Immunohistochemical Analysis of Hypoxia-Inducible Factor 1-Alpha and Ki-67 Expression in Placenta Previa and Accreta

Objective: To investigate the immunohistochemical staining of hypoxia-inducible factor 1-alpha (HIF-1α) and Ki-67 expression in the placenta of pregnant women with placenta previa and placenta accreta. Study Design: Thirty placentas (10 normotensive, 10 placenta previa, and 10 placenta accreta) were processed for routine histological tissue processing. The biochemical parameters of patients were recorded. Placentas were stained with hematoxylin-eosin and HIF-1α and Ki-67 immunostaining. Results: Normal histology was observed in placentas of normotensive pregnant women. Placenta previa sections showed increased syncytial knots, intervillous hemorrhage, fibrin accumulation, and hyalinization. In placenta accreta sections, increased syncytial nodes, vascular dilation/congestion, fibrin accumulation, and hyalinization were observed. Normotensive placentas showed no HIF-1α expression. In placenta previa tissues, high HIF-1α expression was observed in vascular endothelial cells, villous stromal cells, and syncytial knots. High HIF-1α expression was recorded in villous stromal cells and cytotrophoblast cells in placenta accreta. In normotensive placental tissues, no Ki-67 expression was observed. In placenta previa sections, high Ki-67 expression was observed mostly in root villi stromal cells and some endothelial cells. High Ki-67 expression was observed mostly in villi stromal cells of placenta accreta. Conclusion: It is thought that HIF-1α is an important regulatory gene in the development of villus in trophoblast invasion such as placenta accreta and previa, while Ki-67 will play a key role in the development of abnormal placenta with its stimulating effect on inflammatory cell development and angiogenesis in accreta and preeclampsia.

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Immunohistochemical Analysis of Hypoxia-Inducible Factor 1-Alpha and Ki-67 Expression in Placenta Previa and Accreta
Semelhante a Immunohistochemical Analysis of Hypoxia-Inducible Factor 1-Alpha and Ki-67 Expression in Placenta Previa and Accreta (20)
Mais de ANALYTICAL AND QUANTITATIVE CYTOPATHOLOGY AND HISTOPATHOLOGY
Mais de ANALYTICAL AND QUANTITATIVE CYTOPATHOLOGY AND HISTOPATHOLOGY (20)
Último
Último (20)
Immunohistochemical Analysis of Hypoxia-Inducible Factor 1-Alpha and Ki-67 Expression in Placenta Previa and Accreta
- 1. 143 OBJECTIVE: To investigate the immunohistochemical staining of hypoxia-inducible factor 1-alpha (HIF-1α) and Ki-67 expression in the placenta of pregnant women with placenta previa and placenta accreta. STUDY DESIGN: Thirty placentas (10 normotensive, 10 placenta previa, and 10 placenta accreta) were processed for routine histological tissue processing. The biochemical parameters of patients were recorded. Placentas were stained with hematoxylin-eosin and HIF- 1α and Ki-67 immunostaining. RESULTS: Normal histology was observed in placentas of normotensive pregnant women. Placenta previa sections showed increased syncytial knots, intervillous hemorrhage, fibrin accumulation, and hyalinization. In placenta accreta sections, increased syncytial nodes, vascular dilation/congestion, fibrin accumulation, and hyalinization were observed. Normotensive placentas showed no HIF-1α expression. In placenta previa tis sues, high HIF-1α expression was observed in vascular endothelial cells, villous stromal cells, and syncytial knots. High HIF-1α expression was recorded in villous stromal cells and cytotrophoblast cells in placenta ac- creta. In normotensive placental tissues, no Ki-67 ex- pression was observed. In placenta previa sections, high Ki-67 expression was observed mostly in root villi stromal cells and some endothelial cells. High Ki-67 expression was observed mostly in villi stromal cells of placenta accreta. CONCLUSION: It is thought that HIF-1α is an im- portant regulatory gene in the development of villus in trophoblast invasion such as placenta accreta and previa, while Ki-67 will play a key role in the develop ment of abnormal placenta with its stimulating effect on inflammatory cell development and angiogenesis in accreta and preeclampsia. (Anal Quant Cytopathol Histpathol 2021;43:143–149) Keywords: female; hypoxia; hypoxia-inducible factor 1, alpha subunit; placenta; placenta accreta; placenta previa; placental