PARANASAL SINUS AND NASOPHARYNX.pptx
•
1 gostou•95 visualizações

PARANASAL SINUS AND NASOPHARYNX.pptx

Recomendados
Recomendados
Mais conteúdo relacionado
Semelhante a PARANASAL SINUS AND NASOPHARYNX.pptx
Semelhante a PARANASAL SINUS AND NASOPHARYNX.pptx (20)
Mais de Cancer surgery By Royapettah Oncology Group
Mais de Cancer surgery By Royapettah Oncology Group (20)
Último
Último (20)
PARANASAL SINUS AND NASOPHARYNX.pptx
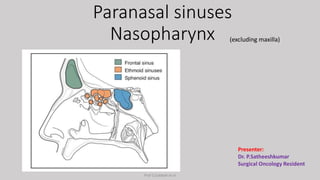
- 1. Paranasal sinuses Nasopharynx (excluding maxilla) Presenter: Dr. P.Satheeshkumar Surgical Oncology Resident Prof S.Subbiah et al
- 2. Incidence < 10% of head and neck cancer 0.5 per 100,000 people (annual incidence) • Tumors can occur at any age • 6th & 7th decades ( major presentation) • <20 years - Minor salivary gland tumors & Olfactory neuroblastoma • Male to Female ratio – 2:1 • {Occupational factors are excluded} Radiation therapy for esthesioneuroblastoma: rationale for elective neck irradiation. Head Neck. 2003 Jul;25(7):529-34. doi: 10.1002/hed.10247. PMID: 12808655. Prof S.Subbiah et al
- 3. Squamous Cell Carcinoma (+ variants) – MC neoplasm • Minor salivary gland tumors – 10% to 15%. • Lymphoma – 5% • Melanoma – 1% • Neuroendocrine carcinoma (rare) – 5% of malignant tumors, Ethmoid and nasal cavity region (late-stage disease). • Soft tissue and Bone sarcomas (Chondrosarcoma, Osteosarcoma and Ewing sarcoma) Histology Prof S.Subbiah et al
- 4. Etiological factors • Smoking – Sinonasal SCC. • First noted around High Wycombe by Acheson et al – High incidence of Adenocarcinoma (Ethmoids) • Wood dust, nickel, and possibly chemicals used in leather processing. • Dust filled environments (Baking, flour milling & shoe making) • High-risk Human papillomavirus (HPV) – 25% of patients with Sinonasal SCC (nonkeratinizing carcinomas) – favorable prognosis. Acheson ED, Adenocarcinoma of the nasal cavity and sinuses in England and Wales. Br J Ind Med. 1972;29(1):21-30. doi: 10.1136/oem.29.1.21. PMID: 5060244; Luce D, Leclerc A, Bégin D,Sinonasal cancer and occupational exposures: a pooled analysis of 12 case-control studies.2002 Mar;13(2):147-57. doi: 10.1023/a:1014350004255. PMID: 11936821. Prof S.Subbiah et al
- 5. Ethmoid sinus • Ethmoid sinuses (several air cells) – between the medial walls of the orbits and the lateral wall of the nasal cavity • Middle turbinate separates it into anterior and posterior ethmoid air cells. • Communicate with the nasal cavity (Middle meatus). Prof S.Subbiah et al
- 6. Ethmoid sinus • Lateral wall – Lamina papyracea. • Medial wall – Lateral wall of the nasal cavity. • Anterior ethmoidal artery • More vulnerable during endoscopic surgery • Running across anterior skull base posterior to the Suprabullar cell and frontal recess • Posterior ethmoidal artery • More protected running within bony roof ARTERIAL SUPPLY • Ophthalmic artery (Internal Carotid) • Ethmoidal A & Sphenopalatine A (External Carotid) VENOUS DRAINAGE Corresponding Venous system LYMPHATICS • Anterior cells – Submandibular nodes • Posterior cells – Retropharyngeal nodes Turri-Zanoni M, Arosio AD,Septal branches of the anterior ethmoidal artery: anatomical considerations and clinical implications in the management of refractory epistaxis. Eur Arch Otorhinolaryngol. 2018 Jun;275(6):1449-1456. doi: 10.1007/s00405-018-4964-x. Epub 2018 Mar 29. PMID: 29600317. Bird B, Stawicki SP. Anatomy, Head and Neck, Ophthalmic Arteries. 2023 Aug 8, StatPearls Publishing; 2023 Jan–. PMID: 29493942. Prof S.Subbiah et al
