Changing the Paradigm of CMV Management: New Science and More Choices for Challenging Cases in the HCT Setting
•
0 gostou•43 visualizações

Roy F. Chemaly, MD, MPH, FIDSA, FACP, and Genovefa Papanicolaou, MD, FIDSA, prepared useful practice aids pertaining to cytomegalovirus for this CME activity titled "Changing the Paradigm of CMV Management: New Science and More Choices for Challenging Cases in the HCT Setting." For the full presentation, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/38UNLwZ. CME credit will be available until March 19, 2021.

Recomendados
Recomendados
Mais conteúdo relacionado
Mais de PVI, PeerView Institute for Medical Education
Mais de PVI, PeerView Institute for Medical Education (20)
Último
Último (20)
Changing the Paradigm of CMV Management: New Science and More Choices for Challenging Cases in the HCT Setting
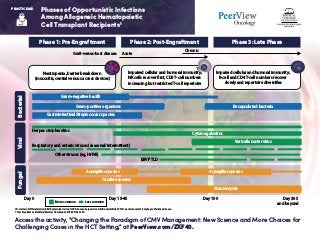
- 1. Phases of Opportunistic Infections Among Allogeneic Hematopoietic Cell Transplant Recipients1 Access the activity, “Changing the Paradigm of CMV Management: New Science and More Choices for Challenging Cases in the HCT Setting,” at PeerView.com/ZXF40. PRACTICE AID CD: cluster of differentiation; EBV: Epstein-Barr virus; HHV6; human herpesvirus 6; NK: natural killer; PTLD: post-transplant lymphoproliferative disease. 1. Tomblyn M et al. Biol Blood Marrow Transplant. 2009;15:1143-1238. Phase 1: Pre-Engraftment BacterialViralFungal Phase 2: Post-Engraftment Phase 3: Late Phase Neutropenia, barrier breakdown (mucositis, central venous access devices) Gram-negative bacilli Encapsulated bacteria Varicella zoster virus Aspergillus speciesAspergillus species Candida species Pneumocystis Gastrointestinal Streptococcus species Gram-positive organisms Impaired cellular and humoral immunity; NK cells recover first, CD8 T-cell numbers increasing but restricted T-cell repertoire Impaired cellular and humoral immunity; B-cell and CD4 T-cell numbers recover slowly and repertoire diversifies Graft-versus-host disease: Day 0 Day 15-45 Day 100 More common Day 365 and beyond Acute Chronic Less common Herpes simplex virus Respiratory and enteric viruses (seasonal/intermittent) Other viruses (eg, HHV6) Cytomegalovirus EBV PTLD
- 2. PRACTICE AID Access the activity, “Changing the Paradigm of CMV Management: New Science and More Choices for Challenging Cases in the HCT Setting,” at PeerView.com/ZXF40. Preventing CMV infection and Disease in HCT Recipients1 Comparison of Current CMV Prevention Strategies The Newest FDA-Approved Drug for CMV Prophylaxis in Allogeneic HCT Recipients: Key Characteristics of Letermovir Prophylaxis Antivirals administered to all at-risk patients for a defined period of time following transplantation CMV DNA test (at least once weekly) Antiviral therapy started when viral load exceeds a certain threshold Effectively prevents early CMV reactivation High rates of medication side effects Increased drug cost Risk for delayed-onset CMV disease Preemptive Therapy 3,4-dihydro-quinazoline-4-yl-acetic acid derivative Only active against CMV (no activity against HSV) Uncommon, mainly GI (gastritis, nausea), dyspnea, hepatitis 93% in feces, mostly as unchanged drug CMV prophylaxis in CMV-seropositive HCT recipients Inhibits terminase complex subunit pUL56 94% healthy individuals; 35% in HCT (increased to 85% with cyclosporine) Reduces exposure to voriconazole; increases exposure to tacrolimus, cyclosporine, midazolam; letermovir exposure increased with cyclosporine 480 mg daily (240 mg if administered with cyclosporine) for prophylaxis in HCT; no dose adjustment for renal dysfunction Use of letermovir for CMV prophylaxis in CMV-seronegative kidney transplant recipients Principle Advantages Disadvantages Reduced medication cost Lower risk of drug toxicity Allows immune reconstitution DoesnotpreventearlyCMVreactivation Escape CMV infections (not detected by weekly CMV NAT) Burden, logistics, cost of weekly surveillance labs Molecule Mechanism of action Spectrum of activity Bioavailability Excretion Dosing Side effects Drug interactions Current FDA approval indication Ongoing trials