lactogen; pregnancy, physiology; preeclampsia. The placenta is a temporary organ that nourishes the fetus, regulates many metabolic activities, and produces hormones necessary for the continuation of pregnancy; its function ends at the end of pregnancy.1 The placenta is implanted in any area of the uterine wall; however, in some clinical complications, it can prevent the fetal head from descending during delivery if it is too low in the uterus. Low-lying placentas can also cause unusual bleeding during pregnancy or delivery.2 Analytical and Quantitative Cytopathology and Histopathology® 0884-6812/21/4303-0143/$18.00/0 © Science Printers and Publishers, Inc. Analytical and Quantitative Cytopathology and Histopathology® Immunohistochemical Analysis of Hypoxia- Inducible Factor 1-Alpha and Ki-67 Expression in Placenta Previa and Accreta Serap Otçu, M.D., and Engin Deveci, Ph.D. From the Department of Obstetrics and Gynecology, Health Sciences University, Diyarbakır Gazi Yaşargil Training and Research Hospi- tal, Diyarbakır; and the Department of Histology and Embryology, Faculty of Medicine, Dicle University, Diyarbakır, Turkey. Serap Otçu is Physician, Department of Obstetrics and Gynecology, Health Sciences University, Diyarbakır Gazi Yaşargil Training and Research Hospital. Engin Deveci is Professor and Head, Department of Histology and Embryology, Faculty of Medicine, Dicle University. Address correspondence to: Engin Deveci, Ph.D., Department of Histology and Embryology, Faculty of Medicine, Dicle University, 21280 Diyarbakır, Turkey (engindeveci64@gmail.com) Financial Disclosure: The authors have no connection to any companies or products mentioned in this article.
- 2. As the embryo develops, substance exchange between fetal and maternal blood circulation to- wards the end of pregnancy can decrease due to some abnormal structural changes such as thick ening of the basement membrane of fetal capil- laries, increased fibrous tissue in the villous stro- ma, and fibrinoid accumulation in the chorionic plate and on root villi in the junction.3,4 Placenta previa occurs when the placenta at- taches to the inside of the uterus, near or above the cervical opening. It affects about 0.5% of pregnan cies. Risk factors include pregnancy in advanced age, smoking, pre-aspiration and curettage, mul tiparity, previous cesarean surgery, labor induc- tion, or termination of pregnancy. Incidence of placenta previa is 1 in 300 deliveries.5,6 Placenta previa can cause severe complications, such as maternal placenta accreta, low blood pressure or postpartum hemorrhage, and fetal growth re- striction. The etiology of placenta previa is not fully known, but there is a relationship between abnormal endometrial vascularization due to scar ring or atrophy from previous trauma, surgery, infection, and uterine scarring.7,8 Placenta accreta is the abnormal adhesion of the placenta to the uterine cavity. It is characterized by the absence of decidua basalis and by the incomplete development of the fibrinoid layer. Placenta accreta occurs in 5–10% of pregnancies complicated with placenta previa. Its incidence ranges from about 533 to 70,000 births.9 The best- defined risk factors are previous uterine surgery and placenta previa. Although risk factors for placental attachment anomaly are well defined, the correct etiology is largely unknown. Abnormal or increased trophoblast invasion is seen. The etiology of the placenta accreta is that the oxygen imbalance in the uterine scar area causes this con dition. The development of the embryo in a relatively hypoxic environment causes prolifera- tion or increased invasion of cytotrophoblasts.10,11 The aim of this study is to investigate HIF-1α and Ki-67 expression in placenta previa and accreta and to compare the expression differences. Materials and Methods Ethical approval was obtained from Dicle Univer sity Faculty of Medicine Non-Interventional Clin- ical Research Ethics Committee (record no. 2020/ 68). In our study, 10 normotensive, 10 placenta previa, and 10 placenta accreta tissue samples from pregnant women (regardless of age) were obtained from Gynecology and Obstetrics Clinics, Gazi Yasargil Training and Research Hospital. All patients signed the informed patient consent form. Biochemical parameters for each patient were recorded. Placental tissues were processed for routine paraffin wax embedding protocol. Histological Tissue Processing Placental tissues