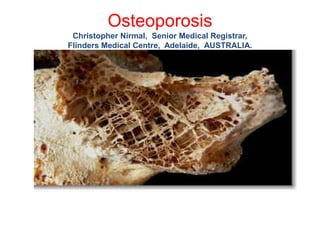
2. Definition
• Osteoporosis is a complex skeletal disease
characterised by low bone density and micro-
architectural defects in bone tissue, resulting in
increased bone fragility and susceptibility to
fracture
3. Introduction
• Osteoporosis is a silent disease
• The condition is under recognised and the affected are under treated
• Osteoporotic fractures (fragility fractures, low-trauma fractures) are those
occurring from a fall from a standing height or less, without major trauma.
• Vertebral compression fractures are the most common type of osteoporotic
fracture.
• They often occur at the midthoracic (T7-T8) spine and the thoracolumbar
junction (T12-L1).
• Fractures may result in significant back pain, limited physical functioning and
activities of daily living.
• Osteoporotic fracture is an important risk factor for subsequent fracture.
4. Epidemiology
(International Osteoporosis Foundation)
200 million people worldwide are affected by osteoporosis
30% of all post menopausal women have osteoporosis in USA and
Europe.
40% of women and 15-30% of men with osteoporosis will sustain
one or more fragility fractures in their lifetime
Number of fractures occuring worldwide each year will increase
from1.66 million to 6.26 million by 2050
Initial fracture is a major risk factor for a new fracture
5. Osteoporosis Australia
• 4.74 million Australians over 50 have osteoporosis or poor bone
health.
• There is 1 fracture every 3.6 minutes in Australia related to
osteoporosis or osteopenia (2013). By 2022 there will be 1 fracture
every 2.9 minutes.
• 144,000 fractures occured due to osteoporosis or osteopenia in 2013.
• Over the next 10 years, the total cost of osteoporosis and associated
fractures is estimated to be $33.6 billion.
6. Pathophysiology
Bone is an active tissue that constantly remodels in response to mechanical
stresses and hormonal changes.
By transmitting signals to osteoclasts and osteoblasts on the bone’s
surface, osteocytes play a principal role in the initiation of bone remodelling.
Osteoclasts resorb bone matrix by first creating a resorption pit.
They end their function with apoptosis followed by
coupling signals sent to osteoblasts.
Osteoblasts then synthesise bone matrix, which undergoes mineralisation.
7.
8. Bone remodelling
Bone remodelling is regulated by various cytokines
interleukins 1, 6, and 11,
colony-stimulating factors, and
calcitrophic hormones such as PTH, 1,25-dihydroxy vitamin D,
calcitonin, and oestrogen.
Members of the TNF and TNF-receptor superfamily,
receptor activator of nuclear factor- kappa B (RANK), RANK ligand
(RANKL), and osteoprotegerin (OPG),
play an essential role in osteoclastic bone resorption in
postmenopausal osteoporosis.
9. Screening
Appropriate history
Physical examination
Standard biochemical and haematological studies
• Biochemistry profile (especially calcium, phosphorous, albumin, total protein,
creatinine, liver enzymes including alkaline phosphatase, electrolytes).
25-hydroxyvitamin D (25[OH]D).
Complete blood count (CBC).
Measurement of Bone Mineral Density
10. Factors associated with fractures or low BMD in
post menopausal women
• Increasing age
• Low body weight
• Personal h/o fracture
• Family h/o osteoporotic fracture
• Excessive alcohol (> 2 drinks per day) caffeine and tobacco use
• H/o falls
• Low level of physical activity
• Low vitamin D or calcium intake
• Use of certain medications / presence of certain medical conditions.
15. Risk factor screening
• FRAX (Fracture Risk Assessment Tool) introduced by
WHO task force – estimates the 10 year probability of
hip fracture or major osteoporotic fractures combined
• FRAX can provide guidance for both BMD testing and
initiation of treatment
• FRAX – validated in 40 cohorts (over 1 million patient
years)
16.