- 3. PRACTICE AID Access the activity, “Changing the Paradigm of CMV Management: New Science and More Choices for Challenging Cases in the HCT Setting,” at PeerView.com/ZXF40. CMV: cytomegalovirus; GCV: ganciclovir; HCT: hematopoietic stem cell transplantation; NAT: nucleic acid testing; QTc: corrected QT interval; SOT: solid organ transplantation; VGCV: valganciclovir. 1. El Helou G, Razonable RR. Infect Drug Resist. 2019;12:1481-1491. Mechanism of action • 2ʹ-deoxyguanosine analog • Competitive binding to UL54 • DNA polymerase • Needs phosphorylation by CMV (UL97 encoded) and host kinases • Virostatic agent • Pyrophosphate analog • Noncompetitive inhibitor of many RNA and DNA polymerases (UL54 DNA polymerase in CMV) • Virostatic agent • Acyclic monophosphate deoxycytidine analog • Competitive substrate of UL54 DNA polymerase leads to inhibition of viral DNA synthesis through incorporation into growing viral DNA chain • Virostatic agent • Inhibits viral terminase complex, encoded by genes UL56, UL51, and UL89 • Virostatic agent Indications/ uses • CMV retinitis • CMV prophylaxis SOT Non-FDA uses • CMV disease • CMV preemptive strategy • CMV prophylaxis in HCT • CMV retinitis Non-FDA uses • Second line for GCV- resistant CMV disease therapy, prophylaxis, or preemptive therapy • CMV retinitis Non-FDA uses • Second line for GCV- resistant CMV disease therapy, prophylaxis, or preemptive therapy • CMV prophylaxis in CMV-seropositive HCT recipients Formulations • GCV IV only • VGCV oral • IV only • IV only • Lipid conjugate not yet approved (brincidofovir) • IV and oral Adverse effects • Pancytopenia and myelosuppression (leukopenia/ neutropenia++) • Renal injury • Diarrhea • Less common: pruritus, nausea, fever, torsade de pointe • Renal injury • Electrolytes wasting • Neutropenia • Less common: headache, diarrhea, fever, QTc prolongation • Renal injury • Proteinuria • Neutropenia • Ocular toxicity (iritis, uveitis, amblyopia) • Less common: headaches, shivering, rash, alopecia, dyspnea • Uncommon, mainly GI (gastritis, nausea), dyspnea, hepatitis Resistance mechanism • Mutations in UL97 gene prevent activation of drug • Mutations in UL54 gene prevent binding to DNA polymerase (may confer cross-resistance with all DNA-polymerase active antivirals) • Mutations in UL54 gene prevent binding to DNA polymerase (may confer cross-resistance with all DNA-polymerase active antivirals) • Mutations in UL54 gene prevent binding to DNA polymerase (may confer cross-resistance with all DNA-polymerase active antivirals) • Mutations in UL56 gene • Less commonly, mutations in UL51 or UL89 genes Characteristics of Antiviral Drugs Approved for CMV Ganciclovir and Valganciclovir Foscarnet Cidofovir Letermovir Preventing CMV infection and Disease in HCT Recipients1
