Nursing management in cancer care
•Transferir como PPTX, PDF•
8 gostaram•10,069 visualizações

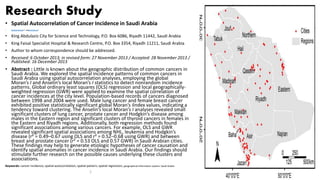
The document analyzes the spatial patterns of common cancers in Saudi Arabia using spatial autocorrelation statistics to detect nonrandom incidence patterns. It finds that lung cancer in males and breast cancer in females exhibited statistically significant clustering in certain regions. Both global and local regression models also revealed significant spatial associations between certain cancer types in Saudi Arabian cities.

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Nursing management in cancer care
Semelhante a Nursing management in cancer care (20)
Mais de Jamilah AlQahtani
Mais de Jamilah AlQahtani (20)
Último
Último (20)
Nursing management in cancer care
- 1. Research Study • Spatial Autocorrelation of Cancer Incidence in Saudi Arabia • Khalid Al-Ahmadi1,* andAli Al-Zahrani2 • King Abdulaziz City for Science and Technology, P.O. Box 6086, Riyadh 11442, Saudi Arabia • King Faisal Specialist Hospital & Research Centre, P.O. Box 3354, Riyadh 11211, Saudi Arabia • Author to whom correspondence should be addressed. • Received: 6 October 2013; in revised form: 27 November 2013 / Accepted: 28 November 2013 / Published: 16 December 2013 • Abstract : Little is known about the geographic distribution of common cancers in Saudi Arabia. We explored the spatial incidence patterns of common cancers in Saudi Arabia using spatial autocorrelation analyses, employing the global Moran’s I and Anselin’s local Moran’s I statistics to detect nonrandom incidence patterns. Global ordinary least squares (OLS) regression and local geographically- weighted regression (GWR) were applied to examine the spatial correlation of cancer incidences at the city level. Population-based records of cancers diagnosed between 1998 and 2004 were used. Male lung cancer and female breast cancer exhibited positive statistically significant global Moran’s Iindex values, indicating a tendency toward clustering. The Anselin’s local Moran’s I analyses revealed small significant clusters of lung cancer, prostate cancer and Hodgkin’s disease among males in the Eastern region and significant clusters of thyroid cancers in females in the Eastern and Riyadh regions. Additionally, both regression methods found significant associations among various cancers. For example, OLS and GWR revealed significant spatial associations among NHL, leukemia and Hodgkin’s disease (r² = 0.49–0.67 using OLS and r² = 0.52–0.68 using GWR) and between breast and prostate cancer (r² = 0.53 OLS and 0.57 GWR) in Saudi Arabian cities. These findings may help to generate etiologic hypotheses of cancer causation and identify spatial anomalies in cancer incidence in Saudi Arabia. Our findings should stimulate further research on the possible causes underlying these clusters and associations. Keywords: cancer incidence; spatial autocorrelation; spatial pattern; spatial regression; geographical information system; Saudi Arabia 1
- 2. 2
- 3. Nursing Management in Cancer Care 3
- 4. Contents • Types of neoplasms and related pathophysiology • Diagnosis procedures • Modalities of treatment and nurse’s role • Special therapies, chemotherapy and radiotherapy • Prevent measures and other therapy 4
- 5. Learning objectives • At the end of this lecture the student will be able to: • Define cancer • Identify the etiology /pathophysiology of cancer • Describe the predispose factors of cancer • Identify the metastasis • Describe clinical manifestation / assessment of cancer • Identify diagnostic test of cancer • Identify the management of cancer ‘’modalities of treatment and nurse’s role’’ • Special therapy, chemotherapy and radiotherapy • Discuses the nursing management of cancer 5
- 6. Cancer Overview • Cancer, also called malignancy, is an abnormal growth of cells. • There are more than 100 to 200 types of cancer, including breast cancer, skin cancer, lung cancer, colon cancer, prostate cancer, and lymphoma. Symptoms vary depending on the type. • Cancer treatment may include chemotherapy, radiation, and/or surgery. 6
