Recomendados

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a HJS_HIVSurveyProject
Semelhante a HJS_HIVSurveyProject (20)
Mais de Mary Beth Levin
Mais de Mary Beth Levin (20)
HJS_HIVSurveyProject
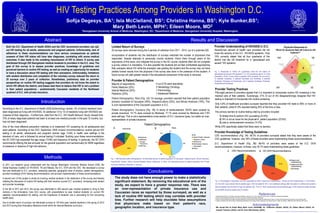
- 1. HIV Testing Practices Among Providers in Washington D.C. Sofija Degesys, BA1; Isla McClelland, BS1; Christina Hanna, BS1; Kyle Bunker,BS1; Mary Beth Levin, MPH1; Eileen Moore, MD2 Abstract 1Georgetown University School of Medicine, Washington, DC; 2Department of Medicine, Georgetown University Hospital, Washington, Introduction Methods Conclusions References Acknowledgments Georgetown University 1. Global Business Coalition on HIV/AIDS, Tuberculosis and Malaria. Why Aren’t D.C. Doctors Testing for HIV? 2010 Nov 17 <http://www.gbcimpact.org/node/2897>. 2. District of Columbia Department of Health. The District of Columbia HIV/AIDS Epidemiology 2008 Update. 3. District of Columbia Department of Health and George Washington University School of Public Health and Health Services. District of Columbia HIV/AIDS Behavioral Surveillance Summary Report 2008. 4. Centers for Disease Control and Prevention. Revised Recommendations for HIV Testing of Adults, Adolescents, and Pregnant Women in Health Care Settings. MMWR Morb Moral Wkly Rep. 2006 Sep 22. Results and Discussion Both the D.C. Department of Health (DOH) and the CDC recommend providers use opt- out HIV testing for all adults, adolescents and pregnant patients. Unfortunately, lack of adherence to these recommendations can have serious consequences as patients unaware of their HIV status will have later diagnoses, correlating with worse medical outcomes. It also leads to the unwitting transmission of HIV to others. A survey was distributed through 520 Georgetown medical students to providers in the D.C. area. The goal of this survey is to assess provider practices, knowledge of guidelines and perceived barriers to routine HIV testing, as well as creating an opportunity for students to have a discussion about HIV testing with their preceptors. Unfortunately, limitations with student distribution and completion of the voluntary survey reduced the return to 25 surveys over 2 years of collection. Nonetheless, preliminary data on provider perspectives on routine HIV testing suggests that providers do not know the extent to which HIV affects the district, and biases lead them to believe that HIV is not a problem in their patient populations - predominantly Caucasian residents of the Northwest quadrant of D.C. with private insurance. According to the D.C. Department of Health 2008 Epidemiology Update, 3% of district residents have been diagnosed as living with HIV/AIDS. An additional 1/3 to 1/2 of residents living with HIV/AIDS are unaware of their diagnosis.1,2 Furthermore, data from the D.C. HIV Health Behavior Study3 showed that 75% of newly diagnosed patients had been to at least one medical provider in the past 12 months, but had not been diagnosed. One of the most effective prevention methods is to implement HIV screening for all adolescents and adult patients. According to the CDC September 2006 revised recommendations4 routine opt-out HIV testing in all adults, adolescents and pregnant women (age 13-64) in health care settings is the standard of care, and is followed by annual testing if indicated. Building upon these recommendations, the DC DOH has expanded the age range (13-84) and frequency of testing. In particular, the DC DOH recommends offering the test annually for the general population and semiannually for MSM regardless of presence or absence of high-risk behavior. In 2011, our research group collaborated with the George Washington University Medical School (GW); the Global Business Coalition on HIV/AIDS, TB and Malaria, the D.C. DOH and the CDC. We developed a survey that was distributed to D.C. providers, assessing specialty, geographic area of practice, patient demographics, provider knowledge of HIV testing recommendations, and provider implementation of these recommendations. A second arm of this project is aimed at involving medical students in the distribution of the survey and thereby initiating the discussion of routine HIV testing with their mentors (current D.C. providers), increasing both student and provider knowledge. In the fall of 2011 and 2012, the survey was distributed to 400 second year medical students to bring to their mentors in the Ambulatory Care (AC) course, with presentations by peer medical students on current HIV statistics, recommendations for testing, and the importance of students' role in advocating for this concerning health issue. Due to limited return of surveys, we distributed surveys to 120 third year medical students in the spring of 2012 and 2013 during their Ambulatory Medicine month within the Internal Medicine curriculum. Limited Return of Surveys 25 surveys were returned during the 4 periods of collection from 2011 - 2013, out