- 7. Frontal sinus • 2 Irregular air cavities separated by a thin bony septum. • Connected to Middle meatus by Frontonasal duct. • Anterior :Ethmoid cells (thin bony walls) • Posterior :Anterior cranial fossa Prof S.Subbiah et al
- 8. Frontal sinus ARTERIAL SUPPLY Supraorbital & Anterior ethmoidal arteries VENOUS DRAINAGE Supraorbital & Superior Ophthalmic veins LYMPHATICS Submandibular nodes NERVE SUPPLY Supraorbital nerve Henson B, Drake TM, Edens MA. Anatomy, Head and Neck, Nose Sinuses. 2023 Jul 24. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 30020644. Prof S.Subbiah et al
- 9. Sphenoid sinus (midline) • Superior – Pituitary • Lateral – Cavernous sinuses (Optic nerve & internal carotid artery) • Anterior – Nasal cavity & Ethmoid sinus • Inferior – Nasopharynx • Posteriorly – Clivus and Brainstem. • Connects (anteriorly) with Nasal cavity [Spheno-ethmoidal recess]. Shumway CL, Motlagh M, Wade M. Anatomy, Head and Neck, Orbit Bones. 2023 Jul 24. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 30285385. Prof S.Subbiah et al
- 10. Sphenoid sinus ARTERIAL SUPPLY Posterior ethmoidal artery VENOUS DRAINAGE Corresponding vein LYMPHATICS Retropharyngeal nodes NERVE SUPPLY • Posterior ethmoidal nerves (Sensory) • Pterygopalatine ganglion (Secretomotor) D P, Prabhu LV, Kumar A, Pai MM, Kvn D. The anatomical variations in the neurovascular relations of the sphenoid sinus: an evaluation by coronal computed tomography. Turk Neurosurg. 2015;25(2):289-93. Prof S.Subbiah et al
- 11. PATTERNS OF SPREAD ETHMOID SINUSES • Tumor invade the medial orbit (lamina papyracea, inner canthus) and the nasal cavity. • Advanced lesions invade the maxillary antrum, nasopharynx, sphenoid sinus, and anterior cranial fossa. . Prof S.Subbiah et al
- 12. SPHENOID SINUS • Cranial nerves (CNs) in the cavernous sinus: III, IV, V1, V2, and VI. • CN palsies and headaches (Initial presentation) Prof S.Subbiah et al
- 13. LYMPHATIC SPREAD • 10% --15% for Nasal cavity & Ethmoid sinus SCCs • Lower for Antral & Sphenoid tumors • Lesions of Nasal cavity or Nasopharynx spread to the retropharyngeal nodes & to level II nodes. • Cervical node involvement in Neuroendocrine carcinoma & Esthesioneuroblastoma – 20% to 25% Prof S.Subbiah et al
- 14. METASTASES • Usually to Lungs, spread to bone (occasional). • Blood-borne metastases – (uncommon) • Olfactory neuroblastoma & Malignant melanoma {uncontrolled local disease, need longer follow-up} • Adenoid cystic carcinoma [Perineural lymphatics] – • Some distance from the original tumor. • Patients can survive for some time with disseminated disease Prof S.Subbiah et al
- 15. CLINICAL PICTURE • ETHMOID SINUS: • Mild-to-moderate sinus pain referred Frontal-nasal area [Early symptom] • Painless mass near the inner canthus. • Diplopia & Proptosis [Medial orbit]. • Nasal discharge, Epistaxis & Nasal obstruction. • FRONTAL SINUS: • Swelling of the forehead. • SPHENOID SINUS: • Orbital symptoms [visual loss]. Chondrosarcoma [Bilateral]. Prof S.Subbiah et al
- 16. Orbital Invasion • 50% of Sinonasal tumors • [Orbital displacement, Ecchymosis, visual acuity reduction (20%)] • Most common in Ethmoid sinus tumors [62%] • Lannetti et al – 3 stages of Orbital invasion: 1. Erosion or destruction of the medial orbital wall; 2. Extraconal invasion of periorbital fat; 3. Invasion of the medial rectus muscle, optic nerve, ocular bulb or eyelid skin Iannetti G, Valentini V, Rinna C, Ventucci E, Marianetti TM. Ethmoido-orbital tumors: our experience. J Craniofac Surg. 2005 Nov;16(6):1085-91. doi: 10.1097/01.scs.0000164332.81428.ba. PMID: 16327559. Prof S.Subbiah et al
- 17. TNM staging – ‘T’ staging Prof S.Subbiah et al
- 18. TNM staging Prof S.Subbiah et al
