
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a disorders of Salivary gland ppt
Semelhante a disorders of Salivary gland ppt (20)
Último
Último (20)
disorders of Salivary gland ppt
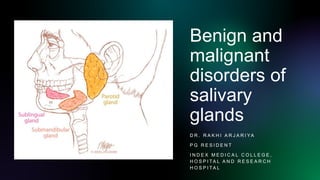
- 1. Benign and malignant disorders of salivary glands D R . R A K H I A R J A R I YA P G R E S I D E N T I N D E X M E D I C A L C O L L E G E , H O S P I TA L A N D R E S E A R C H H O S P I TA L
- 2. Salivary glands Definition: exocrine glands secreting salivary contents into the mouth. Classification according to size: Major(paired)- Parotid Submandibular Sublingual gland Minor(unpaired)- 800 in number • Buccal, palatine, lingual, floor of mouth, retromolar area, oropharynx.
- 3. Developmen t • Parotid gland: 6th to 8th week of IU life; Ectodermal origin • Submandibular gland: 6th week; endodermal origin • Sublingual and minor glands: 8th-12th weeks; endodermal origin
- 4. Parotid Gland Largest salivary gland; wt-25gm Located in the retromandibular fossa (parotid bed), between ramus of mandible and SCM. Enveloped by the investing layer of deep cervical fascia. Divided into superficial and deep lobe by the facial nerve. The accessory parotid gland is a separate part, lying on the masseter between parotid duct above and zygomatic arch below.
- 5. Relations: • Anterior: masseter, medial pterygoid • Posterior: posterior belly digastric muscle, sternocleidomastoid, mastoid process • Superior: EAM, TMJ • Inferior: SCM, Post belly of digastric • Lateral: investing layer of deep cervical fascia, platysma and skin • Medial: Investing layer of deep fascia, styloid process, IJV, ICA, pharyngeal wall.
- 6. STENSON’S DUCT • Arises from the anterior part of the gland; 1.5 cm inferior to zygomatic arch. • 5cm in length; 6mm diameter • Passes over the masseter • Pierces buccinator, opening opposite to the upper second molar. • Intraoral course provides valve like mechanism. •
- 7. Arterial supply Branches of external carotid artery Venous drainage Retromandibular vein into EJV Facial vein into IJV Lymphatic drainage Intra parotid LN Deep cervical nodes Level IIa IIb Nerve innervation •Parasympathetic-Secretomotor •Sympathetic-Superior cervical ganglion •Sensory- Greater auricular nerve Histology • Serous cells • Serous acini embryology • Ectodermal myoepithelial origin
- 8. Important structures • 3 chief structures either in part or in whole traverse the gland and branch inside it. From superficial to deep these are: • Facial nerve. • Retromandibular vein. • External carotid artery, dividing into the superficial temporal and maxillary branches. Click to add text
- 9. Relationship to Facial nerve • Facial nerve exits skull base from the stylomastoid foramen and enters posterior surface of the gland. • Within the substance divides into Upper zygomatico-temporal division Lower cervico-facial division • Facio-venous plane of patey • 5 peripheral branches: pes anserinus Temporal Zygomatic Buccal Mandibular cervical
- 10. Submandibular gland • The gland wraps around the posterior border of mylohyoid muscle. • It is composed of 2 parts: (a) a large superficial part and (b) a small deep part. • Superficial lobe is located in the submandibular triangle. • Deep part is located within the floor of the mouth. •
- 11. Superficial lobe: 3 Surfaces Superficial(inferior) surface relations: covered by fibrous layer-capsule Medial surface: • Anteriorly to Mylohyoid, nerve to mylohyoid, submental vessels • Posteriorly to Hyoglossus, submandibular ganglion, lingual nerve, hypoglossal nerve, styloid process and posterior belly of digastric. Lateral surface is related to: body of mandible
- 12. Anatomic relations: Deep part • Medially: Hyoglossus and styloglossus • Anteriorly: post. end of sublingual gland • Posteriorly wraps around the free edge of mylohyoid
- 13. Wharton's duct • 5 cm long • Arises from the deep part. • It runs between mylohyoid and hyoglossus and onto genioglossus opens into the oral cavity lateral to the frenulum of the tongue. • Lingual nerve double crosses the duct, starting medially and ends laterally. • Hypoglossal nerve runs parallel and inferior to it.