- 7. Cancer starts when cells change abnormally • Cancer is when abnormal cells divide in an uncontrolled way. Some cancers may eventually spread into other tissues • Cancer starts when gene changes make one cell or a few cells begin to grow and multiply too much. This may cause a growth called a tumour. Cancer grows as cells multiply over and over 7
- 8. Some cancers can spread to other parts of the body • A primary tumour is the name for where a cancer starts. • Cancer can sometimes spread to other parts of the body – this is called a secondary tumour or a metastasis. • Cancer and its treatments can affect body systems, such as the blood circulation, lymphatic and immune systems, and the hormone system. 8
- 9. Is cancer genetic? • Most cancers start due to gene changes that happen over a person’s lifetime. • More rarely cancers start due to inherited faulty genes passed down in families. 9
- 10. Cancer can sometimes come back • Many cancers are cured. But in some people cancer can return. • Some cancers can’t be cured but treatment is often able to control them for some years. 10
- 11. There are 5 main cancer groups Cancers are divided into groups according to the type of cell they start from. They include 1) Carcinomas 2) Lymphomas 3) Leukaemias 4) Brain tumours 5) Sarcomas 11
- 12. 12
- 13. Stages and grading of cancer • Staging and grading give an idea of how quickly a cancer may grow and which treatments may work best • The stage of a cancer means how big it is and whether it has spread. • Grading looks at how abnormal the cancer cells are. 13
- 14. Cancer stages Different types of staging systems are used for different types of cancer. Below is an example of one common method of staging: stage 0 – indicates that the cancer is where it started (in situ) and hasn't spread stage I – the cancer is small and hasn't spread anywhere else stage II – the cancer has grown, but hasn't spread stage III – the cancer is larger and may have spread to the surrounding tissues and/or the lymph nodes (part of the lymphatic system) stage IV – the cancer has spread from where it started to at least one other body organ; also known as "secondary" or "metastatic" cancer 14
- 15. Cancer grades The grade of a cancer depends on what the cells look like under a microscope. In general, a lower grade indicates a slower-growing cancer and a higher grade indicates a faster-growing one. The grading system that's usually used is as follows: grade I – cancer cells that resemble normal cells and aren't growing rapidly grade II – cancer cells that don't look like normal cells and are growing faster than normal cells grade III – cancer cells that look abnormal and may grow or spread more aggressively 15
- 16. A neoplasm • is an abnormal growth of cells in the body, also described as a tumor. • Neoplasm comes to us from 'neo-', which means 'new' and '-plasm', which means 'cell' or 'tissue substance • A neoplasm can be a small growth, such as a mole, or a cancerous or pre-cancerous tumor. • Most of the time, neoplasms are not dangerous to own health, 16
- 17. Recognizing a Neoplasm • A visible neoplasm may look exactly like skin, or it may be a different color or texture. • They are usually painless, but they can hurt or bleed—a main point that differentiates them from warts. • Neoplasms may grow very slowly, and it is rare for a neoplasm to grow rapidly. • It may be notice as small growths on the surface of the skin, or inside reachable areas of own body, such as ear canals or nostrils. • Neoplasms can also grow inside the body, where can’t be seen them. In some instances, internal neoplasms may cause noticeable bumps, but they are usually located deep beneath the surface of the skin, where they wouldn't cause a change that could be seen from the outside. 17
- 18. Types of Neoplasm In the human body, there are trillions of normal, healthy cells. These cells grow, divide, multiply, die, and are replaced in a controlled, paced manner. However, in the case of a neoplasm, the cells may grow more rapidly or survive for longer than they are supposed to. Tumors can be cancerous, but they aren't always 18
- 19. Types of Neoplasms: can be benign growths, pre-cancerous tumors, or cancer. 1. A benign neoplasm is a growth that does not have cellular features of cancer or pre-cancer and is, thus, highly unlikely to become dangerous. 2. A pre-cancerous tumor has features of a malignant tumor, but has not yet become cancer, and has not spread. 3. Cancer is a neoplasm that can grow rapidly, spread, and cause damage to the body. A malignant neoplasm is cancerous, while a metastatic neoplasm is malignant cancer that has spread to nearby or distant areas of the body. 19