- 19. TREATMENT -ETHMOID SINUS • Surgery (Preferred) if total resection is possible. Postoperative RT or CRT is usually indicated. • Unresectable tumors are treated with CRT. • Surgical Treatment: • Endoscopic endonasal approaches or Open craniofacial resection • Radiation Therapy: • IMRT (Intensity Modulated RT) & IMPT (Intensity Modulated Proton Therapy). Lewis L, Kreinbrink P, Richardson M, Intensity Modulated Proton Therapy Better Spares Non-Adjacent Organs and Reduces the Risk of Secondary Malignant Neoplasms in the Treatment of Sinonasal Cancers. Med Dosim. 2022 Summer;47(2):117-122. doi: 10.1016/j.meddos.2021.11.002. Epub 2021 Dec 21. PMID: 34952761. Prof S.Subbiah et al
- 20. Surgical options • Open approach: Lateral rhinotomy or Weber-Ferguson incision, with bifrontal craniotomy – Resect lesions extending to the skull base. • Endoscopic endonasal approach under image guidance – Minimized the external incisions & craniotomies. • Skull base reconstruction: • Pericranial flap • Nasoseptalor free flap Abdelmeguid AS, Raza SM, Su SY, Kupferman M, Roberts D, DeMonte F, Hanna EY. Endoscopic resection of sinonasal malignancies. Head Neck. 2020 Apr;42(4):645- 652. doi: 10.1002/hed.26047. Epub 2019 Dec 24. PMID: 31875340. Prof S.Subbiah et al
- 21. Skull base reconstruction Pericranial flap Nasoseptalor flap Patel MR, Shah RN, Snyderman CH, Carrau RL, Germanwala AV, Kassam AB, Zanation AM. Pericranial flap for endoscopic anterior skull-base reconstruction: clinical outcomes and radioanatomic analysis of preoperative planning. Neurosurgery. 2010 Mar;66(3):506-12; discussion 512. doi: 10.1227/01.NEU.0000365620.59677.FF. PMID: 20173545. Zanation AM, Carrau RL, Snyderman CH, Germanwala AV, Gardner PA, Prevedello DM, Kassam AB. Nasoseptal flap reconstruction of high flow intraoperative cerebral spinal fluid leaks during endoscopic skull base surgery. Am J Rhinol Allergy. 2009 Sep-Oct;23(5):518-21. doi: 10.2500/ajra.2009.23.3378. PMID: 19807986. Prof S.Subbiah et al
- 22. Pericranial flap Prof S.Subbiah et al
- 23. SPHENOID SINUS • Primary tumors [rare]. • Limited tumors – Surgical resection, • Most tumors – RT or CRT, [Techniques similar to advanced nasopharyngeal carcinoma]. • Recommended treatment is RT with IMRT Ghosh R, Dubal PM, Chin OY, Patel TD,Sphenoid sinus malignancies: a population-based comprehensive analysis. Int Forum Allergy Rhinol. 2016 Jul;6(7):752-9. doi: 10.1002/alr.21733. Epub 2016 Feb 19. PMID: 26891865. DeMonte F, Ginsberg LE, Clayman GL. Primary malignant tumors of the sphenoidal sinus. Neurosurgery. 2000 May;46(5):1084-91; discussion 1091-2. doi: 10.1097/00006123-200005000-00012. PMID: Prof S.Subbiah et al
- 24. • 4 common Histopathologies • SCC (29.4%), • Adenocarcinomas (14.4%), • Non-Hodgkin's mature B-cell lymphomas (13.1%), • Unspecified epithelial neoplasms (11.0%). • Overall 5-year disease-specific survival (DSS) – 48.1%. • 5-year DSS • Mature B-cell NHL (64.0%) • Unspecified epithelial neoplasms (25.6%). Prof S.Subbiah et al
- 25. Frontal sinus • <1% of Sinonasal malignancies; Male Predominance; Age 61.5 yrs • Histology: • Squamous Cell Carcinoma [MC], • Mature B-cell NHLs (Good prognosis) • Epithelial neoplasms NOS • Adenocarcinomas (Poor Prognosis). • University of Florida Staging System Stage I: Limited to the site of origin Stage II: Extension to adjacent sites (Orbit, PNS, Skin, Nasopharynx, Pterygomaxillary fossa) Stage III: Skull base or pterygoid plate destruction and/or intracranial extension • Resection with Adjuvant RT • 5 yr OS – 31% to 50% • DSS of 44.2% for all histologies Bhojwani A, Frontal Sinus Malignancies: A Population-Based Analysis of Incidence and Survival. Otolaryngol Head Neck Surg. 2016 Apr;154(4):735-41. doi: 10.1177/0194599815621878. Epub 2015 Dec 23. PMID: 26701175. Prof S.Subbiah et al