- 14. • Blood Supply : branches of facial & lingual arteries. • Venous drainage: facial & lingual veins • Lymph drainage : level Ib submandibular deep cervical lymph nodes
- 15. Submandibular Gland Supply • Parasympathetic: secretomotor fibers from superior salivary nucleus of facial nerve via chorda tympani nerve to join lingual nerve and pass into submandibular ganglion. • Postganglionic parasympathetic secretory fibers from ganglion via lingual nerve into gland. • Sympathetic fibers: from plexus of nerves around Facial + Lingual arteries. • Sensory: lingual nerve
- 16. Sublingual glands • It is located beneath the mucosa in the floor of the mouth. • Between mandible and genioglossus • Bound inferiorly by mylohyoid muscle. • It’s largely mucus in nature and weighs about 3-4 g.
- 17. • Blood supply-The sublingual and submental arteries. • Nerve supply- Through chorda tympani nerve; • Preganglionic fibres arise from superior salivatory nucleus; Postganglionic fibres arise from submandibular ganglion • Lymphatic drainage-Level Ia and Ib • The gland possesses about 20 ducts. • Ducts of Rivinus: open individually on the sublingual fold • Duct of Bartholin: which opens into the submandibular duct.
- 18. Classification of salivary gland disorders Salivary gland disorders Developmental Inflammatory Obstructive Other benign disorders Tumours Benign Malignant Rare
- 19. 1.Development Disorders 1. Atresia 2. Aplasia 3. Aberrancy: Staphne’s bone cyst, below the inferior dental neurovascular bundle. 4. Congenital fistula 5. Hyperplasia of gland 6. Diverticula of salivary gland
- 20. • Salivary diverticulum is a small pouch or out-pocketing of the duct system of a major salivary gland. Such diverticuli typically cause pooling of saliva and recurrent sialadenitis, especially parotitis or sialoliths.
- 21. 2.Inflammatory Conditions 1.Acute Bacterial Sialadenitis(suppurative parotitis) • MC affects parotid gland, caused by S.Aureus, S. Pyogenes • Sudden onset painful diffuse swelling of the involved gland; regional lymphadedopathy and fever. • Often seen in debilitating patients with poor oral hygiene. 2.Chronic bacterial Sialadenitis • Most commonly due to salivary calculi causing partial or complete obstruction of the salivary duct. • Most commonly seen in submandibular gland. • Chronic, intermittent, pain with unilateral swelling of the gland.
- 22. 3.Viral Sialadenitis(Mumps parotitis): • Paramyxo virus induced infection of parotid(mostly) or submandibular occasionally; • bilateral gland swelling, swollen cheek appearance • Low grade fever, mild headache, loss of appetite and abdominal pain • Complications include meningitis / encephalitis, deafness, pancreatitis, and orchitis. 4.Irradiation induced sialadenitis • Complication of radiotherapy • Directly related to dose of radiation and severity of damage • Irreplaceable damage followed by fibrous replacement of the acini causing Xerostomia.
- 23. 3.Obstructive disorders: Sialothiasis • Clinical features: Acute painful swelling, precipitated by eating Resolves 1-2 hrs after eating(complete obstruction); Recurrent attacks. • Male preponderance seen • Middle age Organic nidus Calcium salt deposition Calculi formation obstruction
- 24. Sialolithiasis Clinically, enlarged gland, tender on bimanual palpation. Majority of sialoliths occur in salivary gland. Investigation: X ray/ sialography (90 percent submandibular stones are radioopaque and 90% parotid stones are radiolucent)
- 25. Treatment • Sialoendoscopy(dormia basket) • >4 mm stones: intra/extra corporeal lithotripsy- >removal • Surgical methods: • Incision over the duct, f/b stone retrieval. • If fails, submandibular gland excision f/b duct ligation
- 26. Cysts of salivary glands 1. Mucus retention cysts: occur in minor salivary glands; secondary to obstruction 2. Mucus extravasation cyst: Trauma to the region causes pooling of mucus in the area followed by inflammatory reaction.
