APPROACHES OF ILIUM, PUBIC SYMPHYSIS & SACROILLIAC JOINT
•Transferir como PPTX, PDF•
3 gostaram•146 visualizações

THIRD YEAR PG RESIDENT, M.S. ORTHOPAEDICS muscles of the thigh, Gluteus medius, Gluteus maximus, Tensor fascia lat, Anterior and posterior Illium approaches for grafting, Anterior approach to the iliac wing and SI joint. Anterior approach to the iliac wing and SI joint,

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (19)
Semelhante a APPROACHES OF ILIUM, PUBIC SYMPHYSIS & SACROILLIAC JOINT
Semelhante a APPROACHES OF ILIUM, PUBIC SYMPHYSIS & SACROILLIAC JOINT (20)
Último
Último (20)
APPROACHES OF ILIUM, PUBIC SYMPHYSIS & SACROILLIAC JOINT
- 1. APPROACHES OF ILIUM, PUBIC SYMPHYSIS & SACROILLIAC JOINT. DR.ARPAN CHAUDHARY
- 8. GRAFT Anterior iliac crest bone grafts are the most commonly used grafts in orthopaedic surgery. cortical or corticocancellous grafts can be taken from it. grafting in all parts of the body, including the spine. It also is possible to remove pieces of the iliac crest, including both cortices, for major bone reconstructions, especially in the head and neck. For posterior spinal fusion work on conditions such as scoliosis, the bone graft usually is taken from the posterior aspect of the iliac crest. . INDICATIONS : BONE GRAFT HARVEST : TRICORTICAL AUTOGRAFT : CANCELLOUS AUTOGRAFT : CORTICOCANCELLOUS AUTOGRAFT ANTERIOR ILIAC CREST BONE GRAFT
- 9. Position of the Patient Place the patient supine on the operating table. the graft usually is taken in conjunction with other procedures, the iliac crest should be draped as a separate unit. Place a small sandbag under the gluteal (cluneal) area of the side from which the graft will be taken to elevate the crest and rotate it internally, making it more accessible. LANDMARKS The subcutaneous anterior superior iliac spine, the most important landmark. Continue palpating along the crest of the ilium until its widest portion the iliac tubercle. The iliac tubercle marks the anterior portion of the ilium, the area containing the largest amount of cortical cancellous bone for graft material.
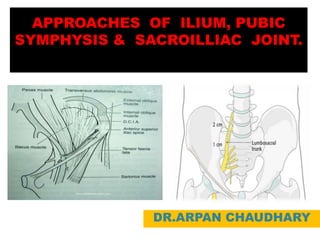
- 10. INTERNERVOUS PLANE Muscles either take origin from or insert onto the iliac crest, but do not cross it. Therefore, the crest offers a truly internervous plane. Identify the natural raphe between the fascia overlying iliac wing Fascia of external oblique anteriorly Fascia of gluteus medius posteriorly Incise directly on the iliac wing INCISION: Parallel the incision in line with the iliac crest Center incision based on type of graft required Tricortical (Smith-Robinson) graft Focus incision at least 2 cm posterior to ASIS Corticocancellous/cancellous bone graft Focus incision over iliac tubercle
- 11. SUPERFICIAL DISSECTION Deepen in line with skin incision down to iliac wing Do not stray anterior to the ASIS Bcz, Lateral femoral cutaneous nerve Course varies Typically, it runs 1 cm anterior to the ASIS underneath the inguinal ligament Inguinal ligament Takes origin off of ASIS. Do not inadvertently cut or detach the inguinal ligament, which can result in an inguinal hernia.