17.
18.
19.
20.
21. Tests for Bone density
DEXA (dual energy xray absorptiometry)
most commonly used
QCT (quantitative computed tomography)
QUS (quantitative ultrasound)
RA (radiographic absorptiometry)
22. Bone strength
• Bone strength determined by BMD and other properties (bone
quality)
• Non BMD determinants of bone strength:
• Bone turnover
• Architecture
• Microarchitecture
• Matrix properties
• Bone turnover: markers used
• High resolution peripheral quantitative CT (HR-pQCT) and
• Micro-MRI : used in research
23. BMD testing (DXA)
• Widely available clinical tool to : diagnose osteoporosis
• predict fracture risk
• monitor response to therapy
• Strong correlation between mechanical strength and BMD
• Strong relationship between fracture risk and BMD
• WHO criteria for diagnosis of osteoporosis are based on reference data
obtained by DXA
• FRAX uses femoral neck BMD
• Relationship between decreased fracture risk with drug therapy and
increase in BMD measured byDXA
24. Candidates for BMD testing
Women 65 years or older
Post menopausal women younger than 65 with clinical risk factors for
fracture
Men with clinical manifestations of low bone mass:
Radiographic osteopenia
Low trauma fractures
Loss of more than 1.5 inches in height
With risk factors for fracture:
Drug therapy
Endocrinological
Malabsorption
25. T and Z scores
DEXA scores are reported as "T-scores" and "Z-scores."
The T-score is a comparison of a person's bone density with that of a
healthy 30 year old of the same sex. (Normal score – within 1 SD)
The Z-score is a comparison of a person's bone density with that of an
average person of the same age and sex.
Adjustment for ethnicity/race should be used in the following
Premenopausal women
Men < 50 yrs
Children
26. WHO Definitions of Osteoporosis
Normal: Bone density is within 1 SD (+1 or -1) of the young adult mean.
Low bone mass (osteopenia): Bone density is 1 to 2.5 SDs below the young
adult mean (-1 to -2.5 SD).
Osteoporosis: Bone density is 2.5 SDs or more below the young adult mean
(less than -2.5 SD).
Severe (established) osteoporosis: Bone density is more than 2.5 SDs below
the young adult mean and one or more broken bones (osteoporotic
fractures)
Z score: -2.0 SD or lower: below expected range for age
> -2.0 SD: within expected range for age
27. Skeletal site to measure
• WHO criteria:
• Lowest T score of lumbar spine (L1 to L4)
• Lowest score of femoral neck or proximal femur
DXA of Hip: best site for diagnosis
DXA of Lumbar spine: Best site to monitor
-1SD equals a 10 to 12% decrease in bone density
Risk for a fracture increases by 50 to 100% for every SD below the
young normal standard
28.
29.
30. • BTM and # risk relationship- not validated
• BTM – Not widely used (due to assay variability and
biologic variability)
• Diurnal variation in bone turnover: peaks at 6am / nadirs at 6pm
• Low BMI and smoking increase bone turnover
• BTMs increase during ovulation and decrease with use of OCP
• Recent food consumption decreases BTM
• Exercise and physical activity decrease BTM
• BTMs are increased for up to 4 months after a #
31. Aims of management
Identify patients at increased risk of fracture
To assess that risk accurately
To reduce the risk of fracture
To improve the patient’s perception of that risk
To give advice to aid understanding of the disease, the
aims of therapy and the choice of therapy
32. Whom to treat?
• Post-menopausal women:
• T score <-2.5 (osteoporotic)
• (or) Fragility fracture
• (or) T score -1.0 to -2.5 (osteopenic) -High risk
• (Low risk osteopenic pts.- not enough data available
• Suggested- modification of risk factors / Vit D and Calcium replete)
• Risk calculated using FRAX tool
33. Men:
Not having symptomatic hypogonadism (or) in hypogonadal men
in whom testosterone is contraindicated
T score <-2.5 (osteoporotic)
(or) Fragility fractures
(or) T score -1.0 to -2.5 (osteopenic)
Low risk osteopenic: modify risk factors / Vit D & Calcium replete
34. • People with special circumstances
• Patients on glucocorticoid therapy
• Women on Aromatase inhibitors for breast ca
• Men with prostate ca having undergone antiandrogen therapy.
