
Recomendados
Recomendados
Mais conteúdo relacionado
Semelhante a pharmacokineticsclass.pptx
Semelhante a pharmacokineticsclass.pptx (20)
Último
Último (20)
pharmacokineticsclass.pptx
- 2. how the human body act on the drugs? Pharmacokinetics is the quantitative study of drug movement in, through and out of the body. Intensity of effect is related to concentration of the drug at the site of action, which depends on its pharmacokinetic properties Pharmacokinetic properties of particular drug is important to determine the route of administration, dose, onset of action, peak action time, duration of action and frequency of dosing 2
- 3. Dosage Regimen Concentration at the site of action Absorption Distribution Metabolism Concentration in Plasma Excretion Pharmacokinetics Pharmacodynamics Effect 3
- 4. 4
- 5. 5
- 6. 6
- 7. 7
- 8. Drug molecules can cross cell membrane by: Passive Diffusion Protein – mediated transport (carrier mediated) Facilitated Transport Active trnsport Primary Secondary 8
- 9. Most important Mechanism for most of the Drugs Majority of drugs diffuses across the membrane in the direction of concentration gradient No active role of the membrane Proportional to lipid : water partition coefficient Lipid soluble drugs diffuse by dissolving in the lipoidal matrix of the membrane Characteristics Not requiring energy Having no saturation Having no carriers Not resisting competitive inhibition 9
- 10. Affecting factors : • the size of molecule • Lipid solubility • Polarity • degree of ionization • the PH of the environment such as: fluid of body fluid in cell blood, urine 10
- 11. 11
- 12. Most of drugs are weak acids or weak bases. The ionization of drugs may markedly reduce their ability to permeate membranes. The degree of ionization of drugs is determined by the surrounding pH and their pKa. 12
- 13. pKa = negative logarithm of acid dissociation constant [A-] = ionized Drug [HA] = unionized drug 13
- 14. 14
- 15. Acidic drugs re absorbed are largely unionized in stomach and absorbed faster while basic drugs are absorbed faster in intestines Ion trapping Acidic drugs are excreted faster in alkaline urine – urinary alkalizers Basic drugs are excreted faster in acidic urine – urinary acidifiers 15
- 16. Passage of Drugs through aqueous pores in membrane or through Para cellular space Lipid insoluble drugs can cross – if the molecular size is small Majority of intestinal mucosa and RBCs have small pores and drugs cannot cross But, capillaries have large paracellular space and most drugs can filter through this 16
- 17. 17
- 18. Involve specific membrane transport proteins know as drug transporters or carriers – specific for the substrate Drug molecules bind to the transporter, translocated across the membrane, and then released on the on other side of the membrane. Specific, saturable and inhibitable Depending on Energy requirement - Can be either Facilitated (passive) or Active Transport 18
- 19. Move substrate of a single class (uniporters) down a concentration gradient No energy dependent Similar to entry of glucose into muscle (GLUT 4) 19
- 20. Active (concentrative) transporters can move solutes against a concentration gradient energy dependent Primary active transporters - generate energy themselves (e.g. ATP hydrolysis) Secondary transporters - utilize energy stored in voltage and ion gradients generated by a primary active transporter (e.g. Na+/K+-ATPase) Symporters (Co-transporters) Antiporters (Exchangers) 20
- 21. • ATP-Binding Cassette Transporters (ABC) Super family – Primary active transport • P-glycoprotein (P-gp encoded by MDR1) • • Intestinal mucosa, renal tubules and blood brain barrier etc. Mediate only efflux of solute from cytoplasm - detoxification Solute Carrier (SLC) transporters – Secondary active transport Organic anion transporting polypeptides (OATPs) Organic cation transporters (OCTs) Expressed in liver and renal tubules – metabolism and excretion of drugs 21
- 22. It involves the invagination of a part of the cell membrane and trapping within the cell of a small vesicle containing extra cellular constituents. The vesicle contents can than be released within the cell, or extruded from the other side of the cell. Pinocytosis is important for the transport of some macromolecules (e.g. insulin through BBB). 22