- 12. DEEP DISSECTION Subperiosteal dissection Using a Cobb elevator, subperiosteally dissect the abdominal musculature and the psoas off the inner table of the iliac wing. Using a Cobb elevator, subperiosteally dissect the gluteus medius and tensor fasciae latae off the outer table of the iliac wing Place Taylor retractors to protect the surrounding structures Closure Close in layers in the standard fashion A drain is typically not required
- 13. Other Avulsion fracture of ASIS Risk may be reduced by performing osteotomy at least 1 cm proximal to ASIS Inguinal ligament Takes origin off of ASIS. Do not inadvertently cut or detach the inguinal ligament, which can result in an inguinal hernia. Hazards Neural structures Lateral femoral cutaneous nerve lies approximately 1 cm distal to the ASIS. In a small percentage of patients may cross over the iliac wing Vascular Femoral artery and vein Rarely at risk, but may be injured if exposure strays anteriorly into the femoral triangle
- 14. OSTEOTOMIES Tricortical graft Make osteotomy at least 2 cm from the ASIS - This reduces risk of iatrogenic ASIS avulsion Make parallel osteotomies to ensure that the graft has parallel end plates - Measure the length and depth of graft required One-level and two-level grafts are typically obtained without difficulty There may be insufficient crest available for longer strut grafts Natural curvature of the iliac wing also may prohibit long strut grafts Corticocancellous graft Strips can be harvested using an osteotome Cancellous bone The iliac tubercle provides the largest supply of cancellous bone and can be accessed via a variety of methods
- 15. Posterior Approach to the Iliac Crest for Bone Graft. Indications: Fixation of disruption to the sacroiliac joint, : Fractures of the ilium adjacent to the sacroiliac joint, : Irrigation and débridement of infection to the area Taken during any posterior spine surgery that requires additional autogenous bone to supplement the area to be fused. The grafts also may be used as corticocancellous grafts for any part of the skeleton that needs fusion or refusion. Position of the Patient Prone Positioning Bolsters and padding in place to allow expansion of the chest and abdomen without restriction Isolation of the anus from the field with an isolation type of drape Radiolucent table used for fluoroscopic assistance is advised Landmarks Palpate the posterior superior iliac spine under the dimpling of the skin bove the buttock. The subcutaneous posterior part of the iliac crest also is palpable.
- 16. INTERNERVOUS PLANE: Muscles insert into or take origin from the iliac crest, but do not cross it. Therefore, the outer border of the iliac crest is truly an internervous plane. The gluteus medius, minimus, and maximus muscles take their origins from the outer surface of the ilium. The segmentally supplied paraspinal muscles take their origin from the iliac crest itself, as does the latissimus dorsi, which is supplied proximally by the long thoracic nerve. Thus, an incision into the iliac crest does not denervate muscles, even if it is not placed exactly on the outer lip of the crest. INCISION Make an 8-10 cm oblique incision, centered over the posterior superior iliac spine and in line with the iliac crest . If scoliosis surgery or lumbar surgery is being performed, the midline incision can be extended distally to the sacrum. Then, the skin and thick, fatty, subcutaneous layer can be retracted laterally. Using a Hibbs retractor, the flap should be dissected free from the underlying lumbodorsal fascia until the posterior superior iliac spine and crest can be palpated and seen.
- 17. Superficial Surgical Dissection The subcutaneous tissues should be dissected until the iliac crest is reached. In children, the iliac apophysis is white and quite visible; it may be incised or split in line With the iliac crest, using it as an avascular plane. In adults, the apophysis is ossified and fused to the crest; the incision lands directly on The crest itself. The Cobb elevator should be used to remove the apophysis or muscles from the iliac crest both medially and laterally, To bare the surface of the posterior portion of the crest. Dangers: Nerves The cluneal nerves cross the iliac crest. They can be avoided by placing the incision no more than 8 cm anterolateral to the posterior superior iliac spine.
- 18. DEEP SURGICAL DISSECTION: Strip the musculature completely off the posterior portion of the Lateral surface of the ilium so that a large enough graft can be obtained. Take care to stay in a subperiosteal plane while passing from the iliac crest to the outer cortex of the ilium. Proceeding 1.5 cm down the ilium in the area of the posterior superior spine, the elevated posterior gluteal line can be seen and felt; pass subperiosteally up over the line and then down its other side. Do not try by letting the line direct the incision outward from bone into muscle. A Taylor retractor will help the exposure by holding the muscles laterally. DANGERS: Nerves It is remotely possible that an osteotome will hit the sciatic nerve, which runs deep to the sciatic notch. However, if an imaginary line is drawn from the posterior superior iliac spine perpendicular to the operating table, and all work is performed cephalad to it, both the notch and the nerve will be avoided completely. If a larger graft is necessary, palpate the sciatic notch itself before taking the graft .
