Changes in the Bladder After Spinal Cord Injury and Expression of VEGF and APAF-1

This study investigated the effects of spinal cord injury on the bladder tissue of rats. Twenty rats were divided into a control group and spinal cord injury (SCI) group. The SCI group exhibited statistically higher levels of oxidative stress markers (MDA, MPO), epithelial degeneration, vascular dilation, inflammation, and expression of VEGF and APAF-1 compared to the control group. The SCI group also had lower levels of the antioxidant GSH. Histological examination of the SCI group showed degeneration of epithelial cells, thickened fibrosis, dilated blood vessels, and increased VEGF and APAF-1 expression compared to the control group. The results suggest that spinal cord injury leads to increased oxidative stress, inflammation and apoptosis in

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Changes in the Bladder After Spinal Cord Injury and Expression of VEGF and APAF-1
Semelhante a Changes in the Bladder After Spinal Cord Injury and Expression of VEGF and APAF-1 (20)
Mais de ANALYTICAL AND QUANTITATIVE CYTOPATHOLOGY AND HISTOPATHOLOGY
Mais de ANALYTICAL AND QUANTITATIVE CYTOPATHOLOGY AND HISTOPATHOLOGY (20)
Último
Último (20)
Changes in the Bladder After Spinal Cord Injury and Expression of VEGF and APAF-1
- 1. 137 OBJECTIVE: A spinal cord injury (SCI) is damage to the spinal cord either from trauma, loss of its normal blood supply, or compression from tumor or infection. In this study we focused on alterations in the bladder tissue with angiogenic and apoptotic aspects after spinal cord injury. STUDY DESIGN: Twenty Wistar Albino rats were categorized as control and SCI groups. At T7-T9 ver- tebras, a steel rod was dropped from 10 cm to create a spinal cord injury under anesthesia. Rats were decapitat- ed and spinal tissue was processed to measure malondi- aldehyde (MDA), glutathione (GSH), and myeloperoxi- dase (MPO). RESULTS: MDA, MPO, epithelial degeneration, vascu- lar dilation, inflammation, VEGF, and APAF-1 expres- sions in the SCI group were statistically higher than those in the control group. GSH content of the SCI group was statistically lower than that in the control group. In the hematoxylin-eosin–stained sections of the control group, normal histology was observed in bladder tissue. In the SCI group, degeneration epithelial cells, thinned epithelium, increased fibrosis, dilated and congested blood vessels, and hyperplastic endothelial cells were observed. In the control group, VEGF expression was slightly observed in some epithelial cells and vascular cells. In the SCI group, VEGF expression was increased in inflammatory and vascular endothelial cells. For APAF-1 expression, the control group showed no ex- pression. In the SCI group, APAF-1 expression was positive in degenerated epithelial cells and connective tissue cells. CONCLUSION: It is thought that the urination reflex was affected due to increased inflammation in the blad- der tissue, leading to alterations in the regulation and function of the muscles. (Anal Quant Cytopathol Hist- pathol 2021;43:137–142) Keywords: APAF-1, bladder, spinal cord injury, urinary bladder, VEGF, vascular endothelial growth factor, Wistar rats. Spinal cord injury (SCI) is biphasic and is divided into primary and secondary mechanical damage. Flexion, extension, dislocation, distraction, frac- tures, ruptured disc material, gunshot wounds, contusion, laceration, and compression are com- mon clinical presentations of primary SCI. Second- ary injuries are caused by metabolic and biochem- ical reasons within hours after primary injury.1 A cascade of events triggered by secondary injury occurs as a result of activation of endogenous cell death. Energy deficiency due to ischemia is the most common characteristic of secondary SCI. The cellular response to hypoxia is cellular swell ing and increased intracellular Ca2+ ion, leading to activation of inflammatory and apoptotic mecha- Analytical and Quantitative Cytopathology and Histopathology® 0884-6812/21/4303-0137/$18.00/0 © Science Printers and Publishers, Inc. Analytical and Quantitative Cytopathology and Histopathology® Changes in the Bladder After Spinal Cord Injury and Expression of VEGF and APAF-1 Mehmet Yariş, M.D., and Engin Deveci, Ph.D. From the Department of Urology, Genesis Hospital, Diyarbakır; and the Department of Histology and Embryology, Medical School, Dicle University, Diyarbakır, Turkey. Mehmet Yariş is Surgeon, Department of Urology, Genesis Hospital. Engin Deveci is Professor and Head, Department of Histology and Embryology, Medical School, Dicle University. Address correspondence to: Engin Deveci, Ph.D., Department of Histology and Embryology, Medical Faculty, Dicle University, Diyar- bakır, Turkey (engindeveci64@gmail.com). Financial Disclosure: The authors have no connection to any companies or products mentioned in this article.