- 20. Benign Neoplasms • Benign neoplasms are often called birthmarks, and they may develop during late childhood or in adulthood. • Benign tumors usually grow slowly, if at all, and they are generally not life- threatening. • These are caused by a limited overgrowth of cells, usually without a known cause. 20
- 21. Examples of benign neoplasm include: • Skin moles • Skin tags (acrochordons) • Cysts in sebaceous glands (sweat glands) • Breast cysts that usually develop during pregnancy • Encapsulated skin growth, often triggered by an insect bite or infection • Raised scar tissue (keloids) • Uterine fibroids • The fact that benign tumors are not cancer doesn't mean that they can't cause problems. • Fibroids, for example, can cause significant bleeding and pain that may require their removal. 21
- 22. Malignant Neoplasms • A metastatic neoplasm is defined as cancer. It is most often associated with damage to a cell's DNA. This damage results in genetic mutations that cause abnormal cells to lose their normal function, multiply faster, live longer, and invade other cells and tissue. • Certain factors can trigger these mutations, including genetics, sun exposure, and toxic substances. Smoking, for instance, can increase a person's risk of lung cancer, while excessive alcohol use may lead to liver cancer. 22
- 23. Malignant NeoplasmsCONT’S • A malignant neoplasm can grow in any part of the body and can metastasize (spread) to virtually any part of the body as well. A malignant neoplasm may begin as a physical mass, such as a tumor in the breast, or it can begin as an overproduction of a cell type, such as leukemia—a form of cancer characterized by overproduction of blood cells. • Pre-cancerous neoplasms are growths that have not spread and show the potential to become cancer. This is usually diagnosed based on a microscopic examination of the neoplasm. 23
- 24. CANCER FACTS • actually cancer cells, do not invade the body like an infection but rather arise from normal cells that are changed ‘transformed’ by contact with carcinogen (substance that damages cellular DNA and alters cell growth). 24
- 25. Normal And Cancer Cells Structure 25
- 26. Cancer Processes • cancer cells, to become transformed, a cell must go through a serious of processes consisting of: • Initiation • Promotion • Progression • Metastasis 26
- 27. Metastasis: • In metastasis, cancer cells break away from where they first formed (primary cancer), travel through the blood or lymph system, and form new tumors (metastatic tumors) in other parts of the body. The metastatic tumor is the same type of cancer as the primary tumor. 27
- 28. Metastasis 28
- 29. 29
- 30. Site of Metastasis for common tumors Primary secondary Lung cancer Lymph node, brain, bone, liver, pancreas Colorectal cancer Adjacent lymph nodes, liver Breast cancer Bone, brain, lung, liver Leukemia Visceral organs, brain 30
- 31. Risk Factors Of Cancer Development • Environmental exposure to carcinogens • Genetic heritage • Age • Alcohol • Diet • Hormones • Immunosuppression • Infectious Agents • Obesity • Radiation • Sunlight • Tobacco 31
- 32. Stages and grading of cancer 32
- 33. Cancer stages Different types of staging systems are used for different types of cancer. Below is an example of one common method of staging: stage 0 – indicates that the cancer is where it started (in situ) and hasn't spread stage I – the cancer is small and hasn't spread anywhere else stage II – the cancer has grown, but hasn't spread stage III – the cancer is larger and may have spread to the surrounding tissues and/or the lymph nodes (part of the lymphatic system) stage IV – the cancer has spread from where it started to at least one other body organ; also known as "secondary" or "metastatic" cancer 33
- 34. Cancer grades The grade of a cancer depends on what the cells look like under a microscope. In general, a lower grade indicates a slower-growing cancer and a higher grade indicates a faster-growing one. The grading system that's usually used is as follows: grade I – cancer cells that resemble normal cells and aren't growing rapidly grade II – cancer cells that don't look like normal cells and are growing faster than normal cells grade III – cancer cells that look abnormal and may grow or spread more aggressively 34
