2. Stents
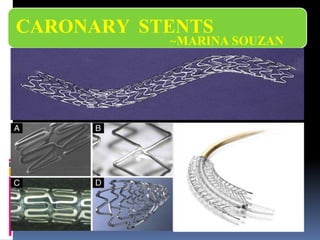
Stents are tiny, expandable tubes made of metal mesh
designed to open a blood vessel that is blocked by
plaque. Over time, the artery wall heals around the
stent.
5. TYPES OF STENTS
Metal composition
Open v/s closed cell designs
Thickness of struts
Eluting drugs
Stent design may be specific -small (<2.5 mm
diameter) vessels / bifurcation lesions
6. Metal composition
Stainless steel designs - greater radial
strength for aorto-ostial locations
Co-Cr - stronger & more radiopaque thinner
struts, lower profiles (<0.40”), better
flexibility & similar radial strength
7. Modular stents
Consist of several crown-shaped modules, which
may be manufactured from metal wires that are
punctually connected to form a tube
ie, based on repeating identically designed units,
again laser-cut, linked together by welded struts
An ‘open-cell’ design
Highly flexible
Offer better side-branch access
8. Provides local delivery of a drug
Methods for the storage and controlled
release
Nondegradable polymers- polyurethane,
silicone, polyorganophosphazene,
polymethacrylate, poly(ethylene
terephthalate), & phosphorylcholine
Biodegradable polymer- poly(l-lactide),
poly(3-hydroxybutyrate), polycaprolactone,
polyorthoester, fibrin
Stent Coating
9. Stent coating
The eluted drug is linked by a
degradable/permanent polymer coating only
a few micrometers in thickness
not expected to change mechanical strength may
affect surface friction
Cavities on the stent struts- drug depots
Small amounts of drugs applied directly to stent
surface
10.
11.
12.
13. Intended to support a vessel for time to
complete the healing process and to then
disappear after a specified time period
Complications resulting from long-term
intravascular presence of a FB-
thrombogenicity, permanent mechanical
irritation, prevention of positive remodeling,
are eliminated
Poly(L-lactic acid) (PLLA), poly(D-lactic acid)
(PDLA), poly(e-caprolactone) (PCL),
poly(glycolic acid) (PGA)
Biodegradeable stents
30. Absorb Stent (Abbot lab) :
Bioresorbable Vascular Scaffold (BVS) system that elutes
everolimus BioresorbableVascular
Scaffold (BVS) system
that elutes everolimus
in a similar way to
XIENCEV and then
resorbs naturally into
the body leaving no
permanent scaffold.
Vascular Reparative
Therapy (VRT).VRT is
designed to restore the
vessel to a more natural
state, making natural
vascular function
possible. working in three
phases to deliverVRT:
Revascularisation
Restoration
Resorption
http://www.ptca.org/news/2012/0928_ABBOTT_ABSORB.html
Stents are tiny, expandable tubes made of metal mesh designed to open a blood vessel that is blocked by plaque. Over time, the artery wall heals around the stent.
Sirolimus is rapamycin, a naturally occurring macrocyclic lactone discovered in the soil of Easter Island (Rapa Nui) in the 1960s. Rapamycin is a product of fermentation of Streptomyces hygroscopicusand was used as an antifungal antibiotic. Sirolimus blocks the cell cycle of proliferating cells binding to the high-affinity cytosolic receptor protein FK506, leading to the inhibition of mammalian target of rapamycin (mTOR), which prevents downregulation of tumor suppressive cell P27. The gene p27 inhibits cell-dependent kinase activity and blocks G1- to S-phase cell cycle progression. Sirolimus is lipophilic and easily crosses the cell membrane. The inhibition of mTOR suppresses T-cell proliferation and is a powerful antiproliferative and antimigratory agent acting on smooth muscle cells. Systemic sirolimus reduces neointimal proliferation after balloon injury in porcine coronary arteries. Local sirolimus administration inhibits neointimal proliferation.
Paclitaxel is a powerful antineoplastic drug found in the Pacific yew tree (Taxus brevifolia) and is used in the treatment of malignant ovarian and breast cancer. Paclitaxel stabilizes polymerized microtubules and enhances microtubular assembly, forming unorganized and decentralized microtubules in the cytoplasm. Cell replication is inhibited predominately in the G0/G1 and G2/M phase of the cell cycle. Paclitaxel is highly lipophilic, promoting rapid uptake through hydrophobic cell membranes and minimizing systemic loss. Paclitaxel is suitable for polymer-based delivery. It has long-lasting antiproliferative effects after a single administration and can be directly applied to metal as a durable simple coating.
Everolimus is a novel semisynthetic highly lipophilic macrolide with immunosuppressant and antiproliferative properties. The chemical name is 40-O-(2-hydroxyethyl)-rapamycin and it is created by modifying rapamycin. Similar to rapamycin, inhibiting mTOR is the likely mechanism for suppression of cell proliferation. At the cellular level, it blocks growth factor–driven transduction signals in the T-cell response to alloantigen and proliferation of both hematopoietic and non-hematopoietic cells. Following stimulation of the IL-2 receptor on the activated cell, it inhibits p70 S6 kinase, thereby arresting the cell cycle in the late G1 phase. Systemic everolimus suppresses in-stent neointimal growth in the rabbit iliac artery following stenting.
Zotarolimus is also a novel semisynthetic derivative of rapamycin, which was designed to have a shorter in vivo half-life. It is a highly lipophilic immunosuppressive and antiproliferative agent. As with rapamycin and everolimus, zotarolimus inhibits mTOR, blocks growth factor–driven cell proliferation, which ultimately results in cell cycle arrest in the G1 phase.
Bioresorbable Vascular Scaffold (BVS) system that elutes everolimus in a similar way to XIENCE V and then resorbs naturally into the body leaving no permanent scaffold.*
Vascular Reparative Therapy (VRT). VRT is designed to restore the vessel to a more natural state, making natural vascular function possible. While stenting performance is characterised by a single phase of revascularisation, Absorb was designed with the premise of working in three phases to deliver VRT:
Revascularisation
Restoration
Resorption
Mechanisms of Angioplasty andStenting
1.
Disruption of plaque and the arterial wall
The inflated balloon exerts pressure against the plaque and the arterial wall, causing fracturing and splitting. Concentric (round or circumferential) lesions fracture and split at the thinnest and weakest points. Eccentric lesions split at the junction of the plaque and the normal arterial wall. Dissection or separation of the plaque from the vessel wall releases the restraining effect caused by the lesion and results in a larger lumen. This is the major mechanism of balloon angioplasty.
2.
Loss of elastic recoil
Balloon dilatation causes stretching and thinning of the medial wall. Stretching causes the vessel wall to temporarily lose its elastic (recoil) properties. The degree of elastic recoil is affected by the balloon/artery size ratio. Almost all vessels have some elastic recoil. The major initial benefit of stenting is the elimination of elastic recoil, maintaining a large lumen over time.
3.
Redistribution and compression of plaque components
During angioplasty, balloon pressure causes denudation of the vessel wall lining (endothelial) cells and the extrusion or pushing out of plaque components. There may be some molding and extrusion longitudinally of the softer lipid material, but this effect accounts for a very small part of the overall effect.