
Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (17)
Semelhante a Meaningful EMR Use - RESULTS SUMMARY with LINK
Semelhante a Meaningful EMR Use - RESULTS SUMMARY with LINK (20)
Meaningful EMR Use - RESULTS SUMMARY with LINK
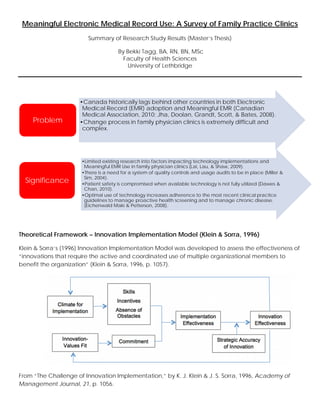
- 1. Meaningful Electronic Medical Record Use: A Survey of Family Practice Clinics Summary of Research Study Results (Master’s Thesis) By Bekki Tagg, BA, RN, BN, MSc Faculty of Health Sciences University of Lethbridge Theoretical Framework – Innovation Implementation Model (Klein & Sorra, 1996) Klein & Sorra’s (1996) Innovation Implementation Model was developed to assess the effectiveness of “innovations that require the active and coordinated use of multiple organizational members to benefit the organization” (Klein & Sorra, 1996, p. 1057). From “The Challenge of Innovation Implementation,” by K. J. Klein & J. S. Sorra, 1996, Academy of Management Journal, 21, p. 1056. •Canada historically lags behind other countries in both Electronic Medical Record (EMR) adoption and Meaningful EMR (Canadian Medical Association, 2010; Jha, Doolan, Grandt, Scott, & Bates, 2008). •Change process in family physician clinics is extremely difficult and complex. Problem •Limited existing research into factors impacting technology implementations and Meaningful EMR Use in family physician clinics (Lai, Lau, & Shaw, 2009). •There is a need for a system of quality controls and usage audits to be in place (Miller & Sim, 2004). •Patient safety is compromised when available technology is not fully utilized (Dawes & Chan, 2010). •Optimal use of technology increases adherence to the most recent clinical practice guidelines to manage proactive health screening and to manage chronic disease. (Eichenwald Maki & Petterson, 2008). Significance
- 2. Research Design – Quantitative Survey Measures Meaningful EMR Use Scale Level Cumulative Capabilities 1 Traditional paper-based practice 2 Electronic reference material, but still paper charting 3 Partial use of computers at point of care for recording patient information 4 Computer has replaced paper chart 5 Advanced clinical decision support in use, including practice level reporting 6 Full EMR interconnected with regional / community hospitals, other practices, labs and pharmacies for collaborative care. (Adapted from Price, Lau & Lai, 2011) Demographics 13 items •Individual •Organizational Innovation Implementation (Klein & Sorra, 1996) 50 items •Implementation Climate •Innovation-Values Fit •Skills •Absence of Obstacles •Incentives •Commitment •Implementation Effectiveness Meaningful EMR Use (Price, Lau & Lai ,2011) 30 items •Health Information •Medications •Laboratory •Medical Imaging •Referrals •Decision Support •Electronic Communication & Connectivity •Patient Support •Administrative processes •Reporting & Population Health Management Convenience sample recruitment methods: • Fax • Paper mail • Phone calls • Networking • Electronic announcements Purpose: explore current meaningful EMR use levels in family physician clinics in Alberta, Canada, and to identify statistically significant factors that contribute to higher meaningful use.