35. Lifestyle measures
• Adequate calcium : total daily intake of 1000mg in adults
• 1300mg in women > 50 and men >70
• and Vitamin D (to maintain a 25 hydroxy vit D conc. of 75 nmol/l or more)
• 800 to 1000 units per day
• Absolute benefit in fracture prevention for non-institutionalised individuals is
low.
• Calcium supplements increase risk of renal calculi / abd bloating /
constipation
• High dose Vitamin D increases risk of falls in elderly adults (>70 yrs)
• 60,000 U per month vs. 24,000 U per month
• Higher dose had increased falls (p= 0.048) - JAMA Jan 2016
36. • Exercise (atleast for 30 mts thrice weekly)
• Weight bearing aerobic exercises (mod to high impact) benefit BMD
(Jogging, tennis, volleyball, stair climbing & step aerobics)
• Exercise for preventing falls: moderate to high intensity balance
training.
• Cessation of smoking
• Cutting down on alcohol.
37.
38. Measures to reduce falls
• Improving vision when possible
• Review of medication
• Assessing household risks
• Providing aids for daily living
• Promoting exercise to maintain mobility and strengthen quadriceps
• Minimising periods of immobilisation
40. Bisphosphonates
• Alendronate / Risedronate / Zoledronate
• Shown to increase bone mass and reduce both vertebral and hip fractures
• Oral Bisphosphonates – first line
• IV Zoledronic acid – for patients intolerant to oral (GI side effects)
• Upper GI: Osophagitis / Gastric ulcer / Oesophageal ca, (RR 1.30)
• Flu like symptoms (I/V Bisphos)
• Hypocalcaemia
• Musculoskeletal pain
• Atrial fibrillation (HORIZON trial) 1.3 vs. 0.5%
• MRONJ
• AFF
• (Not recommended Cr.Cl < 30 (Risedronate) <35 (Alendronate / Zoledronate)
41. Alendronate
• Increased spine BMD by 9% and hip BMD by 6% over 3 years / reduces
bone turnover markers by 50–70%
Lieberman et al, NEJM, 1995
• The Vertebral Fracture Arm of the Fracture Intervention Trial (FIT)
• 2027 post menopausal women with prevalent vertebral fractures on
alendronate 3 yrs
• Incidence of new fractures reduced by ~50% compared with
• Placebo
• Black et al, Lancet, 1996
• Non-vertebral and hip fractures were significantly reduced
• (~33%) in those with a hip BMD T score below −2.5
• Cummings et al, JAMA, 1998
42. Risedronate
• Increased spine BMD by 4–5% and hip BMD by 2–4% versus
placebo over 3 years
• Reduced bone turnover markers by 40–60%
• Harris et al, JAMA, 1998
•
• In 2 three year studies of 3600 women with prevalent vertebral
fractures, risedronate reduced vertebral fractures by 40–50%
• Harris et al, JAMA, 1999
• Reginster et al, Osteoporos Int, 2000
• Osteoporotic non-vertebral fractures were reduced by ~33%
43. Zoledronic acid
• Most potent bisphosphonate currently available
• Health Outcomes and Reduced Incidence with ZoledronicAcid
Once Yearly (HORIZON)
• Large-scale phase III trials of 5 mg given annually to evaluate the
antifracture effect of intravenous zoledronate reported in 2007
• 7765 women, mean age 73
• 3 yrs
• Vertebral fractures reduced by 70%
• Hip fractures reduced by 41%
• Non vertebral fractures reduced by 25%
• Black et al, NEJM, May 3, 2007
46. Bis-phossy jaw, ONJ, BRONJ, MRONJ
Likely pathogenesis of MRONJ:
Related to suppression of bone remodelling and antiangiogenic effects
of the medications.