- 27. 3. Ranula: mucus extravasation cyst arising from sublingual glands • Female preponderance; 2nd decade of life • Possible association with HIV infection • Treatment: marsupialisation, laser ablation or cryosurgery 4. Plunging ranula: Ranula are classified as simple when they lie above mylohyoid and deep/plunging when they lie invade below this muscle. • Painless,persistent, recurrent neck swelling; rarely spreads to upper chest wall • Dumbell shaped, soft fluctuant swelling, in the submental/ submandibular region of the neck • Diagnosed on USG/ MRI. • Treatment: removal of sublingual gland and aspiration of saliva out of the sac.
- 28. • Plunging ranula(left) and Ranula(right). • Ranula: is a special type of mucocele which grows in the floor of the mouth, usually unilateral and is called due to its similar appearance to enlarged abdomen region of a frog. • Plunging ranula
- 29. Autoimmune disorders : Sjogrens syndrome • It is an autoimmune disorder causing progressive destruction of salivary and lacrimal glands. • F>M ; 10:1 ratio • Most commonly affects parotid gland. • Outline of parotid gland is demaracted in the picture.
- 31. Management: o Biopsy of the gland can aid with the diagnosis. o Treatment : symptomatic o Hydration; NSAIDs o Artificial tears, artificial salivary substitute,etc o ( picture above)B/L parotid swelling o Extensive cervical caries is a complication of dry mouth as patients tend to use sweet to stimulate salivary flow.
- 32. Snowstorm appearance • Sialogram showing snowstorm appearance of blobs of contrast leaked from the duct system. • Empyting and clearance of medium are also delayed because of reduced salivary flow.
- 33. 2.Mikulicz’s disease: • Presentation: asymptomatic, bilateral swelling of the parotid, and submandibular salivary glands+lacrimal glands. • resembles Sjogren’s syndrome. • Treatment- corticosteroid therapy in the acute phase, prednisone 40 mg per day for 2–4 weeks followed by a gradual tapering of the dose.
- 34. Other benign disorders: 1) Frey's syndrome 2) Sialorrhea 3) Xerostomia 4) Recurrent parotitis of childhood and obstructive parotitis 5) Sialodenosis 6) Granulomatous sialadenitis 7) Chronic sclerosing sialadenitis
- 35. 1. Frey's syndrome • aka Auriculo temporal syndrome • Sweating + erythema in the pre auricular and temporal areas after gustatory stimulation. • Caused due to faulty regeneration of sympathetic and parasympathetic nerve fibres injured during parotid tumor surgery/ramus resection. • Starch Iodine test: Paint the area with iodine followed by dry starch application, that turns blue on exposure to iodine in the presence of sweat.
- 36. Management • 1) Prevention: Using techniques like Sternomastoid muscle flap Temporalis fascial flap Insertion of artificial membranes between skin and parotid bed. • 2) Treatment: Antiperspirants Tympanic neurectomy Botulinium toxin injection
- 37. 2.Sialorrhea • Uncontrolled drooling in the presence of normal salivary production. • Certain drugs or oral infections cause transient increase in salivary flow rates. • It is seen in children with mental and physical handicap(Cerebral palsy). • Medical management: Antisialogogues(anti cholinergic agents) Surgical management include: Bilateral submandibular duct repositioning with sublingual gland excision Bilateral submandibular gland excision Transposition of parotid ducts with submandibular gland excision.
