
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Anemia
Semelhante a Anemia (20)
Mais de HIRENGEHLOTH
Mais de HIRENGEHLOTH (20)
Último
Último (20)
Anemia
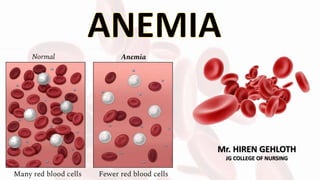
- 1. Mr. HIREN GEHLOTH JG COLLEGE OF NURSING
- 2. • Anemia is a major killer in India. • Statistics reveal that every second Indian woman is anemic • One in every five maternal deaths is directly due to anemia. • Anemia affects both adults and children of both sexes, although pregnant women and adolescent girls are most susceptible and most affected by this disease. INTODUCTION
- 3. ‘’Anemia is a condition in which the hemoglobin concentration is lower than normal; it reflects the presence of fewer than the normal number of erythrocytes within the circulation.’’ As a result, the amount of oxygen delivered to body tissues is also diminished. Anemia is not a specific disease state but a sign of an underlying disorder. It is by far the most common hematologic condition. DEFINITION
- 10. • Iron Deficiency Anemia: • Iron deficiency anemia typically results when the intake of dietary iron is inadequate for hemoglobin synthesis. • The most common cause of iron deficiency anemia in men and postmenopausal women is bleeding from ulcers, gastritis, inflammatory bowel disease, or GI tumors. • The most common causes of iron deficiency anemia in premenopausal women are menorrhagia (ie, excessive menstrual bleeding) and pregnancy with inadequate iron supplementation. • Patients with chronic alcoholism often have chronic blood loss from the GI tract, which causes iron loss and eventual anemia. Other causes include iron malabsorption, as is seen after gastrectomy or with celiac disease.
- 11. • Anemia of Chronic Disease • The term anemia of chronic disease is a misnomer in that only the chronic diseases of inflammation, infection, and malignancy cause this type of anemia. • Many chronic inflammatory diseases are associated with a normochromic, normocytic anemia (ie, the erythrocytes are normal in color and size).
- 12. • Aplastic Anemia: • Aplastic anemia is a rare disease caused by a decrease in or damage to marrow stem cells, damage to the microenvironment within the marrow, and replacement of the marrow with fat. • The precise etiology is unknown, but it is hypothesized that the body’s T cells mediate an inappropriate attack against the bone marrow resulting in bone marrow aplasia (ie, markedly reduced hematopoiesis). Therefore, in addition to severe anemia, significant neutropenia and thrombocytopenia (ie, a deficiency of platelets) also occur.
- 13. • Megaloblastic Anemia: • In the anemias caused by deficiencies of vitamin B12 or folic acid, identical bone marrow and peripheral blood changes occur because both vitamins are essential for normal DNA synthesis. In either anemia, the erythrocytes that are produced are abnormally large and are called megaloblastic red cells. Folic Acid Deficiency The folate stores in the body are much smaller than those of vitamin B12, and they are quickly depleted when the dietary intake of folate is deficient (within 4 months). Folate is found in green vegetables and liver. Folate deficiency occurs in people who rarely eat uncooked vegetables.
- 14. Vitamin B12 Deficiency • A deficiency of vitamin B12 can occur in several ways. Inadequate dietary intake is rare but can develop in strict vegetarians who consume no meat or dairy products. • Faulty absorption from the GI tract is more common. • This occurs in conditions such as Crohn’s disease, or after ileal resection or gastrectomy.
- 15. • Another cause is the absence of intrinsic factor, as in pernicious anemia. Intrinsic factor is normally secreted by cells within the gastric mucosa; it binds with dietary vitamin B12 and travels with it to the ileum, where the vitamin is absorbed. Without intrinsic factor, orally consumed vitamin B12 cannot be absorbed, and erythrocyte production is eventually diminished. • Even if adequate vitamin B12 and intrinsic factor are present, a deficiency may occur if disease involving the ileum or pancreas impairs absorption. • Pernicious anemia, which tends to run in families, is primarily a disorder of adults, particularly the elderly.
- 16. • Hemolytic Anemia: • In hemolytic anemias, the erythrocytes have a shortened lifespan; thus, their number in the circulation is reduced. • Fewer erythrocytes result in decreased available oxygen, causing hypoxia, which in turn stimulates an increase in erythropoietin release from the kidney. The erythropoietin stimulates the bone marrow to compensate by producing new erythrocytes and releasing some of them into the circulation somewhat prematurely as reticulocytes. • If the red cell destruction persists, the hemoglobin is broken down excessively; about 80% of the heme is converted to bilirubin, conjugated in the liver, and excreted in the bile.