- 2. nisms.2 After SCI, neurogenic bladder dysfunction may occur due to neural pathways or neuromus- cular junctions which control the lower urinary tract interrupting the communication. Upper and lower neuron lesions may develop in neurogenic bladder dysfunction. Lower motor neuron lesions are lesions that develop at or below the conus medullaris. Efferent (motor), afferent (sensory), or both portions of the sacral arc pathway suffer because of these lesions, leading to no or de- creased reflexes of the detrusor muscle with a normal or underactive external sphincter. With a denervated or underactive external sphincter, coordination between detrusor contraction and sphincter relaxation occurs during bladder emp- tying.3 Upper motor neuron lesions are divided as intracranial and spinal lesions. In intracranial (suprapontine) lesions, cortical input that inhibits detrusor contractility is blocked. In spinal (supra- sacral or infrapontine) lesions, the region above the conus medullaris is affected and the sacral re- flex arc is spared.4,5 High expression of VEGF has been reported to be associated with immature angiogenesis in the bladder wall and bladder afferent nerve sensitiza- tion. It has been shown that visceral hyperalgesia and pelvic pain leads to, for example, neuropathic pain and inflammation, as well as a shift in VEGF alternative splice variant expression, as well as dif ferential effects on pain. Tooke et al also showed increased expression of total VEGF in the bladders of women with interstitial cystitis/bladder pain syndrome.6 APAF-1 is an important component of the apoptotic complex and is an important marker of the mitochondrial endogenous apoptotic path- way. After induction of apoptosis, cytochrome c is incorporated into the cytoplasm in the presence of ATP, which activates APAF-1 and induces con- formational changes in its protein, aggregating and activating procaspase-9 to form the apoptotic complex.7 In this study, it was aimed to investigate the angiogenic and apoptotic effects on the bladder after spinal cord injury. Materials and Methods Wistar Albino rats 8–10 weeks old were kept at 22±2ºC and 12 hours light and 12 hours dark cycles and were fed a normal diet and tap water without any restrictions. Under anesthesia, the rats were incised in the midline between T5 and T12 verte- bras, and the paravertebral muscles were pushed aside to expose the laminas. Later, at T7-T8-T9 vertebras, laminectomy was performed and a steel rod 3 mm in diameter and 10 g in weight was dropped from 10 cm to create a spinal cord injury.8 The control group was given the same dose of saline. Twenty Wistar Albino rats were divided into 2 groups with 10 in each: (1) Control Group (no trauma was induced in these rats. Only placebo saline was applied). (2) SCI Group (the rats in this group were traumatized as described above. Only placebo saline was administered to the rats). The rats were decapitated, and spinal tissue was processed for malondialdehyde (MDA), glutathi- one (GSH), and myeloperoxidase (MPO) and also for routine light microscopic tissue processing. The spinal cord was stored in 10% formaldehyde for histological examination and fixed for 24 hours. Hematoxylin-eosin staining and immunohistoche mical staining with VEGF and APAF-1 were per- formed. Biochemical Analysis Urinary bladder samples were homogenized with super cold 150 mM KCl for the assurance of MDA and GSH levels. The MDA levels were tested for the products of lipid peroxidation, and the out- comes are expressed as nmol MDA/g tissue. GSH was resolved by a spectrophotometric technique in light of the utilization of Ellman’s reagent, and the outcomes were expressed as μmol GSH/g tissue.9 Measurement of MPO Activity The MPO activity levels were measured using the method described by Hillegass et al.10 Urinary bladder tissue specimens were homogenized in 50 mM potassium phosphate buffer with a pH of 6.0 and centrifuged at 41,400 g for 10 minutes. The pellets were then suspended in 50 mM PB contain- ing 0.5% hexadecyl trimethyl-ammonium bromide. After 3 freeze and defrost cycles, with sonication between cycles, the samples were centrifuged at 41,400 g for 10 minutes. Aliquots (0.3 mL) were added to 2.3 mL of the response mixture contain- ing 50 mM PB, o-dianisidine, and 20 mM H2O2 solution. One unit of enzyme action was charac terized as the measure of MPO presence that caused an adjustment in absorbance, estimated at 460 nm for 3 minutes. MPO action was expressed as µ/g tissue. Immunohistochemical Analysis An antigen-retrieval process was performed in citrate buffer solution (pH 6.0) 2 times: first for 138 Analytical and Quantitative Cytopathology and Histopathology® Yariş and Deveci