- 36. Diagnostic Tests • History & Physical Exam • ( depend on clinical manifestations, index of suspicion for a particular cancer) • Lab Tests • Screening chemistry tests e,g, electrolytes (sodium, potassium, calcium), renal test BUN, creatinine, liver test (bilirubin, AST, Alkaline Phosphate, LDH), bone test (calcium ) depend on individual condition risk factors. • CBC with differential and platelets. May reveal anemia, changes in RBCs and WBC increased or decreased • Tumor Markers: For baseline and observation — to assess tumor burden and monitor levels of tumor and indicate a recurrence; prognosis (what treatment to use if the tumor should recur); most tumor markers are NOT specific, meaning that positive result does not necessarily mean that the primary site can be readily identified. 36
- 37. Diagnostic Tests cont’ • Imaging • Chest x-ray screens for primary or metastatic disease of lung 37
- 38. Diagnostic Tests cont’ • Endoscopy (used for direct visualization of body organs/cativies to detect abnormalities) • Scans (e.g. MRI,CT Gallium) and ultrasound: may be done for diagnostic purposes, identification of metastasis and evaluation of response to treatment. 68 Ga-DOTATOC-PET/MRI (A – C) and PET/CT (D– F) of patient 11. Extensive and inhomogeneous meningioma of the skull base infiltrating the nasal cavity. DOTATOC-PET can distinguish between vital meningioma and other tissues such as postoperative scarring or reactive tissue. (A) contrast-enhanced T1-weighted MRI. (B) DOTATOC-PET 30 minutes p.i. (derived from the PET/CT). (C) fusion of a and b. (D) native CT. (E) DOTATOC-PET 2 hours p.i. (derived from the PET/MRI). (F) fusion of D and E.38
- 39. Diagnostic Tests • Biopsy (fine needle aspiration FNA, needle core, incisional, excisional) done to differentiate and delineate treatment and may be taken from bone marrow, skin, organ. 39
- 40. Carcinogens • Many environmental have been identified as causative of human cancer including: • Physical carcinogens : radiation • Chemical carcinogens (including those from biological sources) • Viral carcinogens viruses • Diet and cancer development 40
- 41. Diet And Cancer Development Foods and drinks to limit in diet or have less of include: 1. fatty red meats and processed meats 2. highly processed foods that are low in fiber 3. heavily salted and pickled foods 4. alcohol. Foods to ‘eat more’ 1. The strongest protective anti-cancer effect has been shown with: 2. vegetables, especially raw vegetables or salads, such as leafy green vegetables and carrots 3. foods high in dietary fibre, such as grains and cereals 4. tomatoes 5. citrus fruits 6. cruciferous vegetables like broccoli, cabbage, Brussels sprouts, bok choy and other Asian greens. 7. Include more of these vegetables and fruits in your diet, along with other varieties. 41
- 42. Treatment • Treatment depends on: • Type of cancer • Location • Extent of cancer • Stage at which has been diagnosed • Health and well being of patient 42
- 43. Oncological treatment modalities 1-Chemotherapy Is one modality of treatment for both cancerous and non-cancerous conditions. Currently, chemotherapeutic agents are being utilized in the treatment of: 1) Cancer 2) HIV/AIDS 3) Sickle cell anemia(SCA) 4) Systemic lupus Erythematosus (SLE) 5) Rheumatoid Arthritis 6) Multiple sclerosis (MS) 43
- 44. Oncological treatment modalities cont’ • Goal of chemotherapy are: 1. Curative treatment are aimed at total elimination of cancerous cells, including those may spread to other parts of the body. 2. Adjuvant chemotherapy is used in addition to surgery and/ or radiation to eliminate systemic microscopic cancerous cells. The purpose of adjuvant therapy is to provide a complete cure or remission. 3. The intent of palliative chemotherapy is to reduce tumor size, extend life and improve the overall quality of life. 44
- 45. Oncological treatment modalities cont’ • Chemotherapy agent can be classified in one of two way: 1. The effect the agent has on the cell 2. The pharmacologic properties of the agent 45