- 38. 3.Xerostomia(dry mouth) Common causes: • dehydration • Post menopause • Chronic anxiety or depression • Anticholinergics( antidepressants) • Sjogren's syndrome • Radiotherapy Treatment: • hydration • Withdraw the offending drugs
- 39. 4.Parotitis: 1. Recurrent parotitis of childhood: rapid swelling of one/both parotid glands Lasts 3-7days, f/b quiescent period of weeks-months varied number of attacks 1-5/year. Sialogram: punctate non obstructive sialectasis. Responsive to antibiotics and endoscopic washouts. 2. Obstructive Parotitis: Multiple causes including stones, strictures and papillary obstruction Strictures cause 20% of obstruction Obstruction is caused due to stagnation of mucus plugs. Present with meal time syndrome Trauma to papilla of parotid causes inflammation.
- 40. 5. Granulomatous sialadenitis • Painless swelling of parotid or submandibular glands; chronic condition • Mycobacterial infection: TB and Non TB sialadenitis + tumour like swelling of the gland; without systemic upset. • Sarcoidosis: sarcoid pseudotumour maybe associated with xerostomia. • Cat's scratch, toxoplasmosis, wegener's, syphylis, deep mycosis, radiotherapy.
- 41. 6. Sialadenosis • Sialadenosis: aka sialosis • enlargement of salivary glands • non-inflammatory • non-neoplastic • Parotid is commonly affected. • Associated with: Endocrine disorders: (1) Diabetes mellitus/insipidus; (2) Acromegaly (3) Hypothyroidism (4) Pregnancy. Nutritional status: (1) Anorexia nervosa; (2) Bulimia; (3) Chronic alcoholism; and (4) General malnutrition.
- 42. • Also known as Kuttner’s tumour . • chronic inflammatory reaction secondary to ductal obstruction and subsequent salivary stasis. • Presentation: painful, hard swelling of submandibular salivary gland. • M>F • CT scan: Chronic sclerosing sialadenitis of submandibular gland. 7. Chronic sclerosing sialadenitis
- 43. Classification of Salivary Gland tumours Type Subgroup Examples Epithelial tumours Adenoma Pleomorphic Monomorphic Pleomorphic Adenoma Adenolymphoma(Warthin's tumour) Carcinoma Low Grade High Grade Acinic Cell Carcinoma Adenoid Cyctic Carcinoma Low grade Mucoepidermoid Carcinoma Adenocarcinoma Squamous Cell Carcinoma High grade Mucoepidermoid Carcinoma Non-epithelial tumours Hemangioma; Lymphagioma Lymphomas Primary Lymphomas Secondary Lymphomas Non Hodgkin's lymphoma Sjogren's Syndrome Secondary tumours Local Distant Tumours of Head/neck Skin and bronchus Tumour like Lesions Solid Cystic Benign lymphoepithelial lesion Adenomatoid Hyperplasia Salivary Gland cysts
- 45. 1.Pleomorphic adenoma • Also known as Mixed tumor, Endothelioma, etc. • 75% of all benign salivary tumours(MC) • Parotid gland (85% of cases) > submandibular gland (5% of cases)> minor salivary glands (10% of cases). • F>M ; 4th-5th decade • Epithelial+myoepithelial components • Clinical features: Slowly growing painless, tumour+ facial nerve associated symptoms • 5% Risk of malignant transformation into carcinoma ex pleomorphic adenoma. • Age, smoking habits, alcohol abuse, a diet rich in cholesterol and previous radiation therapy treatments in the face and neck regions, are the risk factors.
- 46. 1) solitary, ovoid, firm to soft with well defined borders; cut surface tan to white 2)Mixture of epithelial, myoepithelial and stroma component.
- 47. Treatment: • Superficial (Patey's operation)/total parotidectomy. • The tumors of the submandibular glands: simple excision procedure+ preservation of adjacent nerves • Minor salivary glands: 5 mm margin should be obtained; wide local excision with cuff of normal tissue. • Parapharyngeal extention- external cervical approach • These tumors do not invade into periosteum. Thus, the bone need not be resected.
- 48. Warthin Tumour • Papillary cystadenoma lymphomatosum • 2nd MC benign salivary tumour. • M>F • MC site: tail of parotid gland(exclusively seen in parotid) • Clinical features: A painless, slow-growing bump in front of the ear, on the bottom of the mouth, or under the chin. • Etiologic factors: Epstein Barr virus infection, tobacco,smoking, autoimmune disease, ionizing radiation, and chronic inflammation. • Malignant transformation of Warthin tumor is extremely rare and accounts for 0.3% of the cases.