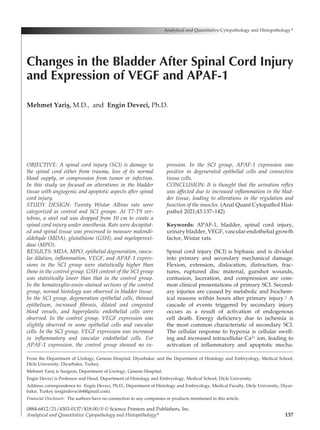
- 3. 8 minutes and then for 6 minutes in a microwave oven at 700 W. They were allowed to cool to room temperature for 30 minutes and washed in distilled water for 5 minutes twice. Endogenous peroxidase activity was blocked in 0.1% hydrogen peroxide for 15 minutes. Ultra V block (Histostain-Plus Kit, Invitrogen, Carlsbad, California, USA) was ap- plied for 10 minutes prior to the application of the primary antibodies VEGF and APAF-1 over- night. The secondary antibody (Histostain-Plus Kit) was applied for 20 minutes. Then the slides were exposed to streptavidin-peroxidase for 20 minutes. Diaminobenzidine (DAB, Invitrogen) was used as a chromogen. Control slides were prepared as mentioned above but omitting the primary antibod- ies. After counterstaining with hematoxylin, wash- ing in tap water for 3 minutes and in distilled water for 2×3 min, the slides were mounted.11 Statistical Analysis The data were recorded as arithmetic mean± standard deviation with mean rank value. Sta- tistical analysis was done using the IBM SPSS 25.0 software (IBM SPSS Statistics for Windows, Version 25.0, Released 2017, IBM Corp., Armonk, New York, USA). Kruskal-Wallis test was used for multiple comparisons. Mann-Whitney U tests were used for within-group comparisons. P<0.05 was used as the significance level. Results Statistical analyses of biochemical, histopathologi- cal, and immunohistochemical scoring are shown in Table I. In terms of MDA, MPO, epithelial de generation, vascular dilation, inflammation, VEGF, and APAF-1 expression, there was an increase in values in the SCI group as compared to the con- trol group, and this increase was statistically sig nificant. Only GSH content was decreased in the SCI group as compared to the control group, and the decrease was statistically significant. A graphi- cal illustration of Table I is shown in Figure 1. Histopathological and immunohistochemical staining is shown in Figure 1. Transitional epithe- lial cells in the control group sections were poly- gonal in shape and were regularly located. The connective tissue cells and fibers were unevenly distributed, and the circular muscle fibers were free. Blood vessels showed mild congestion, and endothelial cells were seen in a fusiform structure (Figure 1A). In the SCI group, degeneration of cells in the transitional epithelial layer, thinning of the epithelium, increase in fibrotic tissue in connec- tive tissue, mild deterioration in muscle tissue, Volume 43, Number 3/June 2021 139 Changes in the Bladder After Spinal Cord Injury Table I Biochemical (MDA, GSH, and MPO) and Histopathological (Epithelial Degeneration, Vascular Dilation, Inflammation, Expression Levels) of Control and Spinal Cord Injury Groups Mann-Whitney Mean Kruskal-Wallis U test Parameter Group N Mean±SD rank test value (p<0.05) MDA (1) Control 10 32.51±3.93 5.50 14.29 (2) (2) SCI 10 56.80±4.13 15.50 p=0.001 (1) GSH (1) Control 10 1.67±0.15 15.50 14.29 (2) (2) SCI 10 0.75±0.13 5.50 p=0.001 (1) MPO (1) Control 10 4.75±0.72 5.50 14.29 (2) (2) SCI 10 7.87±0.74 15.50 p=0.001 (1) Epithelial degeneration (1) Control 10 0.80±0.63 5.50 15.25 (2) (2) SCI 10 3.60±0.52 15.50 p=0.001 (1) Vascular dilation (1) Control 10 1.00±0.67 5.50 15.22 (2) (2) SCI 10 3.40±0.52 15.50 p=0.001 (1) Inflammation (1) Control 10 1.10±0.57 5.60 14.82 (2) (2) SCI 10 3.20±0.63 15.40 p=0.001 (1) VEGF expression (1) Control 10 1.70±0.48 6.55 10.53 (2) (2) SCI 10 2.80±0.63 14.45 p=0.001 (1) APAF-1 expression (1) Control 10 1.00±0.67 5.70 13.90 (2) (2) SCI 10 3.10±0.74 15.30 p=0.001 (1) SD = standard deviation.