- 26. Recurrent disease • As Recurrent pain and CN palsies. • Localized recurrence after surgery only – CRT or Craniofacial resection and postoperative RT or CRT. • RT failures – Maxillectomy or Craniofacial resection. • Resected with negative margin – improved PFS and OS (select patients) Schur SE, Hanna EY, Su SY, Kupferman ME, DeMonte F, Raza SM. Impact of salvage surgery for recurrent sinonasal cancers with skull base and intracranial involvement. J Neurosurg. 2022 Feb 4:1-8. doi: 10.3171/2021.12.JNS212278. Epub ahead of print. PMID: 35120325. Prof S.Subbiah et al
- 27. CHEMOTHERAPY • Evolving area of investigation • Reserved Locally advanced disease, Marginally resectable, unresectable, or Metastatic disease. • Induction Chemotherapy • Platinum compound & Taxanes as doublet or Triplet (fluorouracil, ifosfamide, or cetuximab). • Followed by definitive CRT or RT followed by surgery for any residual disease • Superior Orbital preservation & Increased DFS Abdelmeguid AS, Teeramatwanich W, Neoadjuvant chemotherapy for locoregionally advanced squamous cell carcinoma of the paranasal sinuses. Cancer. 2021 Jun 1;127(11):1788- 1795. doi: 10.1002/cncr.33452. Epub 2021 Feb 10. PMID: 33567468. Lee MM, Vokes EE, Multimodality therapy in advanced paranasal sinus carcinoma: superior long-term results. Cancer J Sci Am. 1999 Jul-Aug;5(4):219-23. PMID: 10439167. Prof S.Subbiah et al
- 28. Concurrent Chemoradiation Therapy • Concurrent Cisplatin to RT • Unresectable disease, • +ve margins, or +ve lymph nodes with ENE. • Treated with RT dose 70Gy. Bhattasali O, Holliday E, Kies MS, Hanna EY, Garden AS, Rosenthal DI, Morrison WH, Gunn GB, Fuller CD, Zhu XR, Frank SJ. Definitive proton radiation therapy and concurrent cisplatin for unresectable head and neck adenoid cystic carcinoma: A series of 9 cases and a critical review of the literature. Head Neck. 2016 Apr;38 Suppl 1:E1472-80. doi: 10.1002/hed.24262. Epub 2015 Nov 11. PMID: 26561041. Hoppe BS, Nelson CJ, Gomez DR, Stegman LD, Wu AJ, Wolden SL, Pfister DG, Zelefsky MJ, Shah JP, Kraus DH, Lee NY. Unresectable carcinoma of the paranasal sinuses: outcomes and toxicities. Int J Radiat Oncol Biol Phys. 2008 Nov 1;72(3):763-9. doi: 10.1016/j.ijrobp.2008.01.038. Epub 2008 Apr 18. PMID: 18395361. Prof S.Subbiah et al
- 29. Adenocarcinoma • < 30% are woodworkers • Middle meatus (MC) • Spread to Ethmoid anteriorly (mass in the glabella) • Posteriorly to Spheno-Ethmoidal recess & Nasopharynx. • Types: Salivary gland type, Metastatic adenocarcinomas, Sino Nasal (intestinal & non-intestinal) • Nonintestinal • Excellent prognosis (20-30% local recurrence) • Intestinal • Locally aggressive – High risk of metastasis to cervical lymph nodes & lung. • 50% local recurrence Generally Radioresistant. Surgery Requires Craniofacial resection, Endoscopic resection (Select cases) Howard DJ, Lund VJ, Wei WI. Craniofacial resection for tumors of the nasal cavity and paranasal sinuses: a 25-year experience. Head Neck. 2006 Oct;28(10):867-73. doi: 10.1002/hed.20432. PMID: 16823871. Cawte T, Taskin M, Kacker A, Wahl S, Martinez SA. Low-grade adenocarcinoma of nasal passages. Otolaryngology–Head and Neck Surgery. 1997;117(1):116-119. doi:10.1016/S0194-59989770217-1 Prof S.Subbiah et al
