Necrotizing ulcerative gingivitis & periodontits
•Transferir como DOCX, PDF•
52 gostaram•11,353 visualizações

NOTE : all this from my reading in some scientific website and articles I hope that you enjoy and you benefit❤

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Necrotizing ulcerative gingivitis & periodontits
Semelhante a Necrotizing ulcerative gingivitis & periodontits (20)
Mais de DrGhadooRa
Mais de DrGhadooRa (19)
Último
Último (20)
Necrotizing ulcerative gingivitis & periodontits
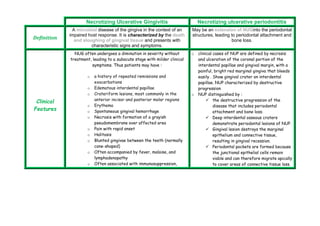
- 1. Necrotizing Ulcerative Gingivitis Necrotizing ulcerative periodontitis Definition A microbial disease of the gingiva in the context of an impaired host response. It is characterized by the death and sloughing of gingival tissue and presents with characteristic signs and symptoms. May be an extension of NUGinto the periodontal structures, leading to periodontal attachment and bone loss. Clinical Features NUG often undergoes a diminution in severity without treatment, leading to a subacute stage with milder clinical symptoms. Thus patients may have : o a history of repeated remissions and exacerbations o Edematous interdental papillae o Crateriform lesions, most commonly in the anterior incisor and posterior molar regions o Erythema o Spontaneous gingival hemorrhage o Necrosis with formation of a grayish pseudomembrane over affected area o Pain with rapid onset o Halitosis o Blunted gingivae between the teeth (normally cone-shaped) o Often accompanied by fever, malaise, and lymphadenopathy o Often associated with immunosuppression, o clinical cases of NUP are defined by necrosis and ulceration of the coronal portion of the interdental papillae and gingival margin, with a painful, bright red marginal gingiva that bleeds easily . Show gingival crater on interdental papillae. NUP characterized by destructive progression o NUP distinguished by : the destructive progression of the disease that includes periodontal attachment and bone loss. Deep interdental osseous craters demonstrate periodontal lesions of NUP. Gingival lesion destroys the marginal epithelium and connective tissue, resulting in gingival recession. Periodontal pockets are formed because the junctional epithelial cells remain viable and can therefore migrate apically to cover areas of connective tissue loss.
- 2. tobacco use, and physical or emotional stress; the vernacular name 'trench mouth' came from large outbreaks in the World War I trenches. The disease is also seen in college dormitories and other stressful crowded living conditions, but there is no evidence that acute necrotizing ulcerative gingivitis is communicabl Tooth mobility Ultimately tooth loss. NUP patient may present with : Oral malodor ( foul odor ) Fever Malaise lymphadenopathy Microscopic Findings Surface epithelium is destroyed and replaced by a meshwork of fibrin, necrotic epithelial cells, polymorphonuclear leukocytes (PMNs, neutrophils), and various types of microorganisms individual cells exhibit varying degrees of hydropic degeneration. Commonly similar to NUG 1 - surface biofilm composed of a mixed microbial flora with different morphotypes and a subsurface flora with dense aggregations of spirochetes ( bacterial zone ). 2 - Dense aggregations of PMNs ( neutrophil-rich zone ) . 3 - N ecrotic cells ( necrotic zone ). 4 - S pirochetal infiltration zone. 5 - High levels of yeasts and herpes-like viruses were observed Etiology Build-up of bacterial plaque on the teeth, adjacent gingivae, and pockets between teeth and gums, releasing toxins that cause an inflammatory response (most common species involved are Gram-negative anaerobic bacteria—Actinobacillus Etiology of NUP Generally as NUG: 1- Bacteria role: NUP in HIV-positive patients demonstrated significantly greater numbers of the opportunistic fungus Candida albicans and a higher prevalence of A. actinomycetemcomitans , P. intermedia , P. gingivalis , Fusobacterium nucleatum , and
- 3. actinomycetemcomitans and Porphyromonas gingivalis) Build-up of calculus contributes to the chronicity of periodontal disease; if plaque is not removed, it forms a hard mass commonly called 'tartar,' which traps bacteria that cause gingivitis. Toxins released from the bacteria stimulate an immune response (via cytokines) that increases production of collagenase. Untreated, this has a destructive effect on the connective tissue, which renders the teeth less secure, leading to periodontal disease and tooth loss Smoking tobacco Faulty dental prosthesis Malocclusion Breathing through the mouth Local trauma (eg, an overly aggressive toothbrushing technique) Dry mouth: because of loss of protective effect of Campylobacter species compared with HIV-negative controls . L ow or variable level of spirochetes , which is inconsistent with the flora associated with NUG . 