Hydatid disease
•Transferir como PPTX, PDF•
34 gostaram•7,968 visualizações

topic presentation on hydatid disease

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (11)
Semelhante a Hydatid disease
Semelhante a Hydatid disease (20)
Mais de BISHAL SAPKOTA
Último
Último (20)
Hydatid disease
- 2. Hydatid Cyst of Liver Introduction Hydatid disease is a worldwide zoonosis produced by the larval stage of the Echinococcus tapeworm . The two main types of hydatid disease are caused by E. granulosus and E. multilocularis. E. granulosus is commonly seen in the great grazing regions of the world— particularly the Mediterranean region, Africa, South America, the Middle East, China & South East Asia 2
- 3. Life cycle of Echinococcus 3
- 4. Hydatid Cyst Structure The hydatid cyst has three layers: (a) the outer pericyst, composed of modified host cells that form a dense and fibrous protective zone; (b) the middle laminated membrane, also k/a Ectocyst which is acellular and allows the passage of nutrients; (c) the inner germinal layer, also k/a Endocyst where the scolices (the larval stage of the parasite) and the laminated membrane are produced. 4
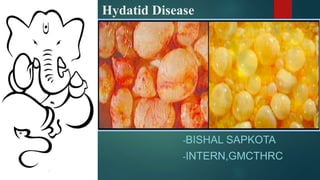
- 5. Daughter vesicles (brood capsules) are small spheres that contain the protoscolices and are formed from rests of the germinal layer. Before becoming daughter cysts, these daughter vesicles are attached by a pedicle to the germinal layer of the mother cyst. At gross examination, the vesicles resemble a bunch of grapes.
- 6. 6
- 7. Pathogenesis The hydatid cysts are mainly located in the liver as the liver acts as 1st filter in 60-70% of human infections as embryos after hatching out penetrates intestinal wall and enter into radical of portal vein. It can also be present in lungs as sometimes the embryo pass through hepatic capillaries and enter the pulmonary circulation , lung act as 2nd filter. 7
- 8. A few embryos may pass through pulmonary circulation too and enter various organs Thus rarely, the cysts may be found in the brain, eye, kidney, muscles ,bones ,spleen, genital organs. 8 Hydatid cyst showing a row of brood capsules attached to the germinal layer.
- 9. Clinical Features The clinical features are highly variable. The spectrum of symptoms depends on the following: Involved organs Size & Site of Cysts Interaction between the expanding cysts and adjacent organ structures( bile ducts & the vascular system of the liver ) Pressure symptoms usually occur late, except when they occur in the brain . Immunologic reactions such as asthma, anaphylaxis, or membranous nephropathy secondary to release of antigenic material 9
- 10. Hepatic Disease The right lobe is the most frequently involved portion of the liver. Once in the human liver, cysts grow to 1 cm during the first 6 months and 2–3 cm annually thereafter, depending on host tissue resistance. 10
- 11. Diagnosis Radiodiagnosis Examination of cyst fluid Serodiagnosis 11
- 12. Radiodiagnosis Plain X-rays pulmonary cysts of E. granulosus - rounded masses of uniform density. But may miss cysts in other organs unless there is cyst wall calcification (as occurs in the liver). 12
- 13. X ray showing Hydatid cyst in left lung. 13
- 14. Xray showing Hydatid cysts in liver 14
- 15. 15MRI, CT, and Ultrasound reveal well-defined cysts with thick or thin walls. The most pathognomonic finding- daughter cysts within the larger cyst. Eggshell or mural calcification on CT, is indicative of E. granulosus infection and helps to distinguish the cyst from carcinomas, bacterial or amebic liver abscesses, or hemangiomas.