were fixed with zinc-formalin so- lution (catalog no. Z2902, Sigma-Aldrich, St. Louis, Missouri, USA) and washed under tap water for 5 minutes. Tissues were passed through ascend ing alcohol series for about 24 hours. Tissues were washed with xylene 2×30 minutes and incubated within paraffin wax. Sections of 5 µm were cut with a microtome (catalog no. RM2265, Leica, Wetzlar, Germany). Deparaffinized within xylene for 2×30 minutes, sections were brought to dis tilled water. Some of the sections were stained with routine hematoxylin and eosin, and the rest were kept for immunohistochemical staining. HIF-1α and Ki-67 Immunostaining All placental tissues were brought to distilled water. Hydrogen peroxide solution (catalog no. TA-015-HP, Thermo Fisher, Fremont, California, USA) was dropped on sections for 20 minutes. After washing in PBS for 3×5 minutes, Ultra V Block (catalog no. TA-015-UB, Thermo Fisher) was applied to sections for 8 minutes. Sections were incubated with primary antibodies anti-HIF-1α (catalog no. ab216842, Abcam, Cambridge, Massa chusetts, USA) and anti-Ki-67 (catalog no. ab16667, Abcam) at +4°C overnight. Sections were allowed to warm at room temperature for 30–60 minutes. Sections were washed with biotinylated secondary antibody (catalog no. TP-015-BN, Thermo Fisher) for 14 minutes. Streptavidin-peroxidase (catalog no. TS-015-HR, Thermo Fisher) was dropped onto sections for 15 minutes. Clearing with PBS, DAB (catalog no. TA-001-HCX, Thermo Fisher) was used as chromogen. Sections were counterstained with Gill hematoxylin (catalog no. 105174, Sigma- Aldrich) and mounted with Entellan (catalog no. 107961, Sigma-Aldrich). Slides were analyzed with Zeiss Imager A2 Zen 3.0 software (Carl Zeiss, Oberkochen, Germany) and photomicrographed. Statistical Analysis The data were recorded as arithmetic mean± standard deviation with mean rank value. Statis tical analysis was done using the IBM SPSS 25.0 144 Analytical and Quantitative Cytopathology and Histopathology® Otçu and Deveci
- 3. software (IBM SPSS Statistics for Windows, Version 25.0, released 2017. IBM Corp., Armonk, New York, USA). One-way ANOVA with Tukey’s test was used for multiple comparisons. P<0.05 was used as the significance level. Results Statistical analysis of multiple comparisons be- tween normotensive, placenta previa, and placen ta accreta is shown in Table I. No statistical dif- ferences were recorded within group comparisons for any parameters (ALT, AST, glucose, albumin, total protein, urea, creatinine). Graphical illustra- tions of all parameters are shown in Figures 1–2. Placenta previa and accreta were stained with hematoxylin-eosin and HIF-1α and Ki-67 immu nohistochemical staining. The staining is present ed in Figure 2. Normotensive placentas showed normal placental histology (Figure 2A). In sections of placenta previa, increased syncytial knots, in- tervillous hemorrhage, fibrin accumulation, and hyalinized regions were observed (Figure 2B). Similar to placenta previa, placenta accreta show ed similar histopathology with increased syncytial nodes, vascular dilation/congestion, fibrin accu mulation, and hyalinization (Figure 2C). In HIF- 1α immunohistochemical staining, no expression was recorded in normotensive placental tissues. In placenta previa tissues, high HIF-1α expres- sion was observed in vascular endothelial cells, villous stromal cells, and syncytial knots (Figure 2E). High HIF-1α expression was recorded in villous stromal cells and cytotrophoblast cells in placenta accreta (Figure 2F). No Ki-67 expression was recorded in normotensive placental tissues (Figure 2G). Placenta previa showed high Ki-67 expression mostly in root villi stromal cells and some endothelial cells (Figure 2H). High Ki-67 expression was observed mostly in villi stromal cells of placenta accreta (Figure 2I). Discussion In this study we investigated the tissues of placen ta previa and placenta accreta by biochemical and immunohistochemical methods. Placenta previa is a pregnancy complication in which placentation is abnormally localized in the lower segment of the uterus.12 It is one of the important causes of maternal, fetal, and neonatal morbidity and mor tality characterized by third trimester bleeding. Al- though its etiology is unknown, advanced mater nal age, multiparity, multiple pregnancy, previous cesarean delivery, and smoking are risk factors, causing placenta previa.6 Studies on