of a potential 520. Incorporation of students into the distribution of surveys restricted the number of physicians that responded. Despite attempts to personally involve students, inform them through peers of the importance of this issue, and integrate the survey in the AC course, students often will not complete a survey unless it is mandatory. It is also possible the students did not feel comfortable approaching their preceptor about HIV while the preceptor was grading the student and the survey may not have yielded honest results from the physician if the survey was done in the presence of the student. A future survey will yield greater results if the educational component of the study is removed. Provider Knowledge of Testing Guidelines CDC recommendations (Fig. 3A): 95.2% of providers surveyed stated that they were aware of the CDC guidelines; however, only 35% of these providers were implementing these recommendations. D.C. Department of Health (Fig. 3B): 68.4% of providers were aware of the D.C. DOH recommendations; however, of those, only 30.7% were implementing these guidelines. Fig. 3. Percentages of physicians are who responded as either “Aware and Implementing”, “Aware and Not Implementing” or “Not Aware.” (A) The CDC recommends that all patients ages 13-64 be tested for HIV in all healthcare settings after the patient is notified and consents (opt-out testing) and annually for high risk patients. (B) The D.C. DOH recommends that all patients ages 13-84 should be tested annually and all MSM should be tested every 6 months. Provider Testing Practices Fifty-eight percent of providers agreed that it is important to incorporate routine HIV screening in the medical care of their patients. Surprisingly, 21% (4 out of 25) disagree/strongly disagree that HIV testing is important to incorporate into routine screening. Only 4.8% of healthcare providers surveyed reported that they provided HIV tests to 90% or more of their patients, while 61.9% reported testing 25% of the time or less. The primary barriers to routine testing cited by providers included: 1) limited time to perform HIV counseling (23.8%) 2) HIV is not an issue for the physician's patient population (23.8%) 3) cost or reimbursement concerns (14.3%) While 24% specifically stated that there were no barriers. Fig. 1. Self-reported patient demographics. (A) Estimated percent of patient population of Caucasian, Hispanic/Latino, African American, Asian/Pacific Islander, Native American/Alaskan Native, Multiracial, or Other. (B) Estimated percent of patient population with Private Insurance, Medicare, Medicaid, or Self-pay. The study does not have enough power to make a statistically significant statement. By removing the educational arm of the study, we expect to have a greater response rate. There was an over-representation of private insurance use and Caucasian races as reported by those surveyed, as well as a lack of routine HIV testing which may correlate with provider bias. Further research will help elucidate false assumptions that physicians make based on their patient's race, geographic location, and insurance type. Poster produced by Faculty & Curriculum Support, Georgetown University School of Medicine We would like to thank Mary Beth Levin (GUSOM), Dr. Catherine Okuliar (GUH), Dr. Eileen Moore (GUH), Dr. Joesph Timpone (GUH), and Dr. Erica McClaskey (GUH). Provider Understanding of HIV/AIDS in D.C. Seventy-two percent of health care providers did not know the severity of the D.C. HIV/AIDS epidemic. Only 19% correctly stated that all four quadrants of the district met the UN threshold for a “generalized and severe” HIV epidemic. Provider & Patient Demographics Majority of respondents: Family Medicine (32%) Internal Medicine (20%) Pediatrics (20%) Patient Demographics: Race (Fig. 1A): On average, providers reported that their patient population primarily consisted of Caucasian (48%), Hispanic/Latinos (25%), and African American (19%). This is over-representative of the Caucasian population in D.C. Patient Demographics: Insurance (Fig. 1B): In terms of reimbursement, 59.6% were covered by private insurance, 14.1% were covered by Medicaid, 17.1% were covered by Medicare and 7.6% were self-pay. This is not a representative cross-section of D.C. insurance types, but rather an over- representation of private insurance. 4 out of 25 were specialists: 2 Hematology Oncology 1 Pulmonology 1 Adolescent Medicine Fig. 2. Responses to “Which DC quadrant(s) meet the UN criteria for 'generalized and severe' HIV epidemic?” (i.e. HIV prevalence above 1% of the population). Of the 14 who chose a quadrant (33% answered “Do not know”), 14 selected Southeast, 9 selected Southeast and Northeast, 8 selected Southeast, Northeast and Southwest, and 4 selected Southeast, Northeast, Southwest and Northwest. Physician Responses to “Which DC Quadrants Meet UN Criteria for HIV Epidemic?” Patient Demographics A B NW NE SW SE 8 4 9 14 BA