Risk: 1 in 10,000 to 1 in 100,000 patient years (oral Bisphosphonates) in OP
Occurs with:
• Bisphosphonates ( I/V > oral )
• Denosumab
• Tyrosine kinase inhibitors
• Bevacizumab
• Mandible > Maxilla
47. • Risk factors:
• In patients with a long term use of any of the medications
mentioned
• Receiving frequent dosing (cancer patients)
• High potency agents
• Recent dental surgery
• Dental or periodontal disease
• Concurrent bony mets or multiple myeloma
• Prevention:
48. • Treatment:
• Stop the culprit medication
• Antiseptic mouth rinses
• Systemic antibiotics
• Surgical debridement / resection
• Hyperbaric oxygen therapy
• Low level laser therapy
• Teriparatide
• Pentoxifylline + VitaminE
• Autologous platelets as an adjunct to surgery
49. Atypical femoral fractures
• Occurs in the proximal third of the femur, typically subtrochanteric
• May be unilateral or bilateral.
• Can also occur more inferiorly to the level of the supracondylar
region.
• Occurs with minimal to no trauma
• Risk: 3.2 to 50 per 100,000 patient years
• An atypical femoral fracture is a diagnosis of exclusion
• not be spiral or comminuted
• not be femoral neck or intertrochanteric
• no evidence of malignant bone tumour (primary or metastatic)
• not be periprosthetic
52. • SERM: Raloxifene
• Need for breast cancer prophylaxis
• Inhibits bone resorption and reduces risk of vertebral fracture
• Increase in thromboembolic events
• Increase in hot flushes
• (Tamoxifen: 50% risk reduction of breast ca. Vs. 38% with Raloxifene over 7 years)
53. • Denosumab:
• RANKL ( receptor activator of nuclear factor kappa-B ligand ) is essential
for the function of bone resorbing osteoclasts.
• Denosumab is a humanised monoclonal ab. against RANKL that reduces
osteoclastogenesis.
• Shown to improve BMD / reduce incidence of vertebral and hip fractures
• Initial therapy in patients at high risk for #
• Intolerant or unresponsive to other agents
• Effective in patients with CKD
54.
55. • FREEDOM trial (Fracture reduction evaluation of Denosumab in
osteoporosis)
• 7868 women 60 to 90 years of age
• 6o mg S/C 6 monthly Denosumab vs. Placebo for 3 years
• Decrease in V.Fractures 68%
• Non V.Fractures 40%
• Hip fractures 20%
56. Denosumab:
• Also 1. Reduces risk of skeletal complications in patients with
bony metastasis
• 2. Delays time to first bony metastasis in castrate resistant
prostate ca / breast ca / NSCLC
• In patients with a PSA doubling < 6 months, median time to first bony
met was 25.9 months with Denosumab vs. 18.7 months with
placebo.
Dose: 120 mg S/C 4 weekly
More effective than Zoledronic acid.
57. • Side effects:
• Hypocalcaemia (esp. In CKD) Adequate Calcium and VitD
• Musculoskeletal pain
• Dyslipidemia
• Eczema
• Occasionally: ONJ
• Atypical fractures
58. • Teriparatide ( synthetic form of human parathyroid harmone):
• Only anabolic agent (stimulates bone formation)
• Intermittent dosing stimulates osteoblasts)
• Indicated in patients with severe osteoporosis
• Other therapies fail
• Reduces risk of vertebral and non vertebral fractures
• S/C injection : 20 mcg daily (max 18 months)
• Transient hypercalcemia / cramps / dizziness / headaches / nausea
• Bone sarcoma in rats (1 reported in humans out of 300,000 )
• .C/I : pre existing hypercalcaemia / malignancy / CKD / pr. hyperparathyroidism
• < 25 years / Paget’s disease / previous RT to bones.