- 30. Inverted papilloma [Schneiderian Papillomas] • Lateral nasal wall (68%), Ethmoid and maxillary sinus (57%) & Nasal septum (28%). • Intracranial extension – carcinoma. • Higher prevalence of HPV with low transcriptional activity. • 20% -- Surface keratinization, • 5% to 10% -- Dysplasia • 10% develop into SCC Weissler MC, Montgomery WW, Turner PA, Montgomery SK, Joseph MP. Inverted papilloma. Ann Otol Rhinol Laryngol. 1986 May-Jun;95(3 Pt 1 doi: 10.1177/000348948609500301. PMID: 3717844. Prof S.Subbiah et al
- 31. Schneiderian Papillomas • Bilateral & Multicentric sites of origin • Recurrence risk • 71% – Intranasal procedure • 56% -- Caldwell-Luc approach. • 29% -- Lateral rhinotomy (lowest) • RT in the form of adjuvant or definitive treatment reduces the recurrence Rutenberg M, Kirwan J, Morris CG, Werning JW, Mendenhall WM. Radiation therapy for sinonasal inverted papilloma. Pract Radiat Oncol. 2013 Oct- Dec;3(4):275-81. doi: 10.1016/j.prro.2012.07.007. Epub 2012 Sep 7. PMID: 24674398. Prof S.Subbiah et al
- 32. Neuroendocrine carcinomas • 5% of PNS tumors • Origin: Ethmoid sinuses (64%), Nasal cavity (32%), Maxillary sinus (14%). • Presented in T4 disease majority (84% metastatic). • Surgical or CRT with etoposide, cisplatin, or carboplatin Mitchell EH, Diaz A, Yilmaz T, Roberts D, Levine N, DeMonte F, Hanna EY, Kupferman ME. Multimodality treatment for sinonasal neuroendocrine carcinoma. Head Neck. 2012 Oct;34(10):1372-6. doi: 10.1002/hed.21940. Epub 2011 Nov 2. PMID: 22052583. Prof S.Subbiah et al
- 33. Neuroendocrine carcinomas • Recurrences: • Local (21%) • Regional (25%) • 5yr OS – 67% & DFS – 44% • Elective treatment of the neck – standard for all patients • Personalized approach – Response to systemic therapy Abdelmeguid AS, Bell D, Hanna EY. Neuroendocrine Carcinoma and Sinonasal Undifferentiated Carcinoma. Adv Otorhinolaryngol. 2020;84:168-184. doi: 10.1159/000457936. Epub 2020 Jul 30. PMID: 32731236. Prof S.Subbiah et al
- 34. Olfactory neuroblastoma or Esthesioneuroblastoma • Rare & Malignant neuroectodermal tumor. • 3 – 5% of Sino-nasal tumors • Olfactory epithelium in the upper nasal vault. • Nasal blockade (93%), bleeding (53%) and mass in the upper nasal cavity with associated skull base erosion. • Age 12 – 70 years (mean 46 years) • Cervical metastases –12 to 23% Elkon D, Hightower SI, Lim ML, Cantrell RW, Constable WC. Esthesioneuroblastoma. Cancer. 1979 Sep;44(3):1087-94. doi: 10.1002/1097-0142(197909)44:3<1087::aid-cncr2820440343>3.0.co;2-a. PMID: 383268. Prof S.Subbiah et al
- 35. Esthesioneuroblastoma • Hyams 4 tired Grading • Marker of malignant potential (lobular architecture, mitosis, necrosis, nuclear pleomorphism, fibrillary matrix, and rosettes) • Grades I and II – Low grade • Grades III and IV – High grade • Low grade Hyams had better OS of both 5 & 10 yr survival Goshtasbi K, Abiri A, Abouzari M, Sahyouni R, Wang BY, Tajudeen BA, Hsu FPK, Cadena G, Kuan EC. Hyams grading as a predictor of metastasis and overall survival in esthesioneuroblastoma: a meta-analysis. Int Forum Allergy Rhinol. 2019 Sep;9(9):1054-1062. doi: 10.1002/alr.22373. Epub 2019 Jun 28. PMID: 31251848; PMCID: PMC7276257. Prof S.Subbiah et al
- 36. Esthesioneuroblastoma KADISH STAGING • Stage A : Confined to Nasal cavity • Stage B: Involves nasal cavity + One or More PNS • Stage C : Beyond the Sino-nasal cavities/PNS. (Cribriform lamina, Orbit, Skull-base & Intracranial) • Stage D : Cervical node involvement or Distant metastasis • Early stage (Kadish A/B) – Surgical resection • Advanced stage (Kadish C) – Surgery & Adjuvant RT with elective nodal irradiation (Reduce the local recurrence) Konuthula N, Iloreta AM, Prognostic significance of Kadish staging in esthesioneuroblastoma: An analysis of the National Cancer Database. Head Neck. 2017 Oct;39(10):1962-1968. doi: 10.1002/hed.24770. Epub 2017 Aug 17. PMID: 28815831; PMCID: PMC5993196. Jiang W, Mohamed ASR, The role of elective nodal irradiation for esthesioneuroblastoma patients with clinically negative neck. Pract Radiat Oncol. 2016 Jul-Aug;6(4):241-247. doi: 10.1016/j.prro.2015.10.023. Epub 2015 Nov 10. PMID: 26979544; PMCID: PMC5286455. Prof S.Subbiah et al
