activity in newborn when pancreatic lipase activity is low 67
- 68. Clinical Implications : Mucocoele : Clinical term that describes swelling caused by accumulation of saliva at the site of a traumatized or obstructed salivary duct Extravasation mucocoeles most commonly occur on the lower lip,buccal mucosa, tongue and floor of the mouth Retention mucocoeles commonly occur on the palate 68
- 69. Clinical Implications: Minor Salivary gland tumour : They can present either as a mucous retention cyst or as malignant tumour Since they are submucosal, they start as a submucosal nodule whuch helps them to differentiate from carcinoma lip/buccal mucosa etc Presence of an ulcer may be a feature of malignancy Treatment of benign cyst/tumour is by simple excision while malignant tumours require wide excision 69
- 70. Physiology of Salivary Secretion 70
- 71. Physiology of Salivary Secretion : Production – 1l/day (0.1 – 4 ml/min) varying from rest to stimulation Constituents: Water 94-99.5% Solids – 0.5-6% Inorganic Organic Organic micromolecules Gases 71
- 72. Functions of Saliva: Lubrication and protection Buffering and clearance Maintenance of tooth integrity Antibacterial activity Taste and digestion Excretion of certain drugs and inorganic ions 72
- 73. Mechanism of Salivary Secretion : Mechanism of Salivary Secretion: Active transport process under neuronal control Osmotic process 73
- 74. Mechanism of Salivary Secretion : 1. Acinar cells: K, Na and HCO3 ions along with Cl to preserve neutrality Primary secretion – Isotonic Ductal cells(rich blood supply) – Reabsorption of Na ions Secretion of HCO3 and K ions Final salivary secretion - Hypotonic 74
- 75. Mechanism of Salivary Secretion : 2. Since saliva is a hypo-osmotic secretion of salivary glands Hence, metabolic activity i.e. Oxygen consumption is increased by 5 folds during secretory activity as compared to that at rest 3. At rest, Saliva contains more K ions, less of Na, Cl and Bicarbonate ions compared to plasma However, as salivary flow increases, there is less time for ion exchange in the ducts, the result being less hypotonic and more isotonic resembling primary secretion 75
- 76. Mechanism of Salivary Secretion : 4. Aldosterone increases the K concentration and decreases the Na concentration of saliva Thus, a high salivary Na/K ratio is seen when aldosterone is deficient 76
- 77. Control of Salivary Secretion : 1. Stimulation of parasympathetic nerves: Liberates Kallikrein from the gland cells which acts on plasma globulins to form bradykinin Effect mediated by release of Ach Also causes release of Vasoactive Intestinal Polypeptide Thus ,the effects being: Vasodilatation in salivary glands Increased secretion from the acini 77
- 78. Control of Salivary Secretion : 2. Stimulation of sympathetic nerves: Shorter and less strong Probable synergistic action Causes secretion of small amounts of saliva rich in organic constituents and mucus from submandibular and sublingual glands 3. Salivary secretion increases either by : Taste of food within 20-30 seconds (Innate reflex) By sight ,smell or thought of food (Conditioned reflex) 78
- 79. Factors altering Salivary Flow: Unstimulated – Submandibular Stimulated – Parotid 2/3rd Acidic food – Max stimulation Sweet food – Least stimulation 79
- 80. Factors altering Salivary Flow: Psychic factors Circadian rhythm Diurnal variation Age Drugs Tricyclic antidepressants Phenothiazines Depression and anxiety states Dehydration, hemorrhage 80
- 81. Factors altering Salivary Flow: Salivary Gland diseases Radiation sialadenitis Autoimmune sialadenitis HIV infection Iron overload Sarcoidosis Amyloidosis Cystic fibrosis 81
- 82. Effect of Drugs on Salivary Flow: Sympathomimetic drugs like adrenaline and ephedrine stimulate salivary secretion Parasympathomimetic drugs like Ach, pilocarpine, muscarine and physostigmine increase the secretion of saliva Histamine stimulates salivary secretion Sympathetic depressants like ergotamine and dipheniramine abolish salivary secretion Parasympathetic depressants like atropine and scopolamine inhibit the secretion of saliva Anaesthetics like chloroform and ether stimulate the reflex secretion of saliva However, deep anaesthesia decreases salivary secretion due to central inhibition 82
- 83. Factors altering Salivary composition: Flow rate Source of secretion Type of stimulus Diurnal variation Diet Drugs – flow dependant components Hormones – mineralocorticoids, ovulation 83
- 84. Factors altering Salivary composition: Disease states Sialadenitis Radiation damage Sjorgen’s syndrome Cystic fibrosis HTN DM Alcoholic cirrhosis Aldosteronism Chronic pancreatitis 84