- 19. VESSLES The superior gluteal vessel, a branch of the internal iliac (hypogastric) artery, leaves the pelvis via the sciatic notch, staying against the bone and proximal to the piriformis muscle. If a graft is taken too close to the sciatic notch, the vessel may be cut and may retract into the pelvis. Nutrient vessels from the artery supply the iliac crest bone along the midportion of the anterior gluteal line, and the vessel may become an osseous bleeder as it enters bone via the nutrient foramen. To control bone bleeding, use bone wax on the raw cancellous surface of the pelvis after the graft has been removed. Bone Avoid the sciatic notch. Breaking through the thick portion of the bone that forms the notch disrupts the stability of the pelvis. Removal of bone from the false pelvis proximal to the notch does not cause loss of Stability.
- 20. How to Enlarge the Approach Local Measures Place a sharp-tipped, right-angled Taylor retractor into the bone to retract the gluteal muscles away from the bone and increase the exposure. To increase the exposure further, lengthen the iliac crest incision and strip more of the gluteal muscles from the outer cortex to avoid working through a “keyhole.” Extensile Measures This incision cannot be extended. It is designed specifically for removing bone for graft material from the posterior outer cortex of the ilium. Inner cortex also may be taken, but soft tissues should not be stripped off the anterior (deep) aspect of the ilium.
- 21. Anterior Approach to the Pubic Symphysis Indication: : Pubic symphysis disruption/diastasis : Fractures of the anterior pelvic ring including superior pubic rami This approach may be carried laterally (modified Stoppa approach) to expose the anterior ring extending to the sacral iliac joint. POSITIONING: Supine Foley catheter in place IN BLADDER Dangers Structures : Bladder Vessels : Superficial epigastric artery and vein Landmarks : Pubic symphysis and pubic tubercles Incision : 8-16 cm centered at the pubic symphysis In line with skin crease and about 1 cm above the pubic symphysis and superior rami
- 22. SUPERFICIAL DISSECTION No true internervous plane Subcutaneous tissue is incised in line with the incision uncovering the rectus sheath. Ligation of the superficial epigastric artery and vein as they run across the field from inferior to superior may be necessary. DEEP DISSECTION MIDLINE Care should be taken to maintain the rectus abdominis attachment if possible; this may mean you have to work under the rectus attachment to the ramus Often one side of the rectus insertion is avulsed in an anterior displaced pelvis disruption Retract the abdominis laterally and superiorly A layer of extraperitoneal fat may be present between the rectus abdominis and the bladder The posterior aspect of the superior rami and pubic symphysis can be accomplished digitally (preperitoneal space of Retzius) CLOSURE : Repair of the rectus abdominis and its sheath should be done separately Subcutaneous and skin closure accomplished in the normal fashion EXTENSILE MEASURES : Can be used in conjunction with the ilioinguinal approach
- 23. 1. Horizontal incision (“Pfannenstiel”) 2.Dissection of subcutaneous tissue Locate the linea alba and incise it longitudinally. Both bellies of the rectus abdominis muscle are gently retracted laterally 3. Exposure of the retrosymphyseal region Use your hand to bluntly dissect the retro symphyseal region. Use care to avoid injury to the urinary bladder or to the prostatic venous plexus.