- 23. 1. ABSORPTION OF DRUGS Absorption is the transfer of a drug from its site of administration to the blood stream Most of drugs are absorbed by the way of passive transport Intravenous administration has no absorption Fraction of administered dose and rate of absorption are important 23
- 24. Drug properties: lipid solubility, molecular weight, and polarity etc Blood flow to the absorption site Total surface area available for absorption Contact time at the absorption surface Affinity with special tissue Routes of Administration (important): 24
- 25. Route of administration: Topical: Depends on lipid solubility – only lipid soluble drugs are penetrate intact skin – only few drugs are used therapeutically Examples – GTN, Hyoscine, Fentanyl, Nicotine, testosterone and estradiol Organophosphorous compounds – systemic toxicity Abraded skin: tannic acid – hepatic necrosis Cornea permeable to lipid soluble drugs Mucus membranes of mouth, rectum, vagina etc, are permeable to lipophillic drugs 25
- 26. Route of administration: Subcutaneous and Intramuscular: Drugs directly reach the vicinity of capillaries – passes capillary endothelium and reach circulation Passes through the large paracellular pores Faster and more predictable than oral absorption Exercise and heat – increase absorption Adrenaline – decrease absorption 26
- 27. Route of administration: Oral Route Physical properties – Physical state, lipid or water solubility Dosage forms: Particle size Disintegration time and Dissolution Rate Formulation – Biopharmaceutics Physiological factors: Ionization, pH effect Presence of Food Presence of Other agents 27
- 28. Before the drug reaches the systemic circulation, the drug can be metabolized in the liver or intestine. As a Result, the concentration of drug in the systemic circulation will be reduced. 28
- 30. Vena cava 30
- 31. Intravenous administration has no absorption phase According to the rate of absorption: Inhalation→Sublingual→Rectal→intramusc ular→subcutaneous→oral→transdermal Example – Nitroglycerine: IV effect – immediate, SL – 1 to 3 min and per rectal – 40 to 60 minute 31
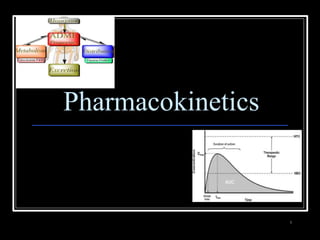
- 32. Bioavailability refers to the rate and extent of absorption of a drug from dosage form as determined by its concentration-time curve in blood or by its excretion in urine. It is a measure of the fraction (F) of administered dose of a drug that reaches the systemic circulation in the unchanged form Bioavailability of drug injected i.v. is 100%, but is frequently lower after oral ingestion, because: The drug may be incompletely absorbed The absorbed drug may undergo first pass metabolism in intestinal wall and/or liver or be excreted in bile. 32
- 33. BIOVAILABILITY - AUC Plasma concentration (mcg/ml) 0 5 Time (h) 1 0 1 5 AUC p.o. F = ------------ x 100% AUC i.v. AUC – area under the curve F – bioavailability 33
- 34. MTC MEC 34
- 35. 2. DISTRIBUTION OF DRUGS It is the passage of drug from the circulation to the tissue and site of its action. The extent of distribution of drug depends on its lipid solubility, ionization at physiological pH (dependent on pKa), extent of binding to plasma and tissue proteins and differences in regional blood flow, disease like CHF, uremia, cirrhosis Movement of drug - until equilibration between unbound drug in plasma and tissue fluids 35
- 36. Definition: Apparent Volume of distribution is defined as the volume that would accommodate all the drugs in the body, if the concentration was the same as in plasma Expressed as: in Liters V = Dose administered IV Plasma concentration 36
- 37. Total Body Fluid = 42 L (approx.) 37
- 38. Chloroquin – 13000 liters, Digoxin – 420 L, Morphine – 250 L and Propranolol – 280 L Streptomycin and Gentamicin – 18 L (WHY ?) `Vd` is an imaginary Volume of Fluid which will accommodate the entire quantity of the drug in the body, if the concentration throughout this imaginary volume were same as that in plasma 38
- 39. Lipid solubility (lipid : water partition coefficient) pKa of the drug Affinity for different tissues Blood flow – Brain Vs Fat Disease states Plasma protein Binding 39
- 40. Highly lipid soluble drugs – distribute to brain, heart and kidney etc. immediately followed by muscle and Fats 40