- 16. CT scan of liver-showing a Large cyst occupying most of right lobe. And daughter cyst (arrow) attached to germinal membrane by stalk. 16
- 17. CT scan showing a round lesion with water attenuation and a ringlike pattern of calcification (arrows). This pattern represents calcification of the pericyst 17
- 18. a)CT scan-Cystic lesion(arrows) in body and tail of pancreas 18 b)CT scan showing Cystic lesion in spleen and liver c) Two thick walled cysts in lungs
- 19. USG Classification (WHO-IWGE, 2003) Group 1 : Active group – cysts larger than 2 cm and fertile Group 2 : Transition group – cysts starting to degenerate and entering a transitional stage because of host resistance or treatment, but may contain viable protoscolices Group 3 : Inactive group – degenerated, partially or totally calcified cysts, unlikely to contain viable protoscolices. 19
- 20. 20
- 21. Examination of cyst fluid A specific diagnosis of E. granulosus infection can be made by the examination of aspirated fluids for protoscolices or hooklets Not usually recommended because of the risk of fluid leakage resulting in either dissemination of infection or anaphylactic reactions. 21
- 22. Serodiagnosis can be useful, although a negative test does not exclude the diagnosis. Can be carried out by ELISA RIA(radioimmunoassay) Complement fixation IHA(indirect haemagglutination) Cysts in the liver elicit positive antibody responses in 90% of cases whereas up to 50% of individuals with cysts in the lungs are seronegative. Detection of antibody to specific echinococcal antigens by immunoblotting has the highest degree of specificity 22
- 23. Complications Rupture pain anaphylactic reaction peritonitis If biliary tree involved: cholangitis, obstructive jaundice, or pancreatitis. Into the bronchi : expectoration of cyst fluid, scolices. 23
- 24. 24Infection • Liver abscess • Mild fever to full blown sepsis Allergic reactions • Urticaria • Brochospasm • Anaphylaxis • Eosinophilia Pressure Effects • Obstructive Jaundice • Budd-Chiari Syndrome Organ dysfunction • Cholangitis • Biliary Cirrhosis
- 25. Management Medical Therapy Surgical Therapy PAIR (Puncture, Aspiration, Injection & Reaspiration) 25
- 26. Medical Therapy Indications: Patients with primary liver or lung cysts that are inoperable Patients with cysts in 2 or more organs, and Peritoneal cysts. Chemotherapeutic agents: Two benzimidazoles are used, albendazole and mebendazole. Albendazole is administered in several 1-month oral doses (10-15 mg/kg/d) separated by 14-day intervals. The optimal period of treatment ranges from 3-6 months, Mebendazole is also administered for 3-6 months orally in dosages of 40- 50 mg/kg/d. Praziquantel 60mg/kg along with albendazole for 2 weeks. 26
- 27. Contraindications to Medical Therapy Early pregnancy, Bone marrow suppression, Chronic hepatic disease, Large cysts with the risk of rupture, and Inactive or calcified cysts. 27
- 28. PAIR Performed using either ultrasound or CT guidance, Puncture usually using a 22G needle through thickest portion Involves aspiration of the contents via a special cannula, followed by Injection of a scolicidal agent for at least 15 minutes, and then Reaspiration of the cystic contents. The cyst is then filled with isotonic sodium chloride solution. Perioperative treatment with a albendazole (15mg/kg/d) in 2 divided doses is mandatory (4 days prior to the procedure and 1-3 months after). The cysts larger than 6 cm in diameter should undergo PAIR technique with drain catheter placed for 24 hrs. 28
- 29. 29 Puncture Confirmation of diagnosis aspiration Injection of scolicidal agent Reaspiration
- 30. Indications Inoperable patients Patients refusing surgery Multiple cysts in segment I, II, and III of the liver Relapse after surgery or chemotherapy Contraindications Early pregnancy, Lung cysts, Inaccessible cysts, Superficially located cysts (risk of spillage), and Cysts communicating with the biliary tree (risk of sclerosing cholangitis from the scolecoidal agent). 30
- 31. Surgical Treatment Choice of Surgery: Radical total or partial pericystectomy with omentoplasty Hepatic segmentectomy During the operation scolicidal agents are used. Nowadays Laparoscopic Approach is being tried. (Laparoscopic Pericystectomy) 31
- 32. Indications Large liver cysts with multiple daughter cysts; superficially located single liver cysts that may rupture (traumatically or spontaneously). Liver cysts with biliary tree communication or pressure effects on vital organs or structures. Infected cysts . Cysts in lungs, brain, kidneys, eyes, bones . Contraindications General contraindications to surgical procedures Multiple cysts in multiple organs; Cysts that are difficult to access; Dead cysts; Calcified cysts Very small cysts 32
- 33. 33
- 34. Hydatid Cyst removed from Brain 34
- 35. Conclusion Many hydatid cysts remain asymptomatic, even into advanced age. Parasite load, the site, and the size of the cysts determine the degree of symptoms. The liver is the most common organ involved, followed by the lungs. These 2 organs account for 90% of cases of echinococcosis. Surgery remains the main treatment of the hydatid liver disease , PAIR technique still promising. Patient education about the prevention of this zoonotic infection . 35
- 36. MCQ 36 Q} water lily appearance in a chest radiograph suggest a. Metastasis b. Cavitating metastasis c. Aspergilloma d. Ruptured hydatid cyst
- 37. Q} diagnosis of hydatid disease is by a. Biopsy b. X-ray c. Casoni test d. Serum examination Q} during surgical exploration for hydatid cystof liver any of the follwing except can be used as scolicidal a. Hypertonic saline b. Formalin c. Cetrimide d. Povidine iodine
- 38. References Bailey And Love’s Short Practice Of Surgery, 25th Edition SRB’s MANUAL OF SURGERY;4E Schwart’s Principles Of Surgery;10E Surgery Essence;3E; Pritesh Singh Bedside Clinicals in Surgery; Makhan lal saha;1E ,2011 reprint Internet Sources Google Webmd.Com Radiopedia.Org 38
- 39. ANY QUESTIONS?
Notas do Editor
- Figure 8. Calcified unilocular hydatid cyst. Contrast material-enhanced CT scan shows a round lesion with water attenuation and a ringlike pattern of calcification (arrows). This pattern represents calcification of the pericyst and strongly suggests a diagnosis of hydatid cyst.