histopathol ogy of placenta previa revealed fibrinoid necrosis, polymorphonuclear cell infiltration, abnormal vas culatures, and dilated vessels. Biswas et al recorded increased trophoblastic giant cells, hemorrhage, absence of chorionic villi in the myometrium, and inflammation in placenta previa tissues.13 Silver et al also reported increased villous infarction with fibrinoid and congested vessels in pathological examination of placenta previa.14 In our study, we observed increased syncytial knots, intervillous hemorrhage, fibrin accumulation, and hyalinized regions in placenta previa sections (Figure 1B). Placenta accreta is defined as abnormally deep adhesion of the placenta to the uterine muscles. Its etiology is not fully known, but placenta previa and previous cesarean deliveries are risk factors. Complications include premature birth, maternal bleeding, and morbidity.15 Histopathological anal ysis of placenta accreta showed chorionic villi adjacent to myometrial fibers, fibrinoid formation, intravascular chorionic villi, hemorrhage, and vas cular changes.14 In our study we observed in- creased syncytial nodes, vascular dilation/conges tion, fibrin accumulation, and hyalinization in placenta accreta tissues. Perinatal studies have focused on the role of oxygen and hypoxia during placentation and pregnancy. Researchers have shown that oxygen has vital functions to regulate trophoblast differ entiation.14 Hypoxia-inducible factor-1α (HIF-1α) is a transcription regulator of genes in adaptive re- sponse to hypoxic conditions. HIF-1α is involved in activation of transcription of over 40 genes such as erythropoietin, glucose transporters, gly- colytic enzymes, and vascular endothelial growth factor during hypoxia. HIF-1α regulates vessel formation in the embryonic stage, tumor angio genesis, and ischemia.16 During placental forma tion, cellular hypoxia develops, and thus HIF-1α is activated to induce trophoblast proliferation and the formation of specific cell subtypes.17,18 Zamudio et al investigated HIF-1α expression and its regu latory mechanisms in placentas from pregnancies of women living at different altitudes. HIF-1α were overexpressed in placentas of women living at high altitudes.19 Ietta et al investigated the role of HIF-1α expression during human placen tal development. Expression of HIF-1α was high when oxygen tension was low but decreased when placental oxygen tension increased. They also Volume 43, Number 3/June 2021 145 HIF-1-α and Ki-67 in Placenta Previa and Accreta
- 4. showed that during early placentation, HIF-1α localized in cytotrophoblasts.20 In our study we found that placenta previa tissues showed high HIF-1α expression in vascular endothelial cells, 146 Analytical and Quantitative Cytopathology and Histopathology® Otçu and Deveci Table I Means and Standard Deviations of Age, ALT, AST, Glucose, Albumin, Total Protein, Urea, and Creatinine with Group Comparisons One-way ANOVA Parameter Group N Mean+SD (p value) Age, years (1) Normotensive 20 33.35±4.72 (2): 0.868 (3): 0.082 (2) Placenta previa 20 32.55±5.04 (1): 0.868 (3): 0.221 (3) Placenta accreta 20 29.90±5.18 (1): 0.082 (2): 0.221 ALT, U/L (1) Normotensive 20 29.90±5.18 (2): 0.241 (3): 1.00 (2) Placenta previa 20 32.55±5.04 (1): 0.241 (3): 0.241 (3) Placenta accreta 20 29.90±5.18 (1): 1.00 (2): 0.241 AST, U/L (1) Normotensive 20 13.14±8.60 (2): 1.00 (3): 1.00 (2) Placenta previa 20 13.11±6.34 (1): 1.00 (3): 1.00 (3) Placenta accreta 20 13.14±8.60 (1): 1.00 (2): 1.00 Glucose, mg/dL (1) Normotensive 20 18.67±7.41 (2): 0.886 (3): 1.00 (2) Placenta previa 20 20.13±13.43 (1): 0.886 (3): 0.886 (3) Placenta accreta 20 18.67±7.41 (1): 1.00 (2): 0.886 Albumin, g/L (1) Normotensive 20 86.80±25.99 (2): 0.425 (3): 1.00 (2) Placenta previa 20 97.06±25.39 (1): 0.425 (3): 0.425 (3) Placenta accreta 20 86.80±25.99 (1): 1.00 (2): 0.425 Total protein, g/dL (1) Normotensive 20 21.84±16.42 (2): 0.479 (3): 1.00 (2) Placenta previa 20 27.72±14.97 (1): 0.479 (3): 0.479 (3) Placenta accreta 20 21.84±16.42 (1): 1.00 (2): 0.479 Urea, mg/dL (1) Normotensive 20 38.38±27.08 (2): 0.736 (3): 1.00 (2) Placenta previa 20 31.59±31.53 (1): 0.736 (3): 0.479 (3) Placenta accreta 20 38.38±27.08 (1): 1.00 (2): 0.736 Creatinine, mg/dL (1) Normotensive 20 16.43±4.91 (2): 0.337 (3): 1.00 (2) Placenta previa 20 19.19±8.03 (1): 0.337 (3): 0.337 (3) Placenta accreta 20 16.43±4.91 (1): 1.00 (2): 0.337 SD = standard deviation.