- 37. • Lower after Definitive RT (17%) than after craniofacial resection + postoperative RT (56%) • Survival • 5 yr OS – 85.6% • 5 yr DSS – 93.4% Abdelmeguid AS, Bell D, Roberts D, Ferrarotto R, Phan J, Su SY, Kupferman M, Raza S, DeMonte F, Hanna E. Long-Term Outcomes of Olfactory Neuroblastoma: MD Anderson Cancer Center Experience and Review of the Literature. Laryngoscope. 2022 Feb;132(2):290-297. doi: 10.1002/lary.29732. Epub 2021 Jul 17. PMID: 34272876. Esthesioneuroblastoma Prof S.Subbiah et al
- 38. Sinonasal Undifferentiated Carcinoma • High-grade Malignant epithelial neoplasm • No evidence of Squamous or Glandular differentiation • Origin: Schneiderian epithelium or Nasal ectoderm • High rates of Locoregional failure & Distant metastases, (Lungs & bone) • Multimodality treatment (Surgery, Radiation & Chemotherapy) • Prognosis -- Poor Abdelmeguid AS, Bell D, Hanna EY. Sinonasal Undifferentiated Carcinoma. Curr Oncol Rep. 2019 Feb doi: 10.1007/s11912-019-0776-4. PMID: 30806835. Prof S.Subbiah et al
- 39. Sinonasal Undifferentiated Carcinoma • Induction chemotherapy plays a vital role in guiding definitive therapy • 5yr survival • Definitive CRT following induction – 81%; • Partial response following induction – 0%; • Surgical resection + RT or CRT -36% Amit M, Abdelmeguid AS, Watcherporn Induction Chemotherapy Response as a Guide for Treatment Optimization in Sinonasal Undifferentiated CarcinoFeb 20;37(6):504-512. ma. J Clin Oncol. 2019 doi: 10.1200/JCO.18.00353. Epub 2019 Jan 7. PMID: 30615549; PMCID: PMC6380524. Prof S.Subbiah et al
- 40. • 3 cycles of Docetaxel, Cisplatin, and Fluorouracil • Followed by concurrent CRT to 70 Gy with weekly Carboplatin or weekly Carboplatin & Paclitaxel London NR Jr, Mohyeldin A, Daoud G, Gamez ME, Blakaj D, Bonomi M, Prevedello DM, Carrau RL. Sinonasal undifferentiated carcinoma: Institutional trend toward induction chemotherapy followed by definitive chemoradiation. Head Neck. 2020 Nov;42(11):3197-3205. doi: 10.1002/hed.26357. Epub 2020 Jul 18. PMID: 32681692. Prof S.Subbiah et al
- 41. Craniofacial resection • Gold standard – Tumors affecting the Anterior skull base. • INDICATIONS: • Malignant tumors involving the anterior skull base • CONTRAINDICATIONS: • Gross invasion of the brain, both orbits • Encasement of the Internal carotid artery (relative) & Cavernous sinus (relative) • Advanced age • Massive high-grade tumors (e.g., Melanomas, Poorly differentiated carcinomas & High-grade sarcomas) with dural invasion (relative) • Recurrent disease with skull base invasion (previous RT or CRT) Abu-Ghanem S, Fliss DM. Surgical approaches to resection of anterior skull base and paranasal sinuses tumors. Balkan Med J. 2013 Jun;30(2):136-41. doi: 10.5152/balkanmedj.2013.9112. Epub 2013 Jun 1. PMID: 25207089; PMCID: PMC4115977. Prof S.Subbiah et al
- 42. Incisions Prof S.Subbiah et al
- 43. Extent of Resection Prof S.Subbiah et al