59. • Combination (Denosumab + Teriparatide)
• DATA trial (Denosumab and Teriparatide administration) in
postmenopausal women with osteoporosis
• Combination increased BMD in femoral neck, total hip and lumbar
spine (compared to either drug as a single agent )
• Ideal for high risk fractures
• Calcitonin:
• Less popular choice
• Relatively modest effect on BMD and weak antifracture efficacy
60. • Oestrogen/Progestin:
• Oestrogens more potent than progestins in preventing bone loss
• Not considered as first line therapy
• Increased incidence of breast ca
• Coronary Artery Disease
• Venous thromboembolism
• Used for control of menopausal symptoms (<60 years of age)
• Combination of bisphosphonate and HRT may offer added benefit in
• women who continue to lose bone mass despite taking oestrogens (or)
• women who are on bisphosphonates and need oestrogens to control
• menopausal symptoms.
61. • Strontium ranelate:
• Modest anti resorptive effect / increase or have neutral effect on
bone mass
• Effective in reducing risk of vertebral fracture / lesser extent for non
vertebral
• For patients who cannot tolerate or unable to take bisphosphonates
• Increased risk of VTE / PE / MI
• Overestimation of BMD (due to uneven distribution / heavier
strontium cations absorbing more xrays than calcium.
62. • Efficacy of Strontium assessed in 2 randomised placebo controlled
trials with more than 6000 pts.
• 2 gms/ day
• SOTI (spinal osteoporosis therapeutic intervention)
• 41% reduction in new vertebral fractures
• TROPOS (treatment of peripheral osteoporosis)
• 16% reduction in non-vertebral fractures
63. Glucocorticoid induced osteoporosis
Glucocorticoids: Reduce intestinal calcium absorption
Reduce osteoblast function
Cause apoptosis of osteocytes
Cause hypercalciuria
Cause gonadal suppression
Indications for treatment
High risk men > 50 years & post menopausal women with a fragility
fracture (or) T score less the -1.0 given any dose of glucocorticoids for
> 3 months.
Low risk men > 50 years & post menopausal women with a T score less
than -1.0 given 7.5 mg daily of glucocorticoids for > 3 months.
Initial BMD plus yearly until steroids ceased.
64. • Bisphosphonates are effective first line agents in preventing and
treating GI osteoporosis (reduce apoptosis caused by steroids)
• Reduce relative risk of GI osteoporosis by 40%
• Data support using Alendronate, Risedronate or Zoledronic acid
• Teriparatide is more effective in reducing vertebral fractures in GI
osteoporosis. (considered second line)
65. Cancer therapy and the bones
• Breast cancer: Aromatase inhibitors (Anastrazole, Letrozole and
Exemestane) used in treatment cause profound decline in serum
oestradiol leading to bone loss.
• Baseline BMD is required
• Treatment with bisphosphonate or Denosumab in osteopenic /
osteoporotic pts.
• Tamoxifen stabilises or increases BMD
• Prostate cancer: Androgen deprivation therapy
• Reduced serum testosterone levels can lead to bone loss.
• Baseline BMD is required
• Treatment with bisphosphonates or Denosumab in osteopenic/
osteoporotic pts.
66. Bisphosphonates- for how long?
• Extension of FIT (Fracture Intervention Trial)
• FLEX( Fracture intervention trial Long term Extension)
• 1099 postmenopausal women who had been randomised to alendronate in FIT with a
mean of 5 years of prior alendronate treatment:
• randomised to alendronate vs. placebo for another 5 yrs.
• Conclusion: Continuation of alendronate for 10 years maintains bone health
• Discontinuation did not increase the risk of non-vertebral fracture or x-ray detected
vertebral fractures over the next 5 years.
• Risk of clinically diagnosed vertebral fractures significantly increased .
• Women at high risk of clinical vertebral fractures (very low BMD / existing v.