- 4. excessive dilation and congestion in blood vessels, and hyperplasia in endothelial cells were observed (Figure 1B). In the immunohistochemical exam- ination, VEGF expression was positive in some epithelial cells, and small blood vessel endothelial cells, macrophage in connective tissue, and plasma cells were observed in the control group (Figure 1C). In the SCI group, increased VEGF expression was observed in inflammatory cells and hyper- plastic endothelial cells in dilated blood vessels along with epithelial degeneration and connective tissue inflammation (Figure 1D). Negative APAF- 140 Analytical and Quantitative Cytopathology and Histopathology® Yariş and Deveci Figure 1 (A) Control group: polygonal cell epithelium, connective tissue, and muscle cells in fusiform appearance (H-E staining). (B) Trauma group: degeneration and thinning of cells in the transitional epithelial layer, increase in fibrotic tissue in connective tissue, mild deterioration in muscle tissue, dilation and congestion in blood vessels, hyperplasia in endothelial cells (H-E staining). (C) Control group: positive VEGF expression in some epithelial cells, small blood vessel endothelial cells, macrophage in connective tissue (VEGF immunostaining). (D) Trauma group: an increase in VEGF expression in inflammatory cells and hyperplastic endothelial cells in dilated blood vessels (VEGF immunostaining). (E) Control group: no APAF-1 expression was observed (APAF-1 immunostaining). (F) Trauma group: APAF-1 was expressed in epithelial tissue, inflammatory cells, and blood vessels (APAF-1 immunostaining).
- 5. 1 expression in epithelial cells, connective tissue, and muscle cells was observed in the control group (Figure 1E). In the SCI group, APAF-1 expression was positive in pyknotic nuclei due to epithelial degeneration, and APAF-1 expression in inflam matory cells in the connective tissue area and en- dothelial and muscle cells showed a positive reac- tion (Figure 1F). Discussion One of the important functions in the urinary tract is the storage and excretion of urine. The urina- tion reflex is mediated by a bulbospinal pathway through the pontine voiding centers (Barrington nuclei) in the rostral brainstem.12 Urination occurs by the association of autonomic and somatic path- ways within the lumbosacral cord.13 Disruption of the pathways between the pontine voiding center and the sacral spinal cord in rats was considered a model of spinal cord injury. Spinal cord injury is a clinical condition that heavily affects patient quality of life, morbidity, and mortality. Incidence of SCI in the USA is annually 17,730 cases, with more than 291,000 affected individuals.14 SCI is also one of the most common causes of neuro- genic bladder that leads to loss of bladder func- tion.15 Depending on the severity, extent, and level of injury, neurogenic bladder may have low or hyper detrusor activity. The pathophysiology of SCI is a highly complex process with neurolog- ical lesions, diseases, and bladder and sphincter injuries.16 A study by Compérat et al showed that histopathological changes occur in neurogenic bladder.17 They showed that inflammatory infil- tration, edema, and fibrosis of the bladder wall were observed. Janzen et al recorded histological changes such as severe fibrosis in the lamina pro- pria and muscularis, hyalinization in the wall, dis- array of smooth muscle cells with leiomyomatous- like hyperplasia, and chronic inflammatory infil- trates in neurogenic bladder.18 Our histopatholog- ical findings of degeneration of cells in the transi- tional epithelial layer, thinning of the epithelium, increase in fibrotic tissue in connective tissue, mild deterioration in muscle tissue, excessive dilation and con gestion in blood vessels, and hyperplasia in endothelial cells were observed (Figure 1B). It is thought that urine storage, muscle reflex, and functional functions may be altered