- 41. Blood brain barrier (BBB): includes the capillary endothelial cells (which have tight junctions and lack large intracellular pores) and an investment of glial tissue, over the capillaries. A similar barrier is loctated in the choroid plexus 41
- 42. BBB is a lipid layer and limits the entry of non-lipid soluble drugs (amikacin, gentamicin, neostigmine etc.). (Only lipid soluble unionized drugs penetrate and have action on the CNS) Efflux carriers like P-gp (glycoprotein) present in brain capillary endothelial cell (also in intestinal mucosal, renal tubular, hepatic canicular, placental and testicular cells) extrude drugs that enter brain by other processes. (Inflammation of meninges of the brain increases permeability of BBB) Dopamine (DA) does not enter brain, but its precursor levodopa does. This is used latter in parkinsonism. 42
- 43. Only lipid soluble drugs can penetrate – limitation of hydrophillic drugs Placental P-gp serves as limiting factor But, REMEMBER, its an incomplete barrier – some influx transporters operate Thalidomide 43
- 44. 44
- 45. Plasma protein binding (PPB): Most drugs possess physicochemical affinity for plasma proteins. Acidic drugs bind to plasma albumin and basic drugs to α1-glycoprotein Extent of binding depends on the individual compound. Increasing concentration of drug can progressively saturate the binding sites The clinical significant implications of PPB are: a) Highly PPB drugs are largely restricted to the vascular compartment and tend to have lower Vd. b) The PPB fraction is not available for action. c) There is an equilibration between PPB fraction of drug and free molecules of drug. 45
- 46. d) The drugs with high physicochemical affinity for plasma proteins (e.g. aspirin, sulfonamides, chloramphenicol) can replace the other drugs(e.g, warfarin) or endogenous compounds (bilirubin) with lower affinity. e) High degree of protein binding makes the drug long acting, because bound fraction is not available for metabolism, unless it is actively excreted by liver or kidney tubules. f) Generally expressed plasma concentrations of the drug refer to bound as well as free drug. g) In hypoalbuminemia, binding may be reduced and high concentration of free drug may be attained (e.g. phenytoin). 46
- 47. 47
- 48. Drugs may also accumulate in specific organs or get bound to specific tissue constituents, e.g.: Heart and skeletal muscles – digoxin (to muscle proteins) Liver – chloroquine, tetracyclines, digoxin Kidney – digoxin, chloroquine Thyroid gland – iodine Brain – chlorpromazine, isoniazid, acetazolamide Retina – chloroquine (to nucleoproteins) Iris – ephedrine, atropine (to melanin) Bones and teeth – tetracyclines, heavy metals (to mucopolysaccharide of connective tissue) Adipose tissues – thiopental, ether, minocycline, DDT 48
- 50. NON-POLAR LIPID SOLUBLE POLAR LIPID INSOLUBLE 50
- 51. 1. Active drug and its metabolite to inactive metabolites – most drugs (ibuprofen, paracetamol, chlormphenicol etc.) 2. Active drug to active product (phenacetin – acetminophen or paracetamol, morphine to Morphine-6- glucoronide, digitoxin to digoxin etc.) 3. Inactive drug to active/enhanced activity (prodrug) – levodopa - carbidopa, prednisone – prednisolone and enlpril – enlprilat) 4. No toxic or less toxic drug to toxic metabolites (Isoniazid to Acetyl isoniazid) 51
- 52. 2 (two) Phases of Biotransformation: •Phase I or Non-synthetic – metabolite may be active or inactive •Phase II or Synthetic – metabolites are inactive (Morphine – M-6 glucoronide is exception) 52
- 53. 53
- 54. Most important drug metabolizing reaction – addition of oxygen or (–ve) charged radical or removal of hydrogen or (+ve) charged radical Various oxidation reactions are – oxygenation or hydroxylation of C-, N- or S-atoms; N or 0- dealkylation Examples – Barbiturates, phenothiazines, paracetamol and steroids 54
- 55. • Involve – cytochrome P-450 monooxygenases (CYP), NADPH and Oxygen • More than 100 cytochrome P-450 isoenzymes are identified and grouped into more than 20 families – 1, 2 and 3 … • Sub-families are identified as A, B, and C etc. • In human - only 3 isoenzyme families important – CYP1, CYP2 and CYP3 • CYP 3A4/5 carry out biotransformation of largest number (30–50%) of drugs. In addition to liver, this isoforms are expressed in intestine (responsible for first pass metabolism at this site) and kidney too Inhibition of CYP 3A4 by erythromycin, clarithromycin, ketoconzole, itraconazole, verapamil, diltiazem and a constituent of grape fruit juice is responsible for unwanted interaction with terfenadine and astemizole • Rifampicin, phenytoin, carbmazepine, phenobarbital are inducers of the CYP 3A4 55
