Gout and Rheumatoid arthritis (RA)
•Transferir como PPTX, PDF•
10 gostaram•3,720 visualizações

Drugs for Gout and Rheumatoid arthritis (RA)

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Gout and Rheumatoid arthritis (RA)
Semelhante a Gout and Rheumatoid arthritis (RA) (20)
Mais de BikashAdhikari26
Mais de BikashAdhikari26 (20)
Último
Último (20)
Gout and Rheumatoid arthritis (RA)
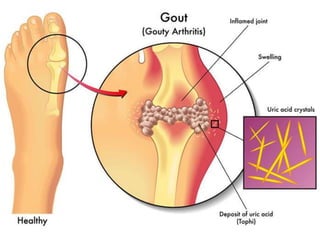
- 2. Gout It is a metabolic disorder characterized by hyperuricaemia (normal plasma urate 2–6 mg/dl). Uric acid, a product of purine metabolism, has low water solubility, especially at low pH. When blood levels are high, it precipitates and deposits in joints, kidney and subcutaneous tissue.
- 3. DRUGS FOR GOUT ACUTE GOUT • NSAIDS • Colchicine • Corticosteroids CHRONIC GOUT Uricosurics • Probenecid • Sulfinpyrazone Synthesis Inhibitors • Allopurinol • Febuxostat
- 4. NSAIDS Strong antiinflammatory drugs like Naproxen, Piroxicam, Diclofenac, Indomethacin or Etoricoxib have beneficial effects on acute Gout. They inhibit the synthesis of Prostaglandins and inhibit chemotactic migration of leucocytes into the inflamed joint. Thus they reduce inflammation in gout.
- 5. COLCHICINE It is a plant alkaloid obtained from Colchicum autumnale which specifically suppresses gouty inflammation. MOA: Colchicine binds to protein tubulin and inhibits microtubule formation, arresting granulocyte motility and decreasing inflammation. Colchicine also inhibits leukocyte chemotaxis, formation of glycoprotein and phagocytosis. Indication: • Antiinflammatory in Gout (NSAIDs alternative) • Chondritis • Prophylaxis of Gout Dose: 1mg starting and then 0.5mg 2-3 hourly until pain reduces (total 3 doses/day)
- 6. Adverse effects • Nausea, Vomiting, Abdominal Pain, Diarrhoea • Myopathy, Neutropenia, Aplastic anaemia, Alopecia (prolong use) Contraindications • Pregnancy • Liver disease • Renal disease • Cardiovascular disease
- 7. CORTICOSTEROIDS Corticosteroids act by inhibiting the conversion of phospholipids into arachidonic acid and supress inflammation. Corticosteroids are given through: • Oral route • Intraarticular route • Intramuscular route Orally Prednisolone 40–60 mg may be given in one day, followed by tapering doses over few weeks.
- 8. URICOSURICS: The drugs that promote renal clearance of uric acid by inhibiting urate reabsorption. PROBENECID MOA: It Inhibits the tubular reabsorbtion of urate, thus increasing the urinary excretion of uric acid & decreasing serum urate level. Indications: • Chronic Gout & Hyperuricemia • Prolong the action of Penicillin Dose: 250-500mg BD Adverse effects: • Dyspepsia • Hypersensitivity (Rashes) • Gastric distress (Peptic ulcer) Contraindications: Probenecid should be avoided if the patient’s creatinine clearance is less than 50 ml/min.
- 9. ALLOPURINOL MOA: Allopurinol is a purine analog which inhibits the enzyme xanthine oxidase and reduces blood levels of uric acid. Indications: • Hyperuricemia in Gout • Hyperuricemia in Cancer or Renal diseases • Kala-azar Dose:Start with 100 mg OD, gradually increase as needed to 300 mg/day; maximum 600 mg/day
- 10. Adverse effects • Hypersensitivity (rashes) • Fever • Muscle pain Contraindications • Pregnancy • Lactation • Hypersensiitivity
- 11. FEBUXOSTAT MOA: Febuxostat is a nonpurine xanthine oxidase inhibitor which reduces uric acid formation and decreases uric acid levels in blood. Indications: • Chronic Gout • Hyperuricemia Dose: 40-80mg OD Adverse effects • Liver damage • Diarrhoea • Nausea • headache Contraindications Same as Allopurinol
- 12. RHEUMATOID ARTHRITIS (RA) is an autoimmune disease in which there is joint inflammation, synovial proliferation and destruction of articular cartilage. Immune complexes composed of IgM activate complement and release cytokines (mainly TNFα and IL-1) which are chemotactic for neutrophils.