- 46. 2- Radiation Therapy • Is the use of high-energy x-ray to treat cancer. • Radiation oncology is a subspecialty that incorporates the science and clinical application of therapeutic radiation in cancer therapy. 46
- 47. Goals of Radiation Therapy • Treatment of cancer with ionizing radiation • Radiation destroys cells in the area being treated • Making it impossible for these cells to continue to grow. 47
- 48. Indications for radiation therapy • Cure: primary treatment for early stage of Hodgkin's disease, cervical carcinoma. • Control: to control the growth or spread of tumors mass. Generally not a cure but may curative and/or to allow less allow less radical surgery • Neo-adjuvant: to ‘’downstage’’ bulky tumors, such as large breast or rectal tumors. Intent may be curative and /or to allow less radical surgery • Adjuvant: to reduce the risk of local recurrence at the site of tumor such as breast radiation after lumpectomy, or to treat sanctuary sites such as the brain after definitive therapy for acute lymphocytic leukemia or small cell lung cancer . • Palliation: pain control for sites of bony metastasis, control of bulky metastasis to reduce morbidity such as massive lymphadenopathy. • Oncologic emergencies: spinal cord compression and superior vena cava syndrome (selected cases). 48
- 49. •Fatigue during radiation is subjective, almost universal, and multifactorial (concurrent chemotherapy, weight loss, pain, anemia and length of radiation treatment). 49
- 50. Treatment Cont,s • 3- surgery • Removal of the tumor, surrounding tissue and lymph nodes. • Be conventional instruments or laser. • 4- hormonal therapy • Use of hormones to change the way hormones in the body help cancer to grow. • Biological therapy • Immunotherapy- makes use of the body’s immune system. 50
- 51. Alternative Therapies •The view point on Alternative therapies for cancer range from an enthusiastic acceptance of complementary therapies to the belief that they are all ‘’quack medicine’’ 51
- 52. Death and dying Dying is the process of moving into the state of death. Dying still has movement, death is static Patricia weenolsen in ‘’the art of dying’’ Ability to support and to meet the needs of dying clients and their support systems is affected by a multitude of factors. • These factors include: 1. The initial stage of the time of diagnosis 2. Post and present treatments 3. Whether the client’s experiencing a recurrence or progression of he disease 4. The client’s relationship with the health care provider 5. The health care provider experience and comfort level with death and dying issues 6. The client’s family/support system or lack thereof 7. The symptoms he/she is experiencing 8. His/her own fears and concerns about death. 52
- 53. Physiological Changes Towards The End Of Life • Decrease urine output, resulting in the need for the urinal, bedpan, commode, and /or characterization. • Decreased GI fluid, resulting in decreased episodes of vomiting, need for NGT. • Decreased pulmonary secretions, resulting in decreased cough, coughing, chocking and suctioning • Decreased pharyngeal secretions for those too weak to swallow, less likely to feel like drowning. 53
- 54. • Decrease fluid overload resulting in decreased peripheral and pulmonary edema • Reabsorption of fluid, resulting in decreased ascites decreased peritumor edema with decreased pain. • Decreased wound and fistula drainage • Decreased intracranial pressure in some patients resulting in increased lucidity. • Decreased care, cost and burden of maintain hydration. Physiological Changes Towards The End Of Life 54
- 55. Nursing care plan • Nursing priorities 1. Support adaptation and independence 2. Promote comfort 3. Maintain optimal physical functioning 4. Prevent complications 5. Provide information about disease process/ condition, prognosis and treatment needs 55
- 56. Nursing care plan • Discharge goals Patient is dealing with current situation realistically Pain alleviated/controlled Homeostasis achieved Complications prevented/minimized Disease process/condition, prognosis and therapeutic choices and regimen understood. Plan in place to meet needs after discharge. 56