- 57. Some Drugs are oxidized by non- microsomal enzymes (mitochondrial and cytoplsmic) – Alcohol, Adrenaline, Mercaptopurine Alcohol – Dehydrogenase Adrenaline – MAO and COMT Mercaptopurine – Xanthine oxidase 57
- 58. This reaction is conversed of oxidation and involves CYP 450 enzymes working in the opposite direction. Examples - Chloramphenicol, levodopa, halothane and warfarin Levodopa (DOPA) Dopamine DOPA- decarboxylase 58
- 59. This is cleavage of drug molecule by taking up of a molecule of water. Similarly amides and polypeptides are hydrolyzed by amidase and peptidases. Hydrolysis occurs in liver, intestines, plasma and other tissues. Examples - Choline esters, procaine, lidocaine, pethidine, oxytocin Ester + H20 Acid + Alcohol Esterase 59
- 60. Cyclization: is formation of ring structure from a straight chain compound, e.g. proguanil. Decyclization: is opening up of ring structure of the cyclic molecule, e.g. phenytoin, barbiturates 60
- 61. Conjugation of the drug or its phase I metabolite with an endogenous substrate - polar highly ionized organic acid to be excreted in urine or bile - high energy requirements Glucoronide conjugation - most important synthetic reaction Compounds with hydroxyl or carboxylic acid group are easily conjugated with glucoronic acid - derived from glucose Examples: Chloramphenicol, aspirin, morphine, metroniazole, bilirubin, thyroxine Drug glucuronides, excreted in bile, can be hydrolyzed in the gut by bacteria, producing beta-glucoronidase - liberated drug is reabsorbed and undergoes the same fate - enterohepatic recirculation (e.g. chloramphenicol, phenolphthalein, oral contraceptives) and prolongs their action 61
- 62. 62
- 63. Acetylation: Compounds having amino or hydrazine residues are conjugated with the help of acetyl CoA, e.g.sulfonamides, isoniazid Genetic polymorphism (slow and fast acetylators) Sulfate conjugation: The phenolic compounds and steroids are sulfated by sulfokinases, e.g. chloramphenicol, adrenal and sex steroids 63
- 64. Methylation: The amines and phenols can be methylated. Methionine and cysteine act as methyl donors. Examples: adrenaline, histamine, nicotinic acid. Ribonucleoside/nucleotide synthesis: activation of many purine and pyrimidine antimetabolites used in cancer chemotherapy 64
- 65. Factors affecting biotransformation Concurrent use of drugs: Induction and inhibition Genetic polymorphism Pollutant exposure from environment or industry Pathological status Age 65
- 66. One drug can inhibit metabolism of other – if utilizes same enzyme However not common because different drugs are substrate of different CYPs A drug may inhibit one isoenzyme while being substrate of other isoenzyme – quinidine Some enzyme inhibitors – Omeprazole, metronidazole, isoniazide, ciprofloxacin and sulfonamides 66
- 67. CYP3A – antiepileptic agents - Phenobarbitone, Rifampicin and glucocorticoide CYP2E1 - isoniazid, acetone, chronic use of alcohol Other inducers – cigarette smoking, charcoal broiled meat, industrial pollutants – CYP1A Consequences of Induction: Decreased intensity – Failure of OCPs Increased intensity – Paracetamol poisoning (NABQI) Tolerance – Carbmazepine Some endogenous substrates are metabolized faster – steroids, bilirubin 67
- 68. 4. EXCRETION 68
- 69. Excretion is a transport procedure which the prototype drug (or parent drug) or other metabolic products are excreted through excretion organ or secretion organ Hydrophilic compounds can be easily excreted. Routes of drug excretion Kidney Biliary excretion Sweat and saliva Milk Pulmonary 69
- 70. Hepatic Excretion Drugs can be excreted in bile, especially when the are conjugated with – glucuronic Acid • Drug is absorbed glucuronidated or sulfatated in the liver and secreted through the bile glucuronic acid/sulfate is cleaved off by bacteria in GI tract drug is reabsorbed (steroid hormones, rifampicin, amoxycillin, contraceptives) • Anthraquinone, heavy metals – directly excreted in colon Portal vein BILE DUCT Intesti nes 70
- 71. RENAL EXCRETION Glomerular Filtration Tubular Reabsorption Tubular Secretion 71