in the bladder due to cellular degeneration and muscle disorgani- zation. Vascular endothelial growth factor (VEGF) is a potent angiogenic factor expressed in angiogenesis and progression of various tumor types. Aposto- lidis et al19 studied neurogenic detrusor overactiv- ity and showed that VEGF expression was weak. They stated that more studies are needed to in- vestigate vascular changes with levels of bladder overactivity. Another study on idiopathic over- active bladder urothelial cells during stretch was performed and revealed that stretching of an over- active bladder increased the expression of mRNA for VEGF by 1.5-fold, 1.5-fold, and 3.5-fold as com- pared with an unstretched overactive bladder, sug- gesting that these findings may contribute to the understanding of overactive bladder.20 Herrera et al21 measured the level of VEGF as a potential in- terventional therapy for spinal cord injury by west- ern blot analysis. They found significant decrease in the levels of VEGF and other VEGF isoforms at the lesion epicenter 1 day after injury. Chen et al22 examined VEGF signaling pathway on spinal cord injury in rats. Their results showed that the con- trol and sham groups had lowest VEGF expres- sion by immunohistochemistry. In our study, after trauma, increased VEGF expression was observed in dilated blood vessels and inflamed cells, as well as in hyperplastic endothelial cells, with epithelial cell degeneration and connective tissue inflamma- tion. It induced angiogenesis (Figure 1D). APAF1 is the structural core of the apoptosome which takes places in the intrinsic or mitochon- drial pathway of apoptosis. Emery et al examined spinal cords of 15 patients who died between 3 hours and 2 months after a traumatic SCI. They found that apoptosis occurs in the spinal cord where injury was developed by caspase 3 immu- nostaining and other histological staining.23 Casha et al24 conducted an SCI experiment on rats and showed axonal degeneration after SCI. The au- thors correlated this finding with oligodendroglial apoptosis by confirming with FAS and p75 ex pression analysis. In a study of SCI, caspase-8 and caspase-9 expression level was elevated 6-hours after SCI, showing apoptosis and neuronal death. They also analyzed caspase-3 expression, stating that caspase-3 was expressed first at 24 hours af- ter SCI.25 After trauma, pyknosis in the nuclei as a result of epithelial degeneration, increase in in flammatory cells, hyperplasia in endothelial cells, and change in muscle cells caused an increase in APAF-1 reaction and prolongation of the apoptotic process (Figure 1F). In conclusion, spinal cord injury causes im- Volume 43, Number 3/June 2021 141 Changes in the Bladder After Spinal Cord Injury
- 6. paired bladder activity with degenerative changes in the bladder epithelium, inducing the apoptotic process. SCIs also disrupt blood vessel organiza- tion and increased inflammation in connective tissue, promoting angiogenesis. We suggest that increased inflammation in the bladder can signifi- cantly affect the urination reflex, causing changes in the regulation and function of the muscles. References 1. Donovan WH: Donald Munro Lecture. Spinal cord injury-- Past, present, and future. J Spinal Cord Med 2007;30(2):85- 100 2. Lifshutz J, Colohan A: A brief history of therapy for trau matic spinal cord injury. Neurosurg Focus 2004;16(1):E5 3. De Groat WC: Nervous control of the urinary bladder of the cat. Brain Res 1975;87(2-3):201-211 4. Leippold T, Reitz A, Schurch B: Botulinum toxin as a new therapy option for voiding disorders: Current state of the art. Eur Urol 2003;44(2):165-174 5. Weld KJ, Graney MJ, Dmochowski RR: Differences in blad- der compliance with time and associations of bladder man- agement with compliance in spinal cord injured patients. J Urol 2000;163(4):1228-1233 6. Tooke K, Girard B, Vizzard MA: Functional effects of block- ing VEGF/VEGFR2 