Recomendados

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Accessibility of medical marijuana
Semelhante a Accessibility of medical marijuana (20)
Último
Último (20)
Accessibility of medical marijuana
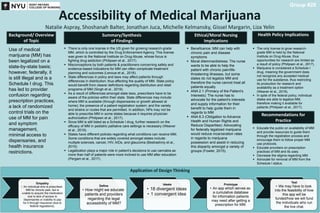
- 1. Application of Design Thinking Accessibility of Medical Marijuana Natalie Aspray, Shoshanah Balter, Jonathan Juca, Michelle Kelmansky, Gissel Margarin, Liza Yelin Summary/Synthesis of Findings Ethical/Moral Nursing Implications Health Policy ImplicationsBackground/ Overview of Topic Group #28 Recommendations for Practice Empathy • An individual who is prescribed MM for chronic pain, but is unable to acquire the medication due to lack of access to dispensaries or inability to pay for it through insurance (due to federal regulations). Define • How might we educate patients and providers regarding the legal accessibility of MM? Ideate • 18 divergent ideas • 1 convergent idea Prototype • An app which serves as a cumulative database for information patients may need after getting a prescription for MM. Test • We may have to look into the feasibility of how this app will be funded/how we will fund the individuals who run the live chat. Use of medical marijuana (MM) has been legalized on a state-by-state basis; however, federally, it is still illegal and is a Schedule I drug. This has led to provider confusion regarding prescription practices, a lack of randomized control trials on the use of MM for pain and symptom management, minimal access to dispensaries, and health insurance restrictions. There is only one license in the US given for growing research-grade MM, which is controlled by the Drug Enforcement Agency. This license was given to the National Institute on Drug Abuse, whose focus is fighting drug addiction (Philipsen et al., 2017). Misconceptions by both patients & practitioners concerning safety and evidence-based indications for MM can often complicate treatment planning and outcomes (Lenoue et al., 2016). State differences in policy and laws may affect patients through differences in distribution; thus affecting the quality of MM. State policy would benefit from clearer definitions regarding distribution and retail programs of MM (Singh et al., 2019). As a result of differences amongst state laws, prescribers have to be aware of the policies within their state. State differences may include: where MM is available (through dispensaries or growth allowed at home); the presence of a patient registration system; and the variety and strains or routes that are permitted. In addition, NPs may not be able to prescribe MM in some states because it requires physician authorization (Philipsen et al., 2017). Since MM is still listed as a Schedule I drug, further research on the efficacy of MM in pediatric palliative care settings is necessary (Weaver et al., 2019). States have different policies regarding what conditions can receive MM. Some conditions that are widely covered amongst states include: multiple sclerosis, cancer, HIV, AIDs, and glaucoma (Bestrashniy et al., 2015). Legalization plays a major role in patient’s decisions to use cannabis as more than half of patients were more inclined to use MM after education (Pergam et al., 2017). Beneficence: MM can help with chronic pain and disease symptoms Moral dilemma/distress: The nurse wants to be able to help the patient with chronic pain/life- threatening illnesses, but some states do not legalize MM and therefore the nurse cannot treat all patients equally ANA 2.1 (Primacy of the Patient’s Interests): The nurse has to advocate for the patient's interests and supply information for their benefit to help guide them in regards to MM ANA 8.3 (Obligation to Advance Health and Human Rights and Reduce Disparities): Advocating for federally legalized marijuana would reduce incarceration rates in regards to marijuana possession and assist in reducing this disparity amongst a variety of groups (Fowler, 2015). The only license to grow research- grade MM is held by the National Institute on Drug Abuse, thus opportunities for research are limited as a result of policy (Philipsen et al., 2017). Marijuana is considered a Schedule I drug, meaning the government does not recognize any accepted medical use for the substance, thus restricting its production for research and availability as a treatment option (Weaver et al., 2019). In spite of the federal policy, individual states are able to legalize MM, therefore making it available for patients (Philipsen et al., 2017). Educate the public on availability of MM and provide resources to guide them through the registration process and encourage them to follow proper MM use protocols. Educate providers on prescription practices of MM and its uses. Decrease the stigma regarding MM. Advocate for removal of MM from the Schedule I status.