- 85. Applied Physiology: 1. Hyposalivation : Reduction in salivary secretion 2 types, temporary and permanent Temporary – Emotional conditions like fear, Fever, or Dehydration Permanent Sialolithiasis Congenital absence or hypoplasia of salivary glands Bell’s palsy 85
- 86. Applied Physiology: 2. Xerostomia : Dry mouth/Pasties/Cottonmouth Due to hyposalivation or aptyalism Causes : 1. Dehydration due to Renal failure 2. Sjogren’s syndrome 3. Post Radiotherapy 4. Trauma to gland or ducts 5. Side effect of some drugs 6. Shock 7. After smoking marijuana 86
- 87. Applied Physiology: 3. Hypersalivation: Excess secretion of saliva Physiological condition – Pregnancy Pathological hypersalivation is called Ptyalism, Sialorrhoea, Sialism or Sialosis Occurs in following conditions : Tooth decay or neoplasm of mouth or tongue Disease of oesophagus, stomach or intestine Neurological disorders like cerebral palsy and mental retardation Cerebral Stroke Parkinsonism Nausea and vomiting 87
- 88. Applied Physiology: 4. Drooling : Uncontrolled flow of saliva with inability to retain saliva in the mouth Occurs in following conditions : During teeth eruption in children Upper respiratory tract infection or nasal allergies in children Dysphagia Tonsillitis Peritonsillar abscess 88
- 89. Applied Physiology: 5. Paralytic secretion of Saliva : Iatrogenic/Traumatic severance of parasympathetic nerve supply Leads to increase in salivary secretion for 3 weeks, later it diminishes finally stopping at about 6th week The increased secretion of saliva after cutting the PS nerve fibres is called Paralytic secretion It is due to the release of large amounts of adrenaline from adrenal medulla after denervation Cutting of the sympathetic Nerve supply does not influence paralytic secretion 89
- 90. Applied Physiology: 6. Augmented Secretion of Saliva: If the nerves supplying salivary glands are stimulated twice, the amount of saliva secreted by the 2nd stimulus is more than due to the 1st stimulus It is because, the 1st stimulus increases excitability of acinar cells, so that when the 2nd stimulus is applied, the salivary secretion is augmented 90
- 91. Conclusion: Knowledge of anatomy and physiology of salivary glands is essential to distinctly identify various associated conditions and salivary gland pathologies Precise anatomical knowledge is also essential to plan out our treatment strategies and alter the patient’s lifestyle for the better 91
- 92. References: Inderbir Singh; Human Embryology; 10th edition; 96,178 Moore, Persaud, Torchia ; The Developing Human; 9th edition; 179 Inderbir Singh; Textbook of Anatomy; 5th edition Volume 3; 781 B D Chaurasia; Human Anatomy; 6th edition Volume 3; 106-112 , 133-8 K Sembulingam; Essentials of Medical Physiology; 4th edition; 197-203 A K Jain ; Textbook of Physiology; 4th edition Volume 1; 201-4 Antonio Nanci; Tencate’s Oral Histology; 8th edition; 253-71 G S Kumar; Orban’s Oral Histology and Embryology; 13th edition, 291-306 Somen Das; A manual on clinical surgery; 8th edition; 359-63 K Rajgopal Shenoy; Manipal Manual of Surgery; 4th edition; 302-8 http://www.britannica.com/science/gland http://www.ncbi.nlm.nih.gov/pubmed/12904600 https://shortnotesinplasticsurgery.wordpress.com/2013/12/17/40-surgery-of-the- parotid-gland/ http://www.google.com/images 92
- 93. Thank you and Good day.. 93
Notas do Editor
- The type of secretory product may also classify exocrine glands into 3 categories viz serous(protein rich), mucous(carbs rich), or sebaceous(lipid rich)
- The type of secretory product may also classify exocrine glands into 3 categories viz serous(protein rich), mucous(carbs rich), or sebaceous(lipid rich)
- tissue capsule, which separates these glands from adjoining structures….septa divides into lobes and lobules, carries blood vessels and nerves.. tissue elements like fibroblasts, adipose cells, mast cells, plasma cells , dendritic cells etc
- tissue capsule, which separates these glands from adjoining structures….septa divides into lobes and lobules, carries blood vessels and nerves..tissue elements like fibroblasts, adipose cells, mast cells, plasma cells , dendritic cells etc
- The various branches radiate like a goose foot to supply the muscles of facial expression: hence the name, pes anserinus
- Because of the oblique course of the duct through the buccinators the inflation of the duct is prevented while blowing
- Because of the oblique course of the duct through the buccinators the inflation of the duct is prevented while blowing
- Hence it becomes necessary to examine the functioning of facial nerve in case of parotid tumors by testing the muscles of facial expression. The palpation of cervical lymph nodes is also essential
- Addison’s