- 57. Nursing Diagnosis • Risk for impaired skin integrity • Fear/ anxiety • Risk for infection • Risk for altered family process • Risk for fluid volume deficit • Risk for constipation/diarrhea • Altered nutrition: less than body requirements • Acute pain 57
- 58. Nursing diagnosis 1. anticipatory grieving Related to : Anticipated loss of physical well being (e,g, loss of body part: change in body function) change in lifestyle Perceived potential death of patient Evidence by : Changes in eating habits, alterations in sleep ptterns, activity levels, libido and commination patterns. Denial of potential loss choked feedings, anger. 58
- 59. Desired Outcomes • Identify and express feelings appropriately. • Continue normal life activities, looking toward/planning for the future, one day at a time. • Verbalize understanding of the dying process and feelings of being supported in grief work. 59
- 60. Nursing Interventions Rationale Expect initial shock and disbelief following diagnosis of cancer and traumatizing procedures (disfiguring surgery, colostomy, amputation). Few patients are fully prepared for the reality of the changes that can occur. Assess patient and SO for stage of grief currently being experienced. Explain process as appropriate. Knowledge about the grieving process reinforces the normality of feelings and reactions being experienced and can help patient deal more effectively with them. Provide open, nonjudgmental environment. Use therapeutic communication skills of Active-Listening, acknowledgment, and so on. Promotes and encourages realistic dialogue about feelings and concerns. Encourage verbalization of thoughts or concerns and accept expressions of sadness, anger, rejection. Acknowledge normality of these feelings. Patient may feel supported in expression of feelings by the understanding that deep and often conflicting emotions are normal and experienced by others in this difficult situation. Be aware of mood swings, hostility, and other acting-out behavior. Set limits on inappropriate behavior, redirect negative thinking. Indicators of ineffective coping and need for additional interventions. Preventing destructive actions enables patient to maintain control and sense of self-esteem. Be aware of debilitating depression. Ask patient direct questions about state of mind. Studies show that many cancer patients are at high risk for suicide. They are especially vulnerable when recently diagnosed and discharged from hospital. Visit frequently and provide physical contact as appropriate, or provide frequent phone support as appropriate for setting. Arrange for care provider and support person to stay with patient as needed. Helps reduce feelings of isolation and abandonment. 60
- 61. Nursing Interventions Rationale Reinforce teaching regarding disease process and treatments and provide information as appropriate about dying. Be honest; do not give false hope while providing emotional support. Patient and SO benefit from factual information. Individuals may ask direct questions about death, and honest answers promote trust and provide reassurance that correct information will be given. Review past life experiences, role changes, and coping skills. Talk about things that interest the patient. Opportunity to identify skills that may help individuals cope with grief of current situation more effectively. Note evidence of conflict; expressions of anger; and statements of despair, guilt, hopelessness, “nothing to live for.” Interpersonal conflicts or angry behavior may be patient’s way of expressing and dealing with feelings of despair or spiritual distress and could be indicative of suicidal ideation. Determine way that patient and SO understand and respond to death such as cultural expectations, learned behaviors, experience with death (close family members, friends), beliefs about life after death, faith in Higher Power (God). These factors affect how each individual deals with the possibility of death and influences how they may respond and interact. Identify positive aspects of the situation. Possibility of remission and slow progression of disease and new therapies can offer hope for the future. Discuss ways patient and SO can plan together for the future. Encourage setting of realistic goals. Having a part in problem solving and planning can provide a sense of control over anticipated events. Refer to visiting nurse, home health agency as needed, or hospice program, if appropriate. Provides support in meeting physical and emotional needs of patient and SO, and can supplement the care family and friends are able to give.61
