
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Inflammatory bowel disease
Semelhante a Inflammatory bowel disease (20)
Mais de Mohammad Rehan
Mais de Mohammad Rehan (11)
Último
Último (20)
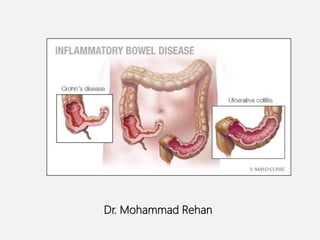
Inflammatory bowel disease
- 2. • It includes a group of chronic disorders that cause inflammation or ulceration in large and small intestines. • 2 major types: Ulcerative colitis (UC) and Crohn’s disease (CD) INCIDENCE- Highest incidence in Europe, the United Kingdom, and North America. Urban areas > rural areas. high socioeconomic classes > lower socioeconomic classes. INFLAMMATORY BOWEL DISEASE
- 3. • Recently two studies, both from northern India, reported a population prevalence of ulcerative colitis (UC) of approximately 42 per 100,000 . • No such population based study is available for crohn’s disease.
- 4. EPIDEMIOLOGY
- 5. ETIOPATHOGENESIS Exact cause is unknown. • Genetic factors • Immunological factors • Microbial factors • Psychosocial factors
- 7. GENETIC FACTORS • Ulcerative colitis is more common in DR2-related genes. • Crohn’s disease is more common is DR5 DQ1 alleles. • 3-20 times higher incidence in first degree relatives.
- 8. IMMUNOLOGIC FACTORS • Defective regulation of immunosuppression. • Activated CD+4 cells activate other inflammatory cells like macrophages & B-cells or recruit more inflammatory cells by stimulation of homing receptor on leucocytes & vascular epithelium resulting in inflammation of mucosa and sub mucosa.
- 11. PATHOGENESIS OF IBD American Gastroenterological Association Institute, Bethesda, MD. Sartor RB. Nat Clin Pract Gastroenterol Hepatol. 2006;3:390- 407. Normal Gut Tolerance- controlled inflammation (Infection, NSAID, other) Complete Healing Chronic Inflammation Genetically Susceptible Host Acute Inflammation ↓ Immunoregulation, failure of repair or bacterial clearance Acute injury Environmental triggers
- 12. PATHOLOGY Macrocopic features •Ulcerative colitis Usually involves rectum & extends proximally to involve all or part of colon. Spread is in continuity. About 40–50% of patients have disease limited to the rectum and rectosigmoid. 30–40% have disease extending beyond the sigmoid but not involving the whole colon, and 20% have a total colitis (10–20% patients have backwash ilietis).
- 14. Mild disease- erythematous & sand paper appearance (fine granular surface) of mucosa. Moderate-marked erythema, coarse granularity, contact bleeding & no ulceration. Severe- spontaneous bleeding, edematous & ulcerated (collar button ulcer) mucosal surface. Long standing-epithelial regeneration so pseudopolyps , mucosal atrophy & disorientation leads to a precancerous condition. Eventually can lead to shortening and narrowing of colon. Fulminant disease-Toxic colitis/ megacolon/ perforation
- 16. MICROSCOPIC FEATURES Limited to mucosa & sub mucosa Crypts atrophy & irregularity Superficial erosion Diffuse mixed inflammation Basal lymphoplasmacytosis
- 19. MACROSCOPIC FEATURES • Crohn’s disease Can affect any part of GIT. Transmural involvement. Segmental with skip lesions. Cobblestone appearance of mucosa. Creeping fat- adhesions & fistula.
- 22. MICROSCOPIC FEATURES • Aphthous ulcerations. • Focal crypt abscesses. • Granuloma formation- pathognomic. • Submucosal or subserosal lymphoid aggregates. • Transmural involvement with fissure formation.
- 25. CLINICAL FEATURES • Ulcerative colitis Diarrhea Rectal bleeding Tenesmus Passage of mucus Crampy abdominal pain Systemic symptoms fever, weight loss Extra intestinal manifestations
- 26. • Physical signs Proctitis – Tender anal canal & blood on rectal examination. Extensive disease-tenderness on palpation of colon. Toxic colitis-severe pain &bleeding. If perforation-signs of peritonitis.