- 44. Midfacial degloving • Access to the middle 3rd of the face • Can be used alone or combined with a coronal scalp incision for craniofacial resection • Casson et al (1970) & Price et al (1980) • INDICATIONS • Select tumors – Nasal cavity, maxilla, ethmoids, sphenoid, pterygopalatine and infratemporal fossae. • Bilateral maxillectomy (if required) Abu-Ghanem S, Fliss DM. Surgical approaches to resection of anterior skull base and paranasal sinuses tumors. Balkan Med J. 2013 Jun;30(2):136-41. doi: 10.5152/balkanmedj.2013.9112. Epub 2013 Jun 1. PMID: 25207089; PMCID: PMC4115977. Browne JD. The midfacial degloving procedure for nasal, sinus, and nasopharyngeal tumors. Otolaryngol Clin North Am. 2001 Dec;34(6):1095-104, viii. doi: 10.1016/s0030-6665(05)70368-6. PMID: 11728935. Prof S.Subbiah et al
- 45. Incisions Prof S.Subbiah et al
- 47. Anatomy Roof Sphenoid bone (body) Posterior wall Arch of atlas & Axis bone body Floor Soft Palate Lateral wall Torus tubares of Eustachain tube, Fossa of Rosenmuller. Prof S.Subbiah et al
- 48. • Internal Maxillary Artery branches • Venous drainage – Pterygoid plexus Facial vein IJV • Sensory supply – Maxillary nerve branches. • Lymphatic supply: • Retropharyngeal nodes • Cervical nodes (both Jugular & Spinal Accessory chains) – often bilaterally. Anatomy Prof S.Subbiah et al
- 49. • Lymphatics follows a Predictable and orderly pattern from upper to lower neck; “skip” metastasis - Rare • Nodal >6 cm &/or Extension below the caudal border of the cricoid cartilage – Worst prognosis. • Metastatic sites: • MC Sites: Lung, bone, liver, and distant lymph nodes. • Involvement of lymph nodes below the clavicle (including Mediastinum, Infraclavicular region, axilla, or groin) Distant metastases Patterns of Spread Prof S.Subbiah et al
- 50. TNM Staging Prof S.Subbiah et al
- 51. PATHOLOGY WHO classification Type 1: well-differentiated, Keratinizing Type 2: well-differentiated, Nonkeratinizing Type 3: Undifferentiated, (Basaloid SCC, Lymphoepithelioma & Anaplastic carcinoma) • Type 1 – Oncogenic HPV infection ( worse OS & locoregional recurrence) • Type 2 & 3 – Endemic variants Associated with EBV infection Genetic susceptibility (High distant failure) Prof S.Subbiah et al
- 52. Genetic risk factors & Pathogenesis • Nonsynonymous BALF2 variants (∼80% of Endemic cases) • Oncogenic drivers: • Constitutive activation of the NF-κB pathway • Overexpression of the LMP-1 (Latent Membrane Protein -1) • Other Pathways: • PI3K/AKT/mTOR and MAPK • Chromatin remodeling & TP53 Mutations • Tumor mutational burden (TMB) – 0.9 to >50 mutations/MB pair • “Actionable” Kinase Mutations • ERBB1/2, PI3K, and MAPK – 5% of tumors Prof S.Subbiah et al
- 53. Diagnostic workup & Screening • Neck swelling & Local symptoms • Unilateral epistaxis, Nasal obstruction, Tinnitus, Headaches, or Cranial neuropathies (Advanced NPC) • Gold Std: • HPE assessment of biopsy • Blind (usually from four quadrants of the nasopharynx) • Image -guided Biopsy • SCREENING: • IgA antibodies against early antigen (EA-IgA), • EBV-nuclear antigen 1 (EBNA1-IgA) • EBV capsid antigen (VCA-IgA) • IgG against Zta (Zta-IgG) • EBV-specific DNAase (EBV DNA) antibodies Prof S.Subbiah et al
- 54. Imaging • MRI or CT of the head and neck - Locoregional disease, • 18F-FDGPET or CT of the Thorax & Abdomen • Skeletal scintigraphy – Distant metastasis. • MRI & 18F-FDG-PET are superior modalities for locoregional and distant metastasis staging, respectively Prof S.Subbiah et al
- 55. Clinical & Molecular biomarkers • Parameters • Gross primary tumor volume (GTVp), Number, Size, & Extra-nodal extension (ENE), Neutrophil to Lymphocyte ratio, C-Reactive protein, and Serum lactate dehydrogenase (LDH) levels • Poor Prognostic factors: • GTVp 30 – 50cc, Nodal size > 4-6cm, High Pretreatment LDH Prof S.Subbiah et al