- 62. • Situational Low Self-Esteem: Development of a negative perception of self-worth in response to current situation. • May be related to • Biophysical: disfiguring surgery, chemotherapy or radiotherapy side effects, e.g., loss of hair, nausea/vomiting, weight loss, anorexia, impotence, sterility, overwhelming fatigue, uncontrolled pain • Psychosocial: threat of death; feelings of lack of control and doubt regarding acceptance by others; fear and anxiety • Possibly evidenced by • Verbalization of change in lifestyle; fear of rejection/reaction of others; negative feelings about body; feelings of helplessness, hopelessness, powerlessness • Preoccupation with change or loss • Not taking responsibility for self-care, lack of follow-through • Change in self-perception/other’s perception of role 62
- 63. Desired Outcomes • Verbalize understanding of body changes, acceptance of self in situation. • Begin to develop coping mechanisms to deal effectively with problems. • Demonstrate adaptation to changes/events that have occurred as evidenced by setting of realistic goals and active participation in work/play/personal relationships as appropriate. 63
- 64. Nursing Interventions Rationale Discuss with patient and SO how the diagnosis and treatment are affecting the patient’s personal life, home and work activities. Aids in defining concerns to begin problem-solving process. Review anticipated side effects associated with a particular treatment, including possible effects on sexual activity and sense of attractiveness and desirability (alopecia, disfiguring surgery). Tell patient that not all side effects occur, and others may be minimized or controlled. Anticipatory guidance can help patient and SO begin the process of adaptation to new state and to prepare for some side effects (buy a wig before radiation, schedule time off from work as indicated). Encourage discussion of concerns about effects of cancer and treatments on role as homemaker, wage earner, parent, and so forth. May help reduce problems that interfere with acceptance of treatment or stimulate progression of disease. Acknowledge difficulties patient may be experiencing. Give information that counseling is often necessary and important in the adaptation process. Validates reality of patient’s feelings and gives permission to take whatever measures are necessary to cope with what is happening. 64
- 65. Nursing Interventions Rationale Evaluate support structures available to and used by patient and SO. Helps with planning for care while hospitalized and after discharge. Provide emotional support for patient and SO during diagnostic tests and treatment phase. Although some patients adapt or adjust to cancer effects or side effects of therapy, many need additional support during this period. Use touch during interactions, if acceptable to patient, and maintain eye contact. Affirmation of individuality and acceptance is important in reducing patient’s feelings of insecurity and self-doubt. Refer for professional counseling as indicated. May be necessary to regain and maintain a positive psychosocial structure if patient and SO support systems are deteriorating. 65
- 66. Conclusion • Metastasis occurs when cancer cells move from the primary site to move remote sites by breaking off from the original tumor. • Fatigue during radiation is subjective almost universal and multifactorial • Decreased urine output, resulting in the need for the the urinal, bedpan, commode and characterization. 66
- 67. References • Smelter S.C.,Bare B.G.,(Brunner and suddarths Medical-surgical Nursing ,.lippencot • Lewis S.W., Heitkemper M.M., Dirkson S.R., Medical Surgical Nursing Assessment And Management of clinical problems • Philadelphia, PA. Lippincott, Williams & Wilkins. 2003(Nurse's 3- Minute Clinical Reference) 67
Notas do Editor
- Sarcoma is a tumor that affects connective tissue. Soft tissue sarcomas, as the name suggests, affect the soft tissues; these include fat, muscle, blood vessels, deep skin tissues, cartilage, tendons, and ligaments. Sarcomas are a relatively rare type of cancer.