- 13. The inflammatory cells secrete lysosomal enzymes which damage cartilage and erode bone, while PGs produced in the process cause vasodilatation and pain.
- 14. The goals of drug therapy in RA are: • Ameliorate(reduce) pain, swelling and joint stiffness. • Prevent articular cartilage damage and bony erosions. • Prevent deformity and preserve joint function.
- 15. Drugs for Rheumatoid Arthritis NSAIDS CORTICOSTEROIDS Disease Modifying Antirheumatoid Drugs (DMARDS) 1.Immunosupressants: Methotrexate Azathioprene Cyclosporine 2.Sulphasalazine 3.Hydroxychloroquine 4.Leflunomide 5.TNFα inhibitors: Etanercept Infliximab Adalimumab 6.IL-1 antagonist: Anakinra Gold & Penicillamine are no longer used!
- 16. Disease Modifying Antirheumatoid Drugs (DMARDS) METHOTREXATE Folic acid analog, Antimetabolite MOA: Methotrexate inhibits dihydrofolate reductase (DHFR), the enzyme that converts dihydrofolic acid(FH2) into tetrahydrofolic acid (FH4) and hence inhibits biosynthesis and proliferation of DNA and immune cells (T cell & B cell). In Rheumatoid Arthritis, methotrexate also inhibits cytokine production, chemotaxis and cell-mediated immune reaction. Note:- Conversion of folic acid into its active form, Tetrahydrofolic acid (FH4) is essential for the synthesis of DNA and cell proliferation.
- 17. METHOTREXATEχ Indications: • First Choice DMARDs alone and in combination • Psoriasis, Ankylosing spondylitis • Immunosuppression and anti-inflammatory • Anticancer (Leukaemia, Breast cancer, Carcinomas) Dose For Rheumatoid Arthritis: 7.5-15 mg weekly
- 19. Adverse Effects: • Bone marrow depression • Leukopenia (Decrease WBC) • Thrombocytopenia (↓ Platelets) • Anaemia (Decrease RBC) • Liver damage • Renal failure • Skin reactions • Alopecia • Ocular irritation Contraindications: • Pregnancy • Bone marrow, Liver And Renal Impairment • Ulcerative disorders
- 20. SULPHASALAZINE MOA: Sulphasalzine splits in colon by bacteria into sulfapyridine (antibacterial) and 5-amino salicylic acid (anti-inflammatory). It decreases IgA & IgM factors, suppresses T cell response and has anti- inflammatory & immunosuppressive actions. Indications: • Rheumatoid Arthritis • Inflammatory Bowel Disease Dose: 1-3g/day in divided doses Adverse Effects: • Anaemia • Hepatitis • Male infertility
- 21. HYDROXYCHLOROQUINE MOA: Hydroxychloroquine supress lysosomal enzymes, reduce monocyte IL–1, inhibit B lymphocytes and interfere antigen processing. It also has free radical scavenging activity. Thus it has beneficial effects on Rheumatoid Arthritis when given for long periods of 3-6 months. Indications: • Rheumatoid Arthritis • Anti-malarial Dose: 400 mg/day for 4–6 weeks, followed by 200 mg/day for maintenance Adverse effects: • Retinal damage • IBS • Graying of Hair
- 22. LEFLUNOMIDE MOA: Leflunomide is an immunomodulator which inhibits proliferation of stimulated lymphocytes in patients with active RA. Active metabolite of leflunomide inhibits dihydroorotate dehydrogenase and pyrimidine synthesis in actively dividing cells & antibody production by B-cells is depressed. Indications: • Rheumatoid Arthritis • Immunosuppression Dose: loading dose of 100 mg daily for 3 days followed by 20 mg OD. Adverse effects: • Loss of hair • Thrombocytopenia • Leukopenia
- 23. BIOLOGICALS TNFα inhibitors: Etanercept Infliximab Adalimumab MOA: TNFα inhibitors & IL-1 antagonist bind and inhibit cytokines, especially TNFα or IL-1 and are reserve drugs for severe refractory disease. These drugs mainly suppress macrophage and T-cell function. Thus inflammation in the joint regress and new erosions are slowed. Indications: (given s.c.) Autoimmune diseases like RA, inflammatory bowel diseases, psoriasis, scleroderma, etc. IL-1 antagonist: Anakinra Abatacept
Notas do Editor
- d