Fractures) may benefit beyond 5 years
67. Drug holiday
• If T score > 2.5 and no new fractures: Drug holiday
• If T score <2.5 and / or there are recent fractures: continue treatment
• Reassess: sooner for drugs with lower skeletal affinity
• 1 year for Risedronate
• 1-2 years for Alendronate
• 2-3 years for Zoledronate
• Restart if evidence of bone loss / fracture with minimal trauma
• The other options for patients at high risk:
• Denosumab
• Strontium ranelate.
68. • 54-year-old woman,
• menopause at age 51,
• lowest T-score –1.5,
• no risk factors,
• bisphosphonate therapy for 3 years.
• What next?
69. • Low risk of fracture:
• treatment is not needed.
• If a bisphosphonate has been prescribed, it
should be discontinued and not restarted
unless/until the patient meets treatment
guidelines
70. • 68-year-old woman,
• menopause at age 50,
• initial lowest T-score –2.3,
• parent with a hip fracture,
• bisphosphonate treatment for 5 years,
BMD stable over that time.
71. • Mild risk of fracture:
• treat with bisphosphonate for 3–5 years, then
stop.
• The ‘drug holiday’ can be continued until there
is significant loss of (or) the patient has a
fracture, whichever comes first.
72. • 72-year-old woman,
• menopause at age 48, lowest initial T-score –2.8,
• no risk factors,
• bisphosphonate therapy for 7 years,
• BMD increased over that time so lowest T-score
now is –2.3
73. • Moderate risk of fracture:
• treat with bisphosphonate for 5–10 years,
• offer a ‘drug holiday’ of 3–5 years (or} until there is
significant loss of BMD or the patient has a fracture,
whichever comes first
74. • 75-year-old woman,
• menopause at age 45,
• lowest initial T-score –3.6,
• rheumatoid arthritis requiring ongoing
corticosteroid therapy for 12 years,
• two vertebral fractures by vertebral fracture
assessment (VFA),
• treatment with bisphosphonate therapy for 10
years.
75. • High risk of fracture (fractures, corticosteroid therapy,
very low BMD):
• treat with bisphosphonate for 10 years,
• offer a ‘drug holiday’ of 1–2 years, until there is
significant loss of BMD (or) the patient has a fracture,
whichever comes first.
• A nonbisphosphonate treatment (e.g. raloxifene or
teriparatide) may be offered during the ‘holiday’ from
the bisphosphonate
76. Monitoring osteoporosis treatment
• Measure BMD at lumbar spine and hip
• 2 years after therapy begins (or)
• 1-2 years after therapy changes significantly
• Actual BMD values required
• Boneturnover markers are showing potential for monitoring
• Collage type 1 cross-linked C-telopeptide (CTX)
• Type 1 procollagen (N-terminal) (P1NP)
• If BMD response satisfactory- further measurements after 2 years
77. Emerging therapies
• PTHrP: Structurally homologous to Teriparatide
• Abaloparatide is a synthetic analogue of PTHrP
• BMD response is greater in spine and hip compared to Teriparatide
• Over 18 months: Incidence of spinal # reduced by 86% vs. 80%
• Non vertebral reduced by 43% vs 28%
• Reduction in degree of hypercalcemia
• Anti-sclerostin: Sclerostin is an osteoblast inhibiting glycoprotein
expressed primarily in osteoctyes.
• Inhibiting sclerostin increased bone mass and structure.
• Romosozumab is a monoclonal ab (Increases bone formation and
• reduces bone resorption)
78. • Romosozumab decreased vertebral # rates
• Further decrease following transition to Denosumab in the 2nd year in the
FRAME study (Fracture study in post menopausal women with
osteoporosis)
No significant reduction in non vertebral #.
Cathepsin K inhibitor: Odanacatib
Anti-resorptive once weekly oral medication
Inhibits resorption more than formation
Phase 3 trial stopped early : highly effectiv e with significant # reduction
and good safety profile
Slightly increased risk of stroke , hence discontinued.
79. References
• UpToDate
• New England Journal of Medicine
• Therapeutic Guidelines, Australia
• Osteoporosis, Australia
• International Osteoporosis Foundation