- Different & Similar Meanings What's the difference between an apartment and a condo? Depending on how you look at things your answer could be: 'nothing'. And, you'd be right. But if you were to look at the question from a slightly different angle, you could say quite simply that an apartment is rented out and a condo is bought. You'd be right again! So there is a similar dilemma between a tumor and a neoplasm. Depending on how you look at it, these two terms could mean the same thing or they may not. This lesson explains. What Is A Tumor? First, let's begin by defining tumor. Way back when, the word tumor technically referred to any swelling or abnormal enlargement in or on the human body. That's because 'tumor' means a swelling or swollen state in Latin. Tumor, or swelling, is also one of the cardinal signs of inflammation alongside rubor (redness), dolor (pain), calor (heat), and fanctio laesa (loss of function). Thus, 'tumor' can classically refer to any swellings or swollen states of the human body (this list is by no means complete): The swelling associated with inflammation. For example, when your knee swells up after you injure it playing basketball or another sport. An abscess, an accumulation of pus as a result of an infection. A cyst, an enclosed sac-like structure filled with a liquid or semisolid substance. A lump or bump associated with cancer. Again, those were all example of tumors in the proper Latin sense of things. You would be correct in calling all of those examples tumors but most people today think of tumors in a different light. What Is A Neoplasm? Nowadays, the word 'tumor' is more frequently associated with a neoplasm. A neoplasm is some sort of abnormal new growth of tissue, a lump or bump, that can be benign or malignant. Neoplasm comes to us from 'neo-', which means 'new' and '-plasm', which means 'cell' or 'tissue substance'. Again, a neoplasm can be: Malignant - in other words cancerous. The tumor invades the surrounding tissues and/or spreads around the body in a process called metastasis. Benign - not cancerous. The tumor doesn't spread around the body nor does it invade the surrounding tissues. However, a benign tumor can damage the body in plenty of ways, such as by obstructing an organ or crushing it. In other words, a benign tumor isn't necessarily harmless. There is no such thing as 'benign cancer' since 'benign' and 'cancer' are referring to completely different things. To unlock this lesson you must be a Study.com Member. Create your account Register to view this lesson Are you a student or a teacher? I am a student I am a teacher Try it risk-free for 30 days You are viewing lesson 4 in chapter 14 of the course: Introduction to Pharmacology29 chapters | 250 lessons Ch 1. History & Types of... Ch 2. Basics of Pharmacology Ch 3. Formulas & Calculations for... Ch 4. Dosage Analysis in... Ch 5. Pharmacology &... Ch 6. Respiratory Medications Ch 7. Endocrine System... Ch 8. Therapeutic Responses in... Ch 9. Stimulants &... Ch 10. Medicinal Herbology Ch 11. Alternative Medicine &... Ch 12. Alternative Medicine for Digestive... Ch 13. Reproductive Health &... Ch 14. Cancer, Abnormal Cells & Pharmacology Chemotherapy vs. Radiation How Does Chemotherapy Kill Cancer Cells? Neoplastic Etiology: Definition & Treatment3:20 Neoplasm vs. Tumor: Definitions & Differences
- Pulmonary metastasis is seen in 20-54% of extrathoracic malignancies. [1] Lungs are the second most frequent site of metastases from extrathoracic malignancies. Twenty percent of metastatic disease is isolated to the lungs. [1] The development of pulmonary metastases in patients with known malignancies indicates disseminated disease and places the patient in stage IV in TNM (tumor, node, metastasis) staging systems. This typically implies an adverse prognosis and alters the management plan. Imaging plays an important role in the screening and detection of pulmonary metastases. Imaging guidance is also used in histologic confirmation of metastatic disease. In patients with poor cardiorespiratory function and comorbidities, imaging-guided thermal ablation procedures are an effective alternative to surgical resection to improve survival. Chest radiography (CXR) is the initial imaging modality used in the detection of suspected pulmonary metastasis in patients with known malignancies. Chest CT scanning without contrast is more sensitive than CXR
- الحمضيات الخضراوات الصليبية مثل البروكلي ، والملفوف ، وبراعم بروكسل ، وبوك تشوي وغيرها من الخضر الآسيوي.