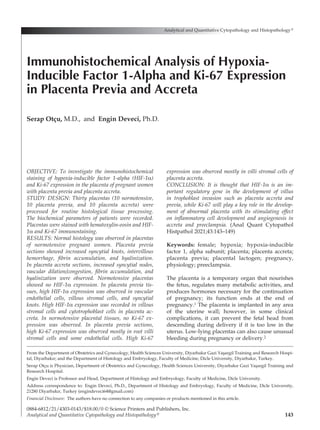
- 5. Volume 43, Number 3/June 2021 147 HIF-1-α and Ki-67 in Placenta Previa and Accreta Figure 1 Graphical illustration of patient parameters regarding placenta complication. Figure 2 Normotensive, placenta previa, and placenta accreta tissues with H-E staining (A–C) and HIF-1α (D–F) and Ki-67 (G–I) immunostainings. (A) Normal placental histology. (B) Increased syncytial nodes (black arrow), intervillous hemorrhage (red star), fibrinoid (black star), and hyalinization (arrowhead). (C) Increased syncytial nodes (black arrow), vascular dilation/congestion (red star), villous fibrinoid (black star), and hyalinization (arrowhead). (D) No HIF-1α in normotensive placental tissues. (E) High HIF-1α expression in vascular endothelial cells (red arrow), villous stromal cells (arrowhead), and syncytial nodes (black arrow). (F) High HIF-1α expression in villous stromal cells (arrowhead) and cytotrophoblast cells (black arrow). (G) No Ki-67 expression in normotensive placental tissues. (H) High Ki-67 expression mostly in root villi stromal cells (arrow) and some endothelial cells (red arrow). (I) High Ki-67 expression in mostly villi stromal cells (arrows).
- 6. villous stromal cells, and syncytial knots (Figure 1E). Placenta accreta tissues showed high HIF-1α expression in villous stromal cells and cytotro phoblast cells in placenta accreta (Figure 1F). Ki-67 is a cellular marker for proliferation which functions in interphase and mitotic cells. Mea- surement of Ki-67 expression level can be used for the prognosis of many tumors.21 Ki-67 expression index has been used in the normal placenta, hy- datidiform moles, and choriocarcinoma. Aberrant placenta formation may be related with abnor- mal regulation of molecular changes and the proliferation of trophoblast cells so that tropho blasts are able to migrate and invade the uterine wall.21,22 Kaya et al recorded that Ki-67 expression was increased in villous cytotrophoblasts of pre- eclamptic placentas relative to controls. They showed an increased number of villous cytotro phoblasts in preeclampsia as compared to in nor- mal pregnancy by analyzing with Ki-67 immuno histochemical staining.23 Unek et al showed that Ki-67 expression was increased in placental villi of preeclampsia.24 Another preeclampsia study recorded that the Ki-67 index was high in villous trophoblasts of preeclamptic patients.25 A study demonstrated that Ki-67 expression was high in trophoblast columns of accreta subtypes.26 In our study we found that placenta previa showed high Ki-67 expression mostly in root villi stromal cells and some endothelial cells (Figure 1H). We re- corded high Ki-67 expression mostly in villi stro- mal cells (Figure 1I). In conclusion, it is thought that HIF-1α is an important regulatory gene in the development of villus in trophoblast invasion such as placenta accreta and placenta previa, while Ki-67 will play a key role in the development of abnormal placen ta with its stimulating effect on inflammatory cell development and angiogenesis in accreta and pre eclampsia References 1. Handwerger S, Freemark M: The roles of placental growth hormone and placental lactogen in the regulation of hu- man fetal growth and development. J Pediatr Endocrinol Metab 2000;13(4):343-356 2. Yetter JF 3rd: Examination of the placenta. Am Fam Physi cian 1998;57(5):1045-1054 3. Freemark M: The roles of growth hormone, prolactin and placental lactogen in human fetal development. In Molecu- lar and Cellular Pediatric Endocrinology. Edited by S Hand werger. Totowa, New Jersey, Human Press 1999, pp 57-84 4. Handwerger S: Clinical counterpoint: The physiology of placental