- 49. Warthin Tumor • Grossly, Warthin tumor is a well-circumscribed spherical to oval mass. On cut section, there are solid areas and multiple cysts with papillary projections. The cystic spaces often contain mucoid creamy brown or white fluid.
- 51. Oncocytic papillary cystadenoma • Benign minor salivary gland tumour. • Mc site: false vocal cords and ventricles of larynx • Presents with hoarseness of voice and painless mass. • Gross-smooth, rounded, cystic, pedunculated mass. • Treatment- complete surgical excision.
- 52. Myoepithelioma • Origin from contractile myo-epithelial cells lining the acini and ducts of salivary glands. • <1% of all salivary neoplasms • Benign but locally aggressive • 3rd-6th decade • Minor glands>parotid>submandibular gland • Presents asymptomatic, slow growing mass • Micro: spindle shaped plasmacytoid cells. • Treatment: wide local excision
- 53. Monomorphic adenomas • No mesenchymal stromal component; predominantly epithelial. • Benign salivary tumor composed of nests and cords of small basaloid cells with inner ductal epithelial cell • Basal cell, canalicular, sebaceous, clear cell are the types. • Basal cell adenoma is the commonest. • 6th decade • More common in parotid, minor glands of upper lip.
- 54. Canalicular adenoma • Site: Minor salivary glands, mainly upper lip.(1st picture) • <1% of salivary glands tumours • Asymtomatic slow growing mass • Histologically: cells arranged in parallel rows forming 'duct like' structures.(2nd picture) • Treatment: surgical excision
- 55. Oncocytoma • Rare, <1% of benign salivary tumours • 6th decade • Parotid>submandibular> minor glands over palate, buccal mucosa, tongue • Enlarging painless mass • Locally aggressive • Gross: encapsulated, circumscribed • Micro: large eosinophilic cells; mitochondial hyperplasia • Treatment: surgical excision
- 56. Malignant Salivary gland tumors • The main malignant tumour types (from most to least common) are: • Mucoepidermoid carcinoma • Adenoid cystic carcinoma • Acinic cell carcinoma • Squamous cell carcinoma • Adenocarcinoma •
- 57. Muco epidermoid Carcinoma • Most common(29-43%) malignant tumor of the salivary gland in both adults and children, • Parotid>minor SG>submandibular • Arises from the epithelium of the interlobular and intralobular salivary ducts. • F: M ratio 3:2 • Mean age of onset is 5th decade. • Smoking, viral infections, working in rubber manufacturing and prior exposure to radiation.
- 58. Muco epidermoid carcinoma • Symptoms: tenderness, otorrhea, dysphagia, and trismus. • Gross features: Unencapsulated, firm, cysts with mucoid content. • Histology: 3 types of cells; epidermoid, mucous, intermediate cells. • Low grade: slow growing, painless mass, higher % mucinous cells; better prognosis • Intermediate grade: intermediate symtoms; mix of epithelial and mucinous cells • High grade: rapidly enlarging, +/-pain; higher % epithelial cells; worse prognosis
- 60. Management Treatment is influenced by site, stage, grade Stage I, II • Wide local excision- minor salivary gland tumours • High-grade tumors are generally treated with surgical excision with wide margins followed by postoperative radiotherapy • Parotidectomy(superficial/total conservative) for parotid • Submandibular gland excision in submandibular gland tumours. Stage III & IV • Radical excision +/- Neck dissection • +/- post operative radiotherapy
- 61. Adenoid Cystic Carcinoma • 2nd most common malignancy. • 10-15% of all malignant salivary neoplasms • Most common in parotid, sublingual, and minor salivary glands. • M=F, 5th and 6th decade. • ACC is typically an aggressive form of cancer that has a poor long-term outlook. • Known for neurotropism, slow growth, local recurrence, and distant mets.