- 27. 1. Truelove SC, et al. Br Med J. 1955;2:1041-1045. 2. Sandborn WJ. Curr Treat Options Gastroenterol.1999;2:113-118. CLINICAL SEVERITY OF UC Mild Moderate Severe Fulminant Bowel movement <4/day Intermediate >6 >10 Blood in stool Intermittent moderate Frequent Continuous Temperature Normal <37.5° >37.5° >37.5° Pulse Normal <90bpm >90 bpm >90 bpm Hemoglobin Normal >75% <75% Transfusion required ESR <30 mm/hour >30 mm/hour >30 mm/hour Clinical signs Abdominal tenderness Abdominal distension and tenderness
- 28. EXTRA INTESTINAL MANIFESTATIONS OF ULCERATIVE COLITIS
- 29. DIAGNOSIS • Laboratory tests • Endoscopy • Radiography • Tissue Biopsy
- 30. LABORATORY TESTS • Hemogram ESR is increased Platelet count-increased Hemoglobin-decreased • C-reactive protein is increased • Fecal Calprotectin levels correlate with histological inflammation, predict relapses & detect pouchitis. • Fecal lactoferrin- high levels indicate intestinal inflammation.
- 31. BARIUM ENEMA
- 32. BARIUM ENEMA • Fine mucosal granularity- earliest radiological change. • Superficial ulcers seen • Collar button ulcers- s/o mucosal penetration • Pipe stem appearance- loss of haustrations • Narrow & short colon- • Ribbon contour colon
- 33. SIGMOIDOSCOPY • Always abnormal • Loss of vascular patterns • Granularity • Friability • Ulceration
- 34. Colonoscopy with acute ulcerative colitis: severe colon inflammation with erythema, friability, and exudates.
- 36. CLINICAL FEATURES ILEAL CROHN’S DISEASE Abdominal pain Diarrhea Weight loss Low grade fever JEJUNOILEITIS - associated with a loss of digestive and absorptive surface, resulting in Malabsorption Steatorrhea
- 37. Colitis and perianal disease • Bloody diarrohea • Passage of mucus • Lethargy • Malaise • Anorexia • Weight loss Contd. Clinical features
- 38. GASTRODUODENAL DISEASE – • Symptoms and signs of upper GI tract disease include nausea, vomiting, and epigastric pain. • The second portion of the duodenum is more commonly involved than the bulb. • Patients with advanced gastro duodenal CD may develop a chronic gastric outlet obstruction.
- 39. DIAGNOSIS • Laboratory tests • Endoscopy • Radiography • Biopsy • CT enterography
- 40. LABORATORY TESTS • Anemia • Leukocytosis • ESR-elevated • CRP-elevated • Hypoalbuminemia
- 41. BARIUM ENEMA String sign Represents long areas of circumferential inflammation and fibrosis, resulting in long segments of luminal narrowing.
- 42. COLONOSCOPY
- 43. • Endoscopic features of CD include rectal sparing, aphthous ulcerations, fistulas, and skip lesions. • Colonoscopy allows examination and biopsy of mass lesions or strictures and biopsy of the terminal ileum. • Upper endoscopy is useful in diagnosing gastroduodenal involvement in patients with upper tract symptoms
- 45. CT- ENTEROGRAPHY • Mural hyper enhancement. • Stratification. • Engorged vasa recta. • Perienteric inflammatory changes.
- 48. TREATMENT LIFE STYLE CHANGES DIET CHANGE DRUGS SURGERY
- 49. DIETARY CHANGES Eating : Low-fat foods. Smaller, more frequent meals. Avoiding : foods high in undigestible fiber. Refined sugars .
- 50. LIFESTYLE CHANGES NO SMOKING REDUCING STRESSDOING EXERCISE TAKING REST
- 51. Therapeutic approach for IBD
- 52. DRUGS • 5-ASA agents • Glucocorticoids • Antibiotics • Immunosuppresants • Biological therapy
- 53. 5-ASA AGENTS • Sulfasalazine – combination of 5-aminosalicylic acid( anti inflammatory ) + sulfapyradine-antibacterial). Partially absorbed in jejunum but remainder passes in colon Therapeutic action –inhibition of P.G.s & leukotriene synthesis, free radical scavanging, free radical scavanging, impairement of white cell adhesion and function, inhibition of cytokine synthesis. • Mesalamine group (coating 5-ASA with acrylic resins), e.g. Asacol, Pentasa, Balsalazide (prodrug of 5-ASA). • Olsalazine (5-ASA dimer cleaves in colon).