- 72. Normal GFR – 120 ml/min Glomerular capillaries have pores larger than usual The kidney is responsible for excreting of all water soluble substances All nonprotein bound drugs (lipid soluble or insoluble) presented to the glomerulus are filtered Glomerular filtration of drugs depends on their plasma protein binding and renal blood flow - Protein bound drugs are not filtered ! Renal failure and aged persons 72
- 73. Back diffusion of Drugs (99%) – lipid soluble drugs Depends on pH of urine, ionization etc. Lipid insoluble ionized drugs excreted as it is – aminoglycoside (amikacin, gentamicin, tobramycin) Changes in urinary pH can change the excretion pattern of drugs Weak bases ionize more and are less reabsorbed in acidic urine. Weak acids ionized more and are less reabsorbed in alkaline urine Utilized clinically in salicylate and barbiturate poisoning – alkanized urine (Drugs with pKa: 5 – 8) Acidified urine – atropine and morphine etc. 73
- 74. Energy dependent active transport – reduces the free concentration of drugs – further, more drug dissociation from plasma binding – again more secretion (protein binding is facilitatory for excretion for some drugs) Bidirectional transport – Blood Vs tubular fluid Utilized clinically – penicillin Vs probenecid, probenecid Vs uric acid (salicylate) Quinidine decreases renal and biliary clearance of digoxin by inhibiting efflux carrier P-gp 74
- 75. Acidic urine alkaline drugs eliminated acid drugs reabsorbed Alkaline urine - acid drugs eliminated - alkaline drugs absorbed 75
- 76. 76
- 77. First Order Kinetics (exponential): Rate of elimination is directly proportional to drug concentration, CL remaining constant Constant fraction of drug is eliminated per unit time Zero Order kinetics (linear): The rate of elimination remains constant irrespective of drug concentration CL decreases with increase in concentration Alcohol, theophyline, tolbutmide etc. 77
- 78. Zero Order 1st Order conc. Time 78
- 79. CL = RoE/C V = dose IV/C 79
- 80. 1 half-life …………. 50% 2 half-lives………… 25% 3 half-lives …….…..12.5% 4 half-lives ………… 6.25% 50 + 25 + 12.5 + 6.25 = 93.75 93.75 + 3.125 + 1.56 = 98% after 5 HL 80
- 81. Repeated dosing: •When constant dose of a drug is repeated before the expiry of 4 half-life – peak concentration is achieved after certain interval •Balances between dose administered and dose interval 81
- 82. At steady state, elimination = input Cpss = dose rate/CL Dose Rate = target Cpss x CL In oral administration Dose rate = target Cpss x CL/F In zero order kinetics: follow Michaelis Menten kinetics RoE = (Vmax) (C) / Km + C Vmax = max. rate of drug elimination, Km = Plasma conc. In which elimination rate is half maximal CL = Roe/C 82
- 83. Low safety margin drugs (anticonvulsants, antidepressants, Lithium, Theophylline etc. – maintained at certain concentration within therapeutic range Drugs with short half-life (2-3 Hrs) – drugs are administered at conventional intervals (6-12 Hrs) – fluctuations are therapeutically acceptable Long acting drugs: Loading dose: Single dose or repeated dose in quick succession – to attain target conc. Quickly Loading dose = target Cp X V/F Maintenance dose: dose to be repeated at specific intervals 83
- 84. Useful in Narrow safety margin drugs – digoxin, anticonvulsants, antiarrhythmics and aminoglycosides etc Large individual variation – lithium and antidepressants Renal failure cases Poisoning cases Not useful in Response mesurable drugs – antihypertensives, diuretics etc Drugs activated in body – levodopa Hit and run drugs – Reseprpine, MAO inhibitors Irreversible action drugs – Orgnophosphorous compounds 84
- 85. Definition of Pharmacokinetics Transport of Drugs across Biological Membrane – different processes with example Factors affecting absorption of drugs Concept of Bioavailability Distribution of Drugs – Vd and its concept Biotransformation Mechanisms with examples Enzyme induction and inhibition concept and important examples Routes of excretion of drugs Orders of Kinetics Definition and concept of drug clearance Definition of half life and plateau principle 85
- 86. By prolonging absorption from the site of action – Oral and parenteral By increasing plasma protein binding By retarding rate of metabolism By retarding renal excretion 86
Notas do Editor
- Polar drugs are water soluble