- 24. 4.RETRACT THE RECTUS ABDOMINI Carefully elevate the remains of this disrupted rectus abdominis to allow exposure of the symphysis while maintaining as much distal fascial continuity as possible to avoid later hernia formation. 5.To elevate the recti insertions from the pubic body lateral to identify the obturator foramen. 6.INSERT REDUCTION FORCEP IF NEEDS 7.Once the symphysis is exposed, the PUBIC RAMI CAN BE IDENTIFIED laterally to the region of the iliopectineal (iliopubic) eminence. 9.CLOSURE
- 25. Posterior Approach to the Sacroiliac Joint It provides access to : The posterior ilium : Sacroiliac joint : Posterior surface of the sacrum Indications Fixation of disruption to the sacroiliac joint, Fractures of the Ilium adjacent to the sacroiliac joint, Irrigation and debridement of infection to the area. Positioning Prone. Bolsters and padding in place to allow expansion of the chest and abdomen without restriction. Isolation of the anus from the field with an isolation type of drape. Radiolucent table used for fluoroscopic assistance is advised. Dangers Structures Inferior gluteal nerve Superior gluteal nerve Sacral nerve roots (from screw fixation) Superior cluneal nerves Vessels Branches of the superior and inferior gluteal arteries are in danger and should be cauteriz
- 26. Landmarks : Posterior iliac crest and PSIS Incision : (8-12 cm centered 2-3 cm above and lateral to the PSIS) Incision for the posterior approach to the sacroiliac joint is vertical in nature from just above the PSIS distally about 10 cm. The incision can be extensile in nature along the iliac crest if necessary Superficial dissection : No true internervous plane Subcutaneous tissue is incised in line with the incision uncovering the fascia of the gluteus maximus and medius Incise the fascia of the maximus over the crest of the ilium Reflect the gluteus maximus subperiosteally downward and laterally (branches of the inferior gluteal artery may be present) This uncovers the gluteus medius and the piriformis emerging from the greater sciatic notch (superior gluteal nerve and artery emerging as well).
- 27. Deep Dissection : In trauma cases, the sacroiliac joint capsule may be disrupted and easily visualized; otherwise, it may need to be incised to visualize the reduction. The gluteus medius cannot be elevated far anteriorly because the neurovascular bundle to the muscle is present (superior gluteal nerve and artery) Deeper dissection involves incising the gluteus maximus fascia and subperiosteally elevating the maximus off of the ilium just lateral to the PSIS. The joint capsule of the sacroiliac joint, if not traumatically disrupted, may need to be incised for anatomical reduction of the joint surface. Extensile measures : The incision superiorly can be carried in a curving fashion along the crest of the ilium superiorly and anteriorly to uncover the wing of the ilium
- 28. Anterior approach to the iliac wing and SI joint: Sacroiliac joint dislocations Fractures of the ilium, even extending into the sacroiliac joint This approach enables direct visualization of the anterior and superior portions of the sacroiliac joint. Provides access to the : Iliac crest : The entire internal iliac fossa, : The most lateral sacral ala. This is limited by the L5 nerve root on the anterior aspect of the ala. POSITIONING Supine on OT table. DANGER The L5 and L4 nerve root (lumbosacral trunk) travels across the sacral ala and is 10-15 mm medial to the sacroiliac joint. Because of the proximity of this lumbosacral trunk, the surgeon must use care when working in this area.
- 29. SKIN INCISION An incision is made along the iliac crest. Be aware of the lateral femoral cutaneous nerve in the region of the ASIS. The incision can be extended intraoperatively depending on the necessary exposure. For fractures involving the posterior aspect of the ilium, or the sacroiliac joint, the exposure needs to be extended posteriorly almost to the table. SUPERFICIAL SURGICAL DISSECTION Divide the subcutaneous tissues in line with the skin incision in order to expose the fascia overlying the external oblique muscle The external oblique muscle is subperiosteally elevated from the iliac crest. With a small elevator, the iliac muscles are elevated using the same subperiosteal layer.
- 30. When elevating the iliacus muscle, bleeding from nutrient vessels can occur and should be stopped with bone wax. Continue with careful blunt dissection to the interior part of the SI joint medially to the pelvic ring. Proceed anteromedially at the pelvic rim as far as to where the iliopectineal eminence begins. The dissection is carried further medially onto the sacral ala. Move the Hohmann retractor medially carefully onto the sacral ala. Note the L5 nerve root traversing this region. Place a second Hohmann more anteriorly on the sacral ala. DEEP DISSECTION
- 31. Place an additional Hohmann anterior to the sacroiliac joint for additional exposure. Take care when placing this anterior retractor as it may injure the superior gluteal artery and nerve as they exit the greater sciatic notch. The sacroiliac joint is now exposed. Repair the aponeurosis of the external oblique muscle to the periosteum that was left intact lateral to the iliac crest. Close the subcutaneous tissues and skin in layers