- 55. Distribution of 5-ASA Preparations Oral •Varies by agent: may be released in the • distal/terminal ileum, or colon1 Suppositories • Reach the upper rectum2,5 • (15-20 cm beyond the anal verge) Liquid Enemas • -May reach the splenic flexure2-4 • -Do not frequently concentrate in the rectum3 Topical Action of 5-ASA: Extent of Disease Impacts Formulation Choice 1. Sandborn WJ, et al. Aliment Pharmacol Ther. 2003;17:29-42; 2. Regueiro M, et al. Inflamm Bowel Dis. 2006;12:972–978; 3. Van Bodegraven AA, et al. Aliment Pharmacol Ther. 1996; 10:327-332; 4. Chapman NJ, et al. Mayo Clin Proc. 1992;62:245-248; 5. Williams CN, et al. Dig Dis Sci. 1987;32:71S-75S.
- 56. Use • Mainstay of OPD treatment for mild to moderate active UC & Crohns colitis. • Maintaining remission • May reduce risk of colorectal cancer Adverse effects • Nausea, headache, epigastric pain, diarrhoea, hypersensitivity, pancreatitis • Caution in renal impairment, pregnancy, breast feeding
- 57. GLUCOCORTICOIDS • Anti inflammatory agents for moderate to severe relapses (including IV treatment; enemas for acute proctitis) • Inhibition of inflammatory pathways. • No role in maintenance therapy • Prednisone-40-60mg/day • Budesonide- 9mg/dl used for 2-3 months & then tapered.
- 58. ANTIBIOTICS • Metronidazole is effective in active inflammatory, fistulous & perianal Crohn’s Disease. Dose-15-20mg/kg/day in 3 divided doses. • Ciprofloxacin 500mg BD. • Rifaximin. • No role of antibiotics in active/quiescent UC.
- 59. IMMUNOSUPPRESANTS • Thiopurines- Azathioprine, 6-mercaptopurine. • Methotrexate • Cyclosporine Reduce inflammation by suppressing immune system’s response (which might damage digestive tissue) invading virus or bacterium. • Used in patients unresponsive to steroid & amino salicylates
- 60. CYCLOSPORINE Preventing clonal expansion of T cell subsets. Use • Steroid sparing • Active and chronic disease Side effects Minor: tremor, paresthesias, malaise, headache gingival hyperplasia, hirsutism. Major: renal impairment, infections, neurotoxicity
- 61. BIOLOGICAL THERAPY Infliximab Anti TNF monoclonal antibody. Binds to TNF trimers with high affinity, preventing cytokine from binding to its receptors. It also binds to membrane-bound TNF- a and neutralizes its activity & also reduces serum TNF levels. • Use • Fistulizing CD • Severe active CD • Refractory/intolerant of steroids or immunosuppression • Side effects • Infusion reactions • Sepsis • Reactivation of Tuberculosis • Increased risk of Tuberculosis
- 62. • Newer Biologics 1) Adalimumab 2) Certolizumab 3) Golimumab
- 63. OTHER MEDICATIONS Anti- diarrheal - Loperamide (Imodium) Laxatives - senna, bisacodyl Pain relievers- acetaminophen (Tylenol). Iron supplements
- 64. SURGERY Ulcerative colitis Indications: • Fulminating disease. • Chronic disease with anemia, frequent stools, urgency & tenesmus. • Steroid dependent disease. • Risk of neoplastic change. • Extra intestinal manifestations. • Severe hemorrhage or stenosis.
- 65. • Reconstructive Proctocolectomy with ileoanal pouch. • Proctocolectomy & ileostomy. • Rectal & anal dissection. • Colectomy with ileorectal anastomosis. • Ileostomy with intra abdominal pouch. Surgery in ulcerative colitis
- 66. OTHERS • Proctocolectomy & ileostomy. • Rectal & anal dissection. • Colectomy with ileorectal anastomosis. • Ileostomy with intra abdominal pouch.
- 67. SURGERY IN CROHN’S DISEASE • Ileocaecal resection. • Segmental resection. • Colectomy & ileorectal anastamosis. • Temporary loop ileostomy. • Proctocolectomy. • Strictureplasty.
- 70. DIFFERENTIAL DIAGNOSIS OF UC AND CD