- 62. Clinical picture • Adenoid cystic carcinoma (ACC) of salivary glands a slow-growing, often asymptomatic mass Pain, paresthesia, facial weakness • Neural invasion in 50%; 25% develop distant mets(lung); skip mets seen along the nerves. • Tumors of the lacrimal gland may cause a bulging eye or changes in vision. • Those affecting the windpipe or voice box may cause respiratory symptoms or changes in speech, respectively.
- 63. Microscopic features: ACC has three histopathologic patterns • Tubular: Intermediate nature • Cribriform: glandular; Best prognosis • Solid pattern: Epithelial nature, tumour necrosis; Best prognosis
- 64. Treatment: • Total parotidectomy • Perineural invasion: ?facial nerve sacrifice • Post operative IMRT(intensity modulated radiotherapy) Prognosis: • Local recurrence: 42% • Distant metastasis: lung • 100% primary site recurrence at 30yrs • 100% lung metastasis at 20 yrs
- 65. Acinic cell Carcinoma • low-grade malignant salivary neoplasm; 6-8% of all salivary malignancies. • Most common site: parotid gland (80%) • Presentation- solitary, slow growing, often painless mass • Most common sites in the oral cavity are the buccal mucosa and upper lip • F>M • 2nd most common salivary malignancy in children (after mucoepidermoid carcinoma.) • 3rd most common salivary malignancy in adults (after mucoepidermoid carcinoma and adenoid cystic carcinoma) • Previous radiation exposure and familial predisposition are the risk factors for ACC.
- 66. Multilocular radiolucent lesion extending from the ascending ramus to periapical area of left mandibular canine. Mandibular canal involvement was clear. sheets of large acinar cells with basophilic to amphophilic cytoplasm with numerous dark-staining granules and round small eccentrically located nuclei. Acinic cell carcinoma
- 67. Squamous cell carcinoma • Malignant epithelial tumor of major salivary glands composed of epidermoid cells. • 0.3-1.5% of salivary gland neoplasms • M>F • Painless mass; ulceration maybe present • Facial palsy in 10%, neck metastasis in 50% and distant metastasis in 10%. • Treatment: Radical excision Neck dissection Post op XRT
- 68. Adenocarcinoma Gross features: • focally circumscribed • Hemorrhagic and necrotic areas Microscopic features: 4 patterns • Solid • Cords • Ducts and tubules • glands
- 69. Polymorphous low grade adenocarcinoma • Aka ' terminal duct carcinoma'. • Originates from intercalated ducts • 2nd most common malignancy of salivary glands • 6th-7th decade • F>M • Painless submucosal mass • Cervical metstasis in 10% • Perineural spread seen • Treatment: complete yet conservative excision.
- 70. Staging of Salivary gland malignancies
- 72. Parotidectomy • Indications: Benign tumours; Malignant tumours; chronic inflammation of the gland. • Incision: Modified blair's incision; facelift incision. • Critical steps 1) Flap elevation(subplatysmal or superficial muscular aponeurotic region) 2) Identification of Facial nerve(Digastric, tragal pointer, tympanomastoid suture line) 3) handling the nerve( tunnel, lift, coagulate, cut) 4) Delivery and closure
- 73. Types of incision • Retro-auricular hairline incision • Modified Blair's incision • Modified facelift incision
- 74. Types of parotidectomy • Extracapsular dissection: Tumour is removed, leaving a parted but intact parotid. Facial nerve is not dissected, unless it lies in close vicinity. • Partial/superficial parotidectomy: The tumor is resected with a cuff of parotid tissue, used for benign lesions and lymph node metastasis into the superficial lobe.
- 75. • Total conservative parotidectomy: Entire gland is removed; for aggressive malignant tumors, deep lobe tumors, sentinel lymph node excision when located in the deep lobe, positive margin after superficial parotidectomy. • Radical parotidectomy: The entire gland and the facial nerve is removed, mostly used when preoperative facial paralysis is well established, or circumferential involvement of the nerve by malignant tumor is encountered. • Simultaneous nerve grafting or other facial reanimation procedures can be employed
- 76. Landmarks used for facial nerve identification: • Tragal pointer • Posterior belly of digastric • Mastoid process • Tympanomastoid suture line • Retrograde dissection Management: • If nerve is non functional preoperatively: excision done • Excise if tumour is adherant to it • In case of adenoid cystic carcinoma: if sectioned nerve is involved excise till free stump is obtained on frozen section • Immediate cable grafting can be done with sural or GAN.