- 17. • Sickle Cell Anemia: • Sickle cell anemia is a severe hemolytic anemia that results from inheritance of the sickle hemoglobin gene. This gene causes the hemoglobin molecule to be defective. • The sickle hemoglobin (HbS) acquires a crystal-like formation when exposed to low oxygen tension. • The oxygen level in venous blood can be low enough to cause this change; consequently, the erythrocyte containing HbS loses its round, pliable, biconcave disk shape and becomes deformed, rigid, and sickle shaped.
- 25. ASSESSMENT AND DIAGNOSTIC EVALUATION • Complete hematologic studies (eg, hemoglobin, hematocrit, reticulocyte count, and red blood cell (RBC) indices, particularly The mean corpuscular volume [MCV] and RBC distribution width [RDW]) • Iron studies (serum iron level, total iron-binding capacity [TIBC], percent saturation, and ferritin) • Serum vitamin B12 and folate levels; haptoglobin and erythropoietin levels • Bone marrow aspiration • Other studies as indicated to determine underlying illness
- 26. MEDICAL MANAGEMENT • Management of anemia is directed toward correcting or controlling the cause of the anemia. • if the anemia is severe, the erythrocytes that are lost or destroyed may be replaced with a transfusion of packed RBCs (PRBCs). The treatment aims to increase the number of RBCs, which, in turn, increases the amount of oxygen in the blood. •Iron-deficiency anemia: Iron supplements and dietary changes can help, and, when relevant, a doctor will identify and address the cause of excessive bleeding.
- 27. •Vitamin B-12 deficiency anemia: Treatments can include dietary supplements and vitamin B-12 shots. •Thalassemia: Treatments include folic acid supplements, iron chelation, and, for some people, blood transfusions and bone marrow transplants. •Anemia due to chronic disease: The doctor will focus on resolving the underlying condition. •Aplastic anemia: Treatment involves blood transfusions or bone marrow transplants •Sickle cell anemia: Treatment typically involves oxygen therapy, pain relief medication, and intravenous fluids, but it can also include antibiotics, folic acid supplements, blood transfusions, and a cancer drug called hydroxyurea. •Hemolytic anemia: The treatment plan may include immunosuppressant drugs, treatments for infections, and plasmapheresis, which filters the blood.
- 28. NURSING MANAGEMENT Assessment: • Obtain a health history, perform a physical examination, and obtain laboratory values. • Ask patient about extent and type of symptoms experienced and impact of symptoms on lifestyle; medication history; alcohol intake; athletic endeavors (extreme exercise). • Ask about family history of inherited anemias. • Perform nutritional assessment: Ask about dietary habits resulting in nutritional deficiencies, such as those of iron, vitamin B12, and folic acid. • Monitor relevant laboratory test results; note changes.
- 29. • Assess cardiac status (for symptoms of increased workload or heart failure): tachycardia, palpitations, dyspnea, dizziness, orthopnea, exertional dyspnea, cardiomegaly, hepatomegaly, peripheral edema. • Assess for GI function: nausea, vomiting, diarrhea, melena or dark stools, occult blood, anorexia, glossitis; women should be questioned about their menstrual periods (eg, excessive menstrual flow, other vaginal bleeding) and the use of iron supplements during pregnancy. • Assess for neurologic deficits (important with pernicious anemia): presence and extent of peripheral numbness and paresthesias, ataxia, poor coordination, confusion.
- 30. Nursing Diagnoses • Fatigue related to decreased hemoglobin and diminished oxygen- carrying capacity of the blood • Altered nutrition, less than body requirements, related to inadequate intake of essential nutrients • Altered tissue perfusion related to inadequate hemoglobin and hematocrit.
- 31. NURSING INTERVENTIONS Managing Fatigue • Assist patient to prioritize activities and establish a balance between activity and rest. • Encourage patient with chronic anemia to maintain physical activity and exercise to prevent deconditioning. Maintaining Adequate Nutrition • Encourage a healthy diet. • Teach patient to avoid or limit intake of alcohol. • Plan dietary teaching sessions for patient and family; consider cultural aspects of nutrition. • Discuss nutritional supplements (eg, vitamins, iron, folate) as prescribed.
- 32. Maintaining Adequate Perfusion • Monitor vital signs and pulse oximeter readings closely, and adjust or withhold medications (antihypertensives) as indicated. • Administer supplemental oxygen, transfusions, and IV fluids as ordered. Monitoring and Managing Complications • Assess patient with anemia for heart failure. • Perform a neurologic assessment for patients with known or suspected megaloblastic anemia. Expected Patient Outcomes • Reports less fatigue • Attains and maintains adequate nutrition • Maintains adequate perfusion • Experiences no or minimal complications