- 4. Access the activity, “Changing the Paradigm of CMV Management: New Science and More Choices for Challenging Cases in the HCT Setting,” at PeerView.com/ZXF40. PRACTICE AID A Closer Look at Resistant and Refractory CMV Infection and Disease in HCT Recipients1,2 Risk Factors for CMV Resistance in HCT Recipientsa Summary of the Definitions of Refractory CMV Infection and Disease and Antiviral Drug Resistance for Use in Clinical Trials Host factors Host factors Viral factors • Prolonged antiviral CMV drug exposure (>3 mo) • Previous antiviral CMV drug exposure • Recurrent CMV infection • Inadequate antiviral CMV drug absorption and bioavailability • Inadequate antiviral CMV oral prodrug conversion • Variation in antiviral CMV drug clearance • Subtherapeutic antiviral CMV drug level • Poor patient compliance with antiviral drug regimen • T-cell depletion • Haploidentical, allogeneic, or cord blood HCT • Delayed immune reconstitution • CMV-seropositive recipient and CMV-seronegative donor • Treatment with antithymocyte antibodies • Active GVHD • Young age • Congenital immunodeficiency syndromes Refractory CMV infection Probable refractory CMV infection Refractory CMV end-organ disease Probable refractory CMV end-organ disease Antiviral drug resistance • CMV viral load rise while receiving treatment (after >2 wk of adequate dosing) • Failure of CMV viral load to fall despite appropriate treatment • Rise in CMV viral load after initial decline while receiving appropriate treatment • Intermittent low-level CMV viremia • High CMV viral loads Host factors CMV viremia that increasesb after at least 2 wk of appropriately dosed antiviral therapy Worsening in signs and symptoms or progression into end-organ disease after at least 2 wk of appropriately dosed antiviral therapy Viral genetic alteration that decreases susceptibility to one or more antiviral drugsd Persistent viral loadc after at least 2 wk of appropriately dosed antiviral therapy Lack of improvement in signs and symptoms after at least 2 wk of appropriately dosed antiviral drugs
- 5. Access the activity, “Changing the Paradigm of CMV Management: New Science and More Choices for Challenging Cases in the HCT Setting,” at PeerView.com/ZXF40. PRACTICE AID A Closer Look at Resistant and Refractory CMV Infection and Disease in HCT Recipients1,2 a Most of the risk factors for CMV resistance pertain to solid organ transplant recipients as well, in addition to graft rejection (instead of GVHD) and CMV-seropositive donor and CMV-seronegative recipient. b More than 1 log10 increase in CMV DNA levels in blood or serum and determined by log10 change from the peak viral load within the first week to the peak viral load at ≥2 weeks as measured in the same laboratory with the same assay. c CMV viral load at the same level or higher than the peak viral load within 1 week but <1 log10 increase in CMV DNA titers done in the same laboratory and with the same assay. d Known examples involve genes involved in antiviral drug anabolism (eg, UL97-mediated phosphorylation of ganciclovir), the antiviral drug target (eg, UL54, UL97, UL56/89/51), or compensation for antiviral inhibition of biological function (eg, UL27). CMV: cytomegalovirus; GVHD: graft-vs-host disease; HCT: hematopoietic cell transplantation; SOT: solid organ transplantation. 1. Chemaly RF et al. Clin Infect Dis. 2019;68:1420-1426. 2. Papanicolaou GA et al. Clin Infect Dis. 2019;68:1255-1264. Maribavir for Refractory or Resistant CMV Infections Cl N N N H HO O O O H H Cl A Phase 3, Multicenter, Randomized, Open-Label, Active-Controlled Study to Assess the Efficacy and Safety of Maribavir Treatment Compared to Investigator-Assigned Treatment in Transplant Recipients With Cytomegalovirus (CMV) Infections That Are Refractory or Resistant to Treatment With Ganciclovir, Valganciclovir, Foscarnet, or Cidofovir • Clinicaltrials.gov/NCT02931539 • Status: recruiting HCT + SOT Side effects: dysgeusia and nausea, vomiting Phase 3 trial Completed phase 3 trial Within 6 weeks, 67% of patients had undetectable plasma CMV DNA Refractory or resistant CMV infection