2- Immunocompromised Status : Clearly, both NUG and NUP lesions are more prevalent in patients with compromised or suppressed immune systems. Commonly in HIV-positive and AIDS patients. 3- Psychologic Stress Stress increases systemic cortisol levels , and sustained increases in cortisone have a suppressive effect on the immune response by microcirculation in gingiva and altered phagocytic functions. Some researchers: F ound that urinary levels of 17- hydroxycorticosteroid were higher in subjects with NUG than in all other subjects diagnosed with periodontal health , gingivitis , or periodontitis 4- Malnutrition Direct evidence of the relationship between malnutrition and necrotizing periodontal disease is limited to descriptions of necrotizing infections in severely malnourished children. M any of the host defenses , including phagocytosis; cell-
- 4. saliva Vitamin deficiency, especially of vitamin C mediated immunity ; and complement, antibody , and altered cytokine production , are impaired in malnourished individuals 5- Reduction of nutrients to cells and tissues results in immunosuppression and disease susceptibility. Malnutrition can predispose an individual to opportunistic infections or intensify the severity of current oral infections 6- Other factors - Smoking - Plaque and other local factors e.g. calculus Predisposing factors Preexisting gingivitis, injury to the gingiva, smoking , nutritional deficiency; fatigue caused by chronic sleep deficiency; other health habits (e.g., alcohol or drug abuse), and systemic disease (e.g., diabetes, debilitating infection). Poor oral hygiene, preexisting periodontal disease, smoking, viral infections, immunocompromised status, psychosocial stress, and malnutrition Complication And comorbidities If oral hygiene is poor, plaque accumulates and can form calculus; both harbor toxin-releasing bacteria around the gum line. Eating carbohydrate-containing foods promotes an acid environment in the mouth that encourages bacterial growth Crowns or fillings that are poorly contoured provide traps for food particles Smoking has a significant effect on overall dental health Gangrenous (necrotic) stomatitis : extensive necrotic process to adjacent gingival mucosa (check, palate, tongue, floor of m., lips)
- 5. Coexisting diseases such as diabetes mellitus Down syndrome, and HIV infection render a patient more susceptible to the inflammatory process Degenerative disease of the connective tissue such as rheumatoid arthritis, systemic lupus erythematosus, and CREST syndrome (calcinosis, Raynaud phenomenon, esophageal dysfunction, sclerodactyly, and telangiectasia) may make a person more susceptible to periodontal disease Sjögren syndrome or xerostomia can cause dryness of the mouth, which increases the likelihood of oral pathology Steroid medication may increase a patient's susceptibility to bacteria Ill-fitting dentures or restorations should be properly fitted Noma ( cancrum oris ): serious (fatal ) form of necrotic stomatitis that lead to exposure of bone and perforation of check & nasal cavity Treatment Treatment usually is divided into the acute phase and the maintenance phase. The primary concern in the acute phase is pain control. For the maintenance phase, treatment is directed toward reducing the burden of potential pathogens, preventing further tissue destruction, and promoting healing. For uncomplicated NUP or NUG, the primary care provider should prescribe an antimicrobial rinse , antibiotic therapy , medications for pain management, and nutritional supplementation; the patient should be referred to a dental health care professional. The treatment is mostly similar to NUG 1- Lavage of necrotic tissue and pseudomembrane under local anesthesia. 2 - Correction of the systemic condition as possible and consultation with patient’s physician . 3- Periodontal debridement ( scaling and root planing ). 4- Local and systemic antibiotics 5- Antiseptic mouth wash ( chlorhexidine )
- 6. Chlorhexidine gluconate rinse (0.12%) twice daily after brushing and flossing (an alcohol-free preparation is preferred). Antibiotic therapy (preferably narrow spectrum, to leave gram-positive aerobic flora unperturbed). Refer to a dentist for the following: Removal of plaque and debris from the site of infection and inflammation. Debridement of necrotic hard and soft tissues, with a 0.12% chlorhexidine gluconate or povidone-iodine lavage 6 - Antifungal and antiviral drugs 7- Good nutrition and enhancement the psychic status. 8 - Oral hygiene instruction and patient motivation to control dental plaque. 9 - Maintenance recall visits to evaluate periodontal health and observe the recurrence of lesions.