Recomendados

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a cannabidiol therapy in the treatment of chronic pain
Semelhante a cannabidiol therapy in the treatment of chronic pain (20)
cannabidiol therapy in the treatment of chronic pain
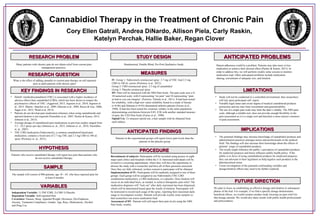
- 1. RESEARCH PROBLEMRESEARCH PROBLEM RESEARCH QUESTIONRESEARCH QUESTION IMPLICATIONSIMPLICATIONS SAMPLESAMPLE * . KEY FINDINGS IN RESEARCHKEY FINDINGS IN RESEARCH MEASURESMEASURES FUTURE DIRECTIONFUTURE DIRECTION Cannabidiol Therapy in the Treatment of Chronic Pain Cory Ellen Gatrall, Andrea DiNardo, Allison Piela, Carly Raskin, Katelyn Perchak, Hallie Baker, Regan Clover Many patients with chronic pain do not obtain relief from current pain management practices. What is the effect of adding cannabis to current pain therapy on self-reported pain in adult patients with chronic pain? • Delta9- tetrahydrocannabinol (THC) is associated with a higher incidence of adverse effects than cannabidiol (CBD), which has been shown to temper the psychoactive effects of THC. (Aggarwal, 2013; Jognson et al., 2010; Jognson et al., 2013; Martin –Sanchez et al., 2009; Motcutt et al., 2004; Russo & Guy, 2006; Sagar et al., 2012; Ward et al, 2013). • Patients do not develop pain medication tolerance when using cannabinoids and upward titration is not required (Nurmikko et al., 2007; Pacher & Kunos, 2013; Johnson et al., 2013). • Average dosage of cannabinoid pain medications in previous studies ranged from 5.5 - 10.2 sprays per day (Johnson et. al., 2013; Johnson et. al., 2010; Nurmikko et. al., 2007). • THC:CBD medication (Naboximols), a common cannabinoid-based pain medication, contains a fixed ratio of 2.7 mg THC and 2.5 mg CBD in 100 uL spray (Portenoy et. al., 2012). HYPOTHESISHYPOTHESIS Patients who receive cannabidiol therapy will report less pain than patients who do not receive cannabidiol therapy. STUDY DESIGNSTUDY DESIGN The sample will consist of 800 patients, age 18 – 65, who have reported pain for at least 6 months. Randomized, Double Blind, Pre-Post Qualitative Study PROCEDUREPROCEDURE LIMITATIONSLIMITATIONS VARIABLESVARIABLES Independent Variable: 1) THC/CBD, 2) CBD 3) Placebo Dependent Variable: Self-reported Pain Covariates: Nausea, Sleep, Appetite/Weight, Dizziness, Dys/Euphoria, Anxiety, Treatment Compliance, Gender, Age, Race, Medications, Alcohol and Drug Use IV: Group 1: Naboximols oromucosal spray: 2.7 mg of THC And 2.5 mg CBD in 100 uL carrier (Portenoy et al., 2012). Group 2: CBD oromucosal spray: 2.5 mg of cannabidiol Group 3: Placebo oromucosal spray DV: Pain will be measured with the NRS Pain Scale. The pain scale uses a 0- 10 numerical scale; with 0 representing “no pain” and 10 representing “pain as bad as you can imagine” (Ferreira- Valente et al., 2011). It had been tested for reliability, with a high test- retest reliability found in a study of literate (r=0.96) and illiterate (r=0.95) rheumatoid arthritis patients (Ferraz et al., 1990). It had also been tested for construct validity in the same population, demonstrating correlations between 0.85- 0.96 with another standard measure of pain, the VAS Pain Scale (Ferraz et al., 1990). Opioid Use: To measure opioid use, a hair sample with be obtained from each subject. Recruitment of subjects: Participants will be recruited using posters in eight major pain clinics and hospitals within the U.S. Interested individuals will be invited to a screening appointment, where they will have the opportunity to discuss the study with a researcher and have all of their questions answered. Once they are fully informed, written consent to participate will be obtained Implementation of IV: Participants will be randomly assigned to one of three groups: Each group will be assigned to use Naboximols (THC:CBD combination medication), a CBD medication, or a placebo. Dose titration will occur on an individual basis, as needed, to achieve therapeutic pain relief. The medication dispenser will “lock out” after daily maximum has been dispensed, which will be determined based upon the results of titration. Participants will be instructed to record each usage of the spray, reporting their maximum daily usage to investigators weekly. Patients will provide weekly urine samples so that researchers can assess medication load. Assessment of DV: Patients will self-report their pain levels using the NRS Pain Scale, weekly ANTICIPATED FINDINGSANTICIPATED FINDINGS Patients in the experimental groups will report lower pain levels than the patients in the placebo group • Study will not be conducted in a controlled environment, thus researchers will rely upon participant self- report. • Variable legal status and social stigma of medical cannabinoid products possession and use may limit recruitment and generalizability. • The use of a single pain scale may limit the data’s validity. The NRS pain scale, although a reliable tool, does not provide enough flexibility in the pain assessment as it is a single tool and therefore a more narrow construct of pain assessment. • The potential findings may increase knowledge of cannabidiol products and administration practices amongst nurses and professionals in the medical field. The findings will also increase their knowledge about the effects of patients’ usage of cannabidiol products. • The results might influence the public’s perception of cannabidiol products for medicinal purposes and hence influence public health policy. If the public is in favor of using cannabidnoid products for medicinal purposes, they can advocate to their legislators to help legalize such products in the pharmaceutical arena. • Closer investigation of the potential confounding variables and dosage/titration effects may need to be further explored. We plan to focus on establishing an effective dosage and titration in subsequent phases of the trial. For example, if we find a specific dosage demonstrates beneficial effects, we would conduct another study focusing on pain relief for that dosage amount. We would also share results with public health professionals and policymakers. ANTICIPATED PROBLEMSANTICIPATED PROBLEMS Patient adherence could be a problem. Patients may take more or less medication to achieve their desired effect (Pacher & Kunos, 2013). In order to address this, we will perform weekly urine screens to monitor medication load. Other anticipated problems include medication sharing, recruitment of adequate size, and titration.