- 56. Treatment – Early stage • Stage 1: RT alone • Stage 2: CRT (high risk features like N1 disease, GTVp >30cc, Plasma EBV DNA titer >500 - 4000copies/ml) • Estimated 5-year OS stage I – 93.2% to 98.9% stage II – 86.6% to 92.5% Au KH, Ngan RKC, Ng AWY, Treatment outcomes of nasopharyngeal carcinoma in modern era after intensity modulated radiotherapy (IMRT) in Hong Kong: A report of 3328 patients (HKNPCSG 1301 study). Oral Oncol. 2018 Feb;77:16-21. doi: 10.1016/j.oraloncology.2017.12.004. Epub 2017 Dec 12. PMID: 29362121. Li XY, Chen QY, Sun XS, Ten-year outcomes of survival and toxicity for a phase III randomised trial of concurrent chemoradiotherapy versus radiotherapy alone in stage II nasopharyngeal carcinoma. Eur J Cancer. 2019 Mar;110:24-31. doi: 10.1016/j.ejca.2018.10.020. Epub 2019 Feb 7. PMID: Prof S.Subbiah et al
- 57. Treatment Prof S.Subbiah et al
- 58. Advanced stage • Stage 3 & 4A: • CRT increased the OS of 6.3% compared to RT alone in low risk groups • High risk groups: • Induction chemotherapy or Metronomic Capacitabine (650mg/m2 for 1 yr) increases the survival compared to CRT and RT alone. • Gemcitabine + Cisplatin is the preferred regimen over TPF regime since toxicity profile is less compared to TPF Chen YP, Liu X, Zhou Q, Yang KY, Metronomic capecitabine as adjuvant therapy in locoregionally advanced nasopharyngeal carcinoma: Lancet. 2021 Jul 24;398(10297):303-313. doi: 10.1016/S0140-6736(21)01123-5. Epub 2021 Jun 7. PMID: 34111416. Yan L, Zheng H, Ren B, Comparison Efficacy and Safety of Gemcitabine plus Cisplatin and 5-Fluorouracil plus Cisplatin for Metastatic Nasopharyngeal Carcinoma: A Meta-Analysis and Systematic Review. J Oncol. 2022 Jul 16;2022:7233559. doi: 10.1155/2022/7233559. PMID: 35880116; PMCID: PMC9308559. Prof S.Subbiah et al
- 59. Recurrent disease • Loco-regional Recurrence: Salvage surgery (preferred) • re-RT(Reirradiation) • IMRT(Intensity Modulated RT) or PBT (Proton beam therapy) or brachytherapy (Risk of severe late toxicities; ∼50% of deaths) • Metastatic disease: • Platinum based Doublet regimen (Gemcitabine + Cisplatin) • Combining chemotherapy with PD-1 inhibitor (Toripalimab or Camrelizumab) for 6 cycles • If Good response – followed by Maintenance PD-1 inhibitor alone Chan ATC, Lee VHF, Hong RL, Ahn MJ, Pembrolizumab monotherapy versus chemotherapy in platinum-pretreated, recurrent or metastatic nasopharyngeal cancer (KEYNOTE-122). Ann Oncol. 2023 Mar;34(3):251-261.doi: 10.1016/j.annonc.2022.12.007. Epub 2022 Dec 16. PMID: 36535566. Liu YP, Wen YH, Endoscopic surgery compared with intensity-modulated radiotherapy in resectable locally recurrent nasopharyngeal carcinoma: a multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2021 Mar;22(3):381-390. doi: 10.1016/S1470-2045(20)30673-2. Epub 2021 Feb 15. PMID: 33600761. Prof S.Subbiah et al
- 60. Treatment Prof S.Subbiah et al
- 61. Nasopharyngectomy • Approaches: • Infratemporal approach from the lateral aspect, • Transpalatal, • Transmaxillary • Transcervical approaches (Inferior & anterolateral) • Resectable recurrent or residue • Salvage Nasopharyngectomy • Persistent neck nodes after RT/CRT • Salvage Neck dissection. Prof S.Subbiah et al
- 62. Incisions Prof S.Subbiah et al
- 63. Extent of resection Prof S.Subbiah et al
- 64. Dingman Self retaining Retractor Prof S.Subbiah et al
- 65. Follow-up • Post CRT • Endoscopy at 6–8 weeks • Imaging at 10–12 weeks after RT/CRT (Document tumor responses) • Surveillance: • Clinical examination – every 4 to 6 months (Initial 3–5 years) • CT and/ or MR imaging – Every 6 months. • Late recurrence – Not uncommon & represent second primary, hence long-term follow up is necessary • FDG PET scan is better than CT for diagnosing Recurrent disease Prof S.Subbiah et al
- 66. Thank you… Prof S.Subbiah et al