- 3. Findings Responding sample: participants n= 139, clinics n = 44 Telus - Med- Access 34% Telus - Wolf 36% Other (7 EMRs) 30% EMR Use Breakdown Factors Significantly Correlated with Increased Meaningful EMR Use Participation in POSP (F (2,21) = 15.31, p < 0.001) Health zone (F (3,21) = 5.17, p = 0.008) - Highest level of use - Edmonton zone (M = 4.59, SD = 0.64) Innovation-Values Fit (r = 0.49, p ≤ 0.05, R2 = 0.24) Innovation Implementation (r = 0.81, p ≤ 0.01) - Implementation Climate (r = 0.79, p ≤ 0.01, R2 = 0.62) - Task Support, (r = 0.65, p ≤ 0.01) - Goal Emphasis, (r = 0.53, p ≤ 0.01) Implementation Effectiveness: • Positively impacted by intrinsic motivation o (r = 0.59, p ≤ 0.01), • Not impacted by extrinsic motivation (bonuses, raises, or promotions) o (r = 0.14, p = 0.21). Implications and Impact Clinics can increase their Meaningful EMR Use by participating in programs like POSP, by improving employee access to tools, resources, and training, as well as providing clear direction about expected technology use standards and desired outcomes.
- 4. • Small sample size • Meaningful EMR Use scale items (Price, Lau, and Lai, 2011): o New scale - no previous reliabilities o This data set showed low reliabilities (α = 0.50) for 5 items: Electronic Communication and Connectivity, α = 0.48 Health Information, α = 0.45 Patient Support, α = 0.29 Medical Imaging, α = 0.22 Referrals, α = 0.09 • Further research on the Meaningful EMR Use scale (Price, Lau, and Lai, 2011) to assess validity. • Adjustments to the Meaningful EMR Use scale (Price, Lau, and Lai, 2011) to increase reliability. • Targeted study of a group of clinics (ex. a Primary Care Network) at several intervals post EMR adoption or during an improvement initiative. Future Research AreasLimitations Glossary: • EMR – Electronic Medical Record • Goal Emphasis - clear direction about expected standards and outcomes • Health Information – a patient’s medical summary, demographics, and visit notes • Implementation Climate - employee perceptions of the practices, procedures, and behaviors that get rewarded, supported, and expected within their organization. • Implementation Effectiveness - employees feel that the system is a valuable addition to the work practices of the organization, and they choose to use the system when given the opportunity. • Innovation Implementation Model (Klein & Sorra, 1996) - a model assessing the implementation of innovations that require the active and coordinated use of multiple organizational members to benefit the organization. • Innovation-Values Fit - the extent to which users feel the innovation will either foster or inhibit the fulfillment of their values • Meaningful EMR Use – The extent to which the different modules of an EMR system are used. • Patient Support - support provided to patients through the distribution of handouts and test results • POSP – Physician Office Systems Program • Task Support - employees have the tools and resources to keep them up to date with training References: Canadian Medical Association. (2010). National physician survey, 2010: Provincial results by FP/GP or Other Specialist, Sex, Age, and All Physicians: ALBERTA. Retrieved from http://nationalphysiciansurvey.ca/wp- content/uploads/2012/09/2010-ProvAB-Q27.pdf Dawes, M., & Chan, D. (2010). Knowing we practice good medicine: Implementing the electronic medical record in family practice. Canadian Family Physician, 56(1), 15–16. Eichenwald Maki, S., & Petterson, B. (2008). Using the electronic health record. Clifton Park, NY: Delmar Cengage Learning. Jha, A. K., Doolan, D., Grandt, D., Scott, T., & Bates, D. W. (2008). The use of health information technology in seven nations. International Journal of Medical Informatics, 77, 848–854. doi:10.1016/j.ijmedinf.2008.06.007 Klein, K. J., & Sorra, J. S. (1996). The challenge of innovation implementation. Academy of Management Journal, 21, 1055– 1080. doi:10.5465/AMR.1996.9704071863 Lai, J. K., Lau, F., & Shaw, N. (2009). A study of information technology use and implementation of electronic medical record systems in BC medical practices. BC Medical Journal, 51, 114–121. Miller, R. H., & Sim, I. (2004). Physicians’ use of electronic medical records: Barriers and solutions. Health Affairs, 23, 116–126. doi:10.1377/hlthaff.23.2.116 Price, M., Lau, F., & Lai, J. (2011). Measuring EMR adoption: A framework and case study. Electronic Healthcare, 10(1), e25–e30. Author contact information: Bekki.Tagg@uleth.ca Full thesis available at http://hdl.handle.net/10133/3682