- 77. Submandibular gland excision • Benign Tumours: Excision in supracapsular plane • Malignant Tumours: Wide excision + neck dissection • Clinically high-grade tumours: treat aggressively with excision of the gland plus a 2 cm margin of apparently healthy tissue. • Resection of involved nerves with microscopic negative margins is desirable. • Large infiltrative tumours with bony involvement: composite resection of tumour, adjacent soft tissue cuff and bony resection. • N0 neck: clearance of nodes+ selective neck dissection (levels 1 and 2A).
- 78. Submandibular gland excision Excision involves 6 phases Incision ( horizontal skin crease, 2 fingers breadth below ramus of mandible) Superior(subplatysmal) flap is raised Identify and Preserve mandibular marginal nerve Superficial lobe mobilised Dissection of deep lobe and identification of lingual nerve Proximal part facial A is ligated; duct is transected Wound closure
- 80. Non Surgical Management • For a salivary gland tumor, radiation therapy is most often used in combination with surgery, depending on the size, grade, extent, and location of the cancer and whether there are some cancer cells in the margin around the tumor removed by surgery. • If radiation therapy is recommended, it should be started within 8 weeks of the surgery. Radiation therapy may also be given along with chemotherapy • There are 2 main types of radiation therapy used for salivary gland cancer: • External beam radiation • Internal beam radiation • Chemotherapy has limited role in terms of salivary gland tumours
- 82. Recommendations • USG guided FNAC is recommended for all salivary tumours and cytology. • Adjuvant radiotherapy (RT) following surgery is recommended for all malignant submandibular tumours except in cases of small, low-grade tumours that have been completely excised. • In the event of intra-operative tumour spillage, most cases need long-term follow-up for clinical observation only. The merits of adjuvant RT ought to be discussed. • As a general principle, if the facial nerve function is normal pre-operatively then every attempt to preserve facial nerve function should be made during parotidectomy and if the facial nerve is divided intra-operatively then immediate microsurgical repair (with an interposition nerve graft if required) should be considered. • Where malignant parotid tumours lie in close proximity to the facial nerve there should be a low threshold for adjuvant RT. • Adjuvant RT should be considered in high grade or large tumours or in cases where there is incomplete or close resection margin. • Adjuvant RT should be prescribed on the basis of clinical factors in addition to histology and grade, e.g. stage, pre-operative facial weakness, positive margins, peri-neural invasion and extracapsular spread.
- 83. References: • Sood, S et al. “Management of Salivary Gland Tumours: United Kingdom National Multidisciplinary Guidelines.” The Journal of laryngology and otology vol. 130,S2 (2016): S142-S149. doi:10.1017/S0022215116000566 • Cantù, Giulio. “Adenoid cystic carcinoma. An indolent but aggressive tumour. Part B: treatment and prognosis.” Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale vol. 41,4 (2021): 296-307. doi:10.14639/0392-100X- N1729 • Lahouti AH, Rao RA. Acinic cell carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/salivaryglandsaciniccell.html • Weinreb, Ilan. “Hyalinizing clear cell carcinoma of salivary gland: a review and update.” Head and neck pathology vol. 7 Suppl 1,Suppl 1 (2013): S20-9. doi:10.1007/s12105-013-0466-8 • Ishikawa S, Ishikawa H, Fuyama S, Kobayashi T, Waki T, Taira Y, Iino M. Report of a case of acinic cell carcinoma of the upper lip and review of Japanese cases of acinic cell carcinoma of the minor salivary glands. J Clin Exp Dent. 2016 Dec 1;8(5):e638-e644. doi: 10.4317/jced.53049. PMID: 27957284; PMCID: PMC5149105.
- 84. Thank you!!!