signaling in the rat urinary bladder in acute and chronic CYP-induced cystitis. Am J Physiol Renal Physiol 2019;317(7):F43-F51 7. Jia YF, Gao HL, Ma LJ, Li J: Effect of nimodipine on rat spinal cord injury. Genet Mol Res 2015;14(1):1269-1276 8. Allen AR: Surgery of experimental lesion of spinal cord equivalent to crush injury of fracture dislocation of spinal column: A preliminary report. JAMA 1911;LVII(11):878-880 9. del Rayo Garrido M, Silva-García R, García E, Martiñón S, Morales M, Mestre H, Flores-Domínguez C, Flores A, Ibarra A: Therapeutic window for combination therapy of A91 peptide and glutathione allows delayed treatment after spinal cord injury. Basic Clin Pharmacol Toxicol 2013;112(5): 314-318 10. Hillegass LM, Griswold DE, Brickson B, Albrightson- Winslow C: Assessment of myeloperoxidase activity in whole rat kidney. J Pharmacol Methods 1990;24(4):285-295 11. Özevren H, I ∙ rtegün S, Deveci E, Aşır F, Pektanç G, Deveci Ş: Ganoderma lucidum protects rat brain tissue against trau- ma-induced oxidative stress. Korean J Neurotrauma 2017; 13(2):76-84 12. Cheng CL, de Groat WC: The role of capsaicin-sensitive afferent fibers in the lower urinary tract dysfunction in- duced by chronic spinal cord injury in rats. Exp Neurol 2004;187(2):445-454 13. Chien CT, Yu HJ, Lin TB, Chen CF: Neural mechanisms of impaired micturition reflex in rats with acute partial bladder outlet obstruction. Neuroscience 2000;96(1):221-230 14. Jain NB, Ayers GD, Peterson EN, Harris MB, Morse L, O’Connor KC, Garshick E: Traumatic spinal cord injury in the United States, 1993-2012. JAMA 2015;313(22):2236-2243 15. Manack A, Motsko SP, Haag-Molkenteller C, Dmochowski RR, Goehring EL Jr: Nguyen-Khoa BA, Jones JK: Epide- miology and healthcare utilization of neurogenic bladder patients in a US claims database. Neurourol Urodyn 2011; 30(3):395-401 16. Jeong SJ, Cho SY, Oh SJ: Spinal cord/brain injury and the neurogenic bladder. Urol Clin North Am 2010;37(4):537-546 17. Compérat E, Reitz A, Delcourt A, Capron F, Denys P, Chartier-Kastler E: Histologic features in the urinary blad- der wall affected from neurogenic overactivity--A compari- son of inflammation, oedema and fibrosis with and without injection of botulinum toxin type A. Eur Urol 2006;50(5): 1058-1064 18. Janzen J, Soni BM: Microscopic findings in a neurogenic bladder caused by myelomeningocele. Spinal Cord 2005; 43(1):65-66 19. Apostolidis AN, Yiangou Y, Brady CM, Ford AP, Baecker PA, Jacques TS, Freeman A, Fowler CJ, Anand P: Endothe- lial nitric oxide synthase expression in neurogenic urinary bladders treated with intravesical resiniferatoxin. BJU Int 2004;93(3):336-340 20. Christiaansen CE, Sun Y, Hsu YC, Chai TC: Alterations in expression of HIF-1α, HIF-2α, and VEGF by idiopathic overactive bladder urothelial cells during stretch suggest role for hypoxia. Urology 2011;77(5):1266.e1267-1211 21. Herrera JJ, Nesic O, Narayana PA: Reduced vascular endo- thelial growth factor expression in contusive spinal cord injury. J Neurotrauma 2009;26(7):995-1003 22. Chen H, Li J, Liang S, Lin B, Peng Q, Zhao P, Cui J, Rao Y: Effect of hypoxia‑inducible factor‑1/vascular endothelial growth factor signaling pathway on spinal cord injury in rats. Exp Ther Med 2017;13(3):861-866 23. Emery E, Aldana P, Bunge MB, Puckett W, Srinivasan A, Keane RW, Bethea J, Levi AD: Apoptosis after traumatic human spinal cord injury. J Neurosurg 1998;89(6):911-920 24. Casha S, Yu WR, Fehlings MG: Oligodendroglial apoptosis occurs along degenerating axons and is associated with FAS and p75 expression following spinal cord injury in the rat. Neuroscience 2001;103(1):203-218 25. Keane RW, Kraydieh S, Lotocki G, Bethea JR, Krajewski S, Reed JC, Dietrich WD: Apoptotic and anti-apoptotic mech- anisms following spinal cord injury. J Neuropathol Exp Neurol 2001;60(5):422-429 142 Analytical and Quantitative Cytopathology and Histopathology® Yariş and Deveci