Bursitis
•Transferir como PPTX, PDF•
13 gostaram•9,191 visualizações

This short presentation is to help those in medical fields to have a summary knowledge of what bursitis is and it can also help students in their assignments and or course works. It contains what bursae are, what bursitis means, causes, risk factors, common sites, clinical features, how to diagnose bursitis, other conditions that can mimic bursitis, how to prevent bursitis and management.

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Bursitis
Semelhante a Bursitis (20)
Último
Último (18)
Bursitis
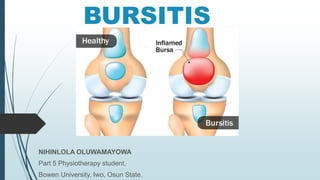
- 1. BURSITIS NIHINLOLA OLUWAMAYOWA Part 5 Physiotherapy student, Bowen University, Iwo, Osun State.
- 2. OUTLINE INTRODUCTION TO BURSA AND FUNCTIONS TYPES OF BURSA BURSITIS DEFINITION CAUSES RISK FACTORS COMMON SITES CLINICAL FEATURES DIAGNOSIS DIFFERENTIAL DIAGNOSIS PREVENTION TREATMENT • TREATMENTIN BURSITIS DUE TO FRICTION • IN INFECTIVE BURSITIS REFERENCES
- 3. INTRODUCTION TO BURSA AND FUNCTIONS Bursa is a thin membranous sac lined with synovial membrane situated at the ends or certain important locations of the bones where tendons, etc. FUNCTIONS To prevent friction between two structures like tendons and bones that is liable to be rubbed against each other. To prevent wear and tear of muscles and tendons. To protect the structures from pressure and injury. 3
- 5. TYPES OF BURSA They’re filled with fluid that helps ease rubbing and friction between tissues like bone, muscle, tendons, and skin. True bursa: are normally present in the body at certain important situations like beneath the acromion, elbow, knee, heel, etc. False bursa: are also called as adventitious bursa. They develop due to external trauma, pressure. 5
- 6. BURSITIS DEFINITION Is the inflammation of bursae. This occurs because of bacterial infection or mechanical irritation. Because of which the bursitis may be infective or irritative caused by excessive pressure or friction. Also sometimes due to gouty deposit. It can affect any joint, but is most common in the shoulders, hips, elbows or knees. 6
- 7. CAUSES • Trauma may be due to a single blow or repetitive trauma. • Infection (acute or chronic) e.g. tuberculosis. • Metabolic disorders, For example gout. •Abnormal external pressures, For example, hip ischial- tuberosity in prolong sitting. • Inflammatory disorders, such as rheumatoid arthritis. • Unaccustomed activity, exercise or ill-fitting shoes etc. •Due to excessive pressure, friction. 7
- 8. RISK FACTORS Age: Bursitis becomes more common with aging. Occupations or hobbies: risk of developing bursitis increases in work or hobby that requires repetitive motion or pressure on particular bursae. Examples include carpet laying, gardening and playing a musical instrument etc. History of other medical conditions: certain systemic diseases and conditions (rheumatoid arthritis, gout and diabetes). Overweight can increase the risk of developing hip and knee bursitis. 8
- 9. COMMON SITES Upper Limbs — Sub-acromion — Olecranon Lower Limbs — Pre-patellar — Tendo-Achilles — Medial side of the great toe — Lateral side of the little toe. 9
- 10. CLINICAL FEATURES Pain, swelling, redness, tenderness, painful and reduced joint range of motion, limping is seen in gluteal bursitis, etc. 10
- 11. DIAGNOSIS Physical Test: involves taking symptoms history and do a physical exam to see if the joint is swollen. You might also have Imaging tests: X-rays can rule out other problems that might be causing pain. MRI and ultrasound give an image of your joint. Plain X-ray helps to detect the calcaneal and the retro- calcaneal spurs. Lab tests: involves the use of a needle to take a bit of fluid from the bursa and test it for signs of infection. 11
- 12. DIFFERENTIAL DIAGNOSIS Tendonitis Cellulitis Osteoarthritis Rheumatoid arthritis Septic arthritis Fracture Ligamentous injury 12
- 13. PREVENTION You can’t always prevent bursitis, but some steps can lower your risk. Use cushions or pads when you’re resting a joint on a hard surface, like if you’re kneeling or sitting. If you play sports, mix things up so you don’t make the same motions all the time. Warm up and stretch before you play, and always use proper form. clean any cuts on elbows and knees to prevent infections 13
- 14. PREVENTION Warming up and stretching before strenuous activities to protect your joints from injury. Take breaks often when you’re making the same motions over and over again. Use good posture all day. Keep a healthy body weight. If something hurts, stop doing it and check with your doctor. Exercising: strengthening your muscles can help protect your affected joint. 14
- 15. TREATMENT IN BURSITIS DUE TO FRICTION • Rest to the part. • Thermotherapy: Ultrasound, TENS therapies, etc. • Cryotherapy in initial stages. • Restricted weight bearing. • Isometric exercises to the affected part. • Muscle strengthening exercises. • Joint mobilization if there is restriction. • Injection of hydrocortisone in intractable cases. • Excision of the bursa, if chronic and troublesome. 15
- 16. TREATMENT IN INFECTIVE BURSITIS • Appropriate antibiotics Cryotherapy • Rest of the measures is same as above. • Appropriate supports like felt pad, footwear modifications etc. • Avoiding repeated frictional movements. Deep friction massage. 16
- 17. TREATMENT IN INFECTIVE BURSITIS For example—shoulder abduction in sub deltoid bursa. • Relaxed passive movements to avoid friction. • Active limited ROM exercises with strong isometrics. • Progressive resistive exercises. • Deep heating like Ultrasound , Short Wave Diarthermy, TENS, etc. • Active exercises to the unaffected joints. • Isometrics with limb in elevation helps considerably. 17
- 18. REFERENCES Gitesh Amrohit (2012)The Pocketbook for Physiotherapists. 2nd ed. Pg. 317 Jaypee Brothers Medical Publishers (P) Ltd: India John Ebnezar(2011) Essentials of Orthopedics for Physiotherapists. 2nd ed. Pg. 34 Jaypee Brothers Medical Publishers (P) Ltd: India Fauci, Anthony S., and Carol Langford. Harrisons’s rheumatology. McGraw Hill Professional, 2010. Aaron, Daniel L., et al. “Four common types of bursitis: diagnosis and management.” Journal of the American Academy of Orthopaedic Surgeons 19.6 (2011): 359-367. 18
- 20. 20