lactogen in human pregnancy. [Review]. Endocr Rev 1991;12:329-336 5. D’antonio F, Bhide A: Ultrasound in placental disorders. Best Prac Res Clin Obstet Gynaecol 2014;28(3):429-442 6. McShane PM, Heyl PS, Epstein MF: Maternal and perinatal morbidity resulting from placenta previa. Obstet Gynecol 1985;65:176-182 7. Crane JM, Van den Hof MC, Dodds L, Armson Ba, Liston R: Maternal complications with placenta previa. Am J Perinatol 2000;17(2):101-105 8. Ananth CV, Smulian JC, Vintzileos AM: The effect of placenta previa on neonatal mortality: A population-based study in the United States, 1989 during 1997. Am J Obstet Gynecol 2003;188(5):1299-1304 9. Oyelese Y, Smulian JC: Placenta previa, placenta accreta and vasa previa. Obstet Gynecol 2006;107(4):927-941 10. Arcario T, Greene M, Ostheimer GW, Datta S, Nauity JS: Risks of placenta previa/accreta in patients with pre- vious caesarean deliveries. Anesthesiology 1988;69(Suppl 3A):A 659 11. Miller DA, Chollet JA, Goodwin TM: Clinical risk factors for placenta previa placenta accreta. Am J Obstet Gynecol 1997;177:210-214 12. Lockwood CJ, Russo-Stieglitz K: Placenta previa: Epidemi ology, clinical feature, diagnosis, morbidity and mortality. Available at https:/ /www.uptodate.com/contents/placenta- previa-epidemiology-clinical-features-diagnosis-morbidity- and-mortality. Accessed April 28, 2020 13. Biswas R, Sawhney H, Dass R, Saran RK, Vasishta K: Histopathological study of placental bed biopsy in placenta previa. Acta Obstet Gynecol Scand 1999;78(3):173-179 14. Silver R: Abnormal placentation: Placenta previa, vasa previa, and placenta accreta. Obstet Gynecol 2015;126(3): 654-668 15. Khong TY: The pathology of placenta accreta, a worldwide epidemic. J Clin Pathol 2008;61:1243-1246 16. Soares MJ, Iqbal K, Kozai K: Hypoxia and placental de- velopment. Birth Defects Res 2017;109(17):1309-1329 17. Lee JW, Ko J, Ju C, et al: Hypoxia signaling in human diseases and therapeutic targets. Exp Mol Med 2019;51:1-13 18. Simmons DG, Cross JC: Determinants of trophoblast line age and cell subtype specification in the mouse placenta. Dev Biol 2005;284:12-24 19. Zamudio S, Wu Y, Ietta F, Rolfo A, Cross A, Wheeler T, Post M, Illsley NP, Caniggia I: Human placental hypoxia- inducible factor-1alpha expression correlates with clinical outcomes in chronic hypoxia in vivo. Am J Pathol 2007; 170(6):2171-2179 20. Ietta F, Wu Y, Winter J, Xu J, Wang J, Post M, Caniggia I: Dynamic HIF1A regulation during human placental devel opment. Biol Reprod 2006;75(1):112-121 21. Sun X, Kaufman PD: Ki-67: More than a proliferation mark er. Chromosoma 2018;127(2):175-186 22. Hilali N, Kocarslan S, Vural M, et al: Ki-67 proliferation index in patients with placenta previa percreta in the third trimester. Wien Klin Wochenschr 2015;127:98-102 23. Kaya B, Nayki U, Nayki C, Ulug P, Oner G, Gultekin E, 148 Analytical and Quantitative Cytopathology and Histopathology® Otçu and Deveci
- 7. Yildirim Y: Proliferation of trophoblasts and Ki67 expres- sion in preeclampsia. Arch Gynecol Obstet 2015;291(5):1041- 1046 24. Unek G, Oxmen A, Mendilcioglu I, Simsek M, Korgun ET: The expression of cell cycle related proteins PCNA, Ki67, p27 and p57 in normal and preeclamptic human placentas. Tissue Cell 2014;46:198-205 25. Arnholdt H, Meisel F, Fandrey K, Löhrs U: Proliferation of villous trophoblast of the human placenta in normal and abnormal pregnancies. Virchow Archiv B Cell Pathology 1991;60(6):365-372 26. Tantbirojn P, Crum CP, Parast MM: Pathophysiology of placenta creta: The role of decidua and extravillous tro phoblast. Placenta 2008;29(7):639-645 Volume 43, Number 3/June 2021 149 HIF-1-α and Ki-67 in Placenta Previa and Accreta