4 u1.0-b978-1-4160-4224-2..50022-3..docpdf
•
1 gostou•2,194 visualizações

This document discusses teratogenesis and environmental exposures that can increase risks during pregnancy. It defines a teratogen as an agent that can interfere with normal embryo or fetal development. While major birth defects are usually considered, teratogens can also increase risks of other adverse outcomes. About 10% of major birth defects are due to environmental exposures. The document reviews historical cases of recognized teratogens like thalidomide and discusses principles of teratology, mechanisms of pathogenesis, adverse case reports, and pregnancy registries for monitoring drug safety.

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (19)
Semelhante a 4 u1.0-b978-1-4160-4224-2..50022-3..docpdf
Semelhante a 4 u1.0-b978-1-4160-4224-2..50022-3..docpdf (20)
Mais de Loveis1able Khumpuangdee
Mais de Loveis1able Khumpuangdee (20)
Último
Último (20)
4 u1.0-b978-1-4160-4224-2..50022-3..docpdf
- 1. Chapter 20 Teratogenesis and Environmental Exposure Christina Chambers, PhD, MPH, and Carl P. Weiner, MD, MBA A teratogenic agent is defined as one that has the potential to interfere lidomide, a sedative-hypnotic drug, was associated with a dramatic with the normal functional or structural development of an embryo increase in risk for a characteristic pattern of limb reduction anomalies or fetus. A teratogenic exposure occurs when a pregnant woman is and other defects.3,4 Although the drug had undergone premarket exposed to an agent that increases risk. Although teratogenic exposures testing in rodents, it had not shown any evidence of adverse outcomes are generally thought of as those that increase the risk for major con- in these species. The subsequent recognition that therapeutic agents genital anomalies, in the broader sense, teratogenic exposures also could induce malformations was a major stimulus for the implementa- increase the risk for a spectrum of adverse pregnancy outcomes, tion of the Kefauver-Harris Amendment to the Food, Drug and including spontaneous abortion, stillbirth, minor structural anoma- Cosmetic Act in the United States, which expanded the role of the Food lies, shortened gestational age, growth restriction, and behavioral or and Drug Administration (FDA) as a regulatory agency charged with cognitive deficits. However, excess risks for these latter events are much ensuring both the efficacy and the safety of products.5 more difficult to recognize. Although the thalidomide experience raised public awareness of the The currently known teratogenic exposures comprise a wide range potential risks of prenatal exposures, it was accompanied by misun- of agents, including some prescription and over-the-counter medica- derstandings about how to differentiate exposures that actually cause tions, recreational drugs and alcohol, chemicals, physical agents, and birth defects from coincidental exposures occurring in women whose maternal diseases. Although studies specifically evaluating human tera- pregnancy outcome is abnormal for other, unrelated reasons. A classic togenicity are lacking for most environmental agents, including pre- example is doxylamine succinate and pyridoxine hydrochloride with scription medications, it is generally estimated that at least 10% of or without dicyclomine hydrochloride (Bendectin®), a once popular major birth defects are attributable to environmental exposures and antiemetic medication used by as many as 30% of American women therefore are, to some extent, preventable.1 As a result, the possible for the treatment of nausea and vomiting of pregnancy. In 1983, this teratogenicity of agents to which a woman may be exposed during agent was voluntarily withdrawn from the market after anecdotal con- pregnancy is of great concern to the general public and requires that cerns for teratogenicity triggered on onslaught of litigation, despite clinicians develop expertise in evaluating these risks on behalf of their voluminous scientific evidence to the contrary.6 patients. Within the last 40 years, research in the field of teratology has advanced, and several new human teratogens have been identified, including several anticonvulsants, selected antineoplastic agents, Historical Perspective inhibitors of enzymes in the angiotensinogen-angiotensin pathway, methylmercury, cocaine, alcohol, hyperthermia, tetracycline, warfarin, Before the 1940s, it was somewhat naively thought that the placenta and isotretinoin.7 Work continues to better define the range of adverse provided a protective barrier for the developing embryo and fetus, so outcomes associated with these exposures, the magnitude of the risk that agents to which the mother was exposed could not interfere with for a given dose at a specific gestational age, and the subpopulations normal prenatal development. The revolutionary concept that a mater- of mothers and infants who may be at particularly increased risk nal exposure could pose a risk to the developing embryo or fetus was because of their genotype. However, major knowledge gaps exist for first raised, not by a scientist or an obstetrician, but rather by an Aus- most agents—few of which have been adequately evaluated in human tralian ophthalmologist, Norman Gregg, who observed in his own pregnancy.8 clinical practice an unusual number of children diagnosed with con- Concerns regarding the inadequacy of accurate information for genital cataracts shortly after a rubella epidemic. Gregg’s work led to the developmental effects of a majority of therapeutic and over-the- investigations that identified additional features of a variable but char- counter agents are critical. Studies indicate that drug exposure during acteristic pattern of developmental abnormalities associated with fetal pregnancy is extremely common: in one U.S. health care system sample rubella infection, including congenital heart defects, hearing deficits, of 98,182 deliveries, 64% of women were prescribed at least one medi- and endocrine abnormalities, all of which came to be known as the cation during their pregnancy other than a vitamin or mineral supple- congenital rubella syndrome.2 ment.9 In another U.S. population–based sample of women, more than In the early 1960s, an Australian obstetrician and a German geneti- 70% reported the use of one or more over-the-counter medications cist independently recognized that first-trimester maternal use of tha- during pregnancy.10 Therefore, a theoretical and practical framework
- 2. 348 CHAPTER 20 Teratogenesis and Environmental Exposure is necessary to aid clinicians in advising patients, who are likely to have portion of the first trimester, whereas later gestational exposure is experienced several exposures by the time their pregnancy is recog- associated with central nervous system (CNS) effects.18 The former nized, and to help support evidence-based clinical decision making abnormality likely reflects a vitamin K deficiency, the latter a complica- in the common situations in which pregnancy exposures can be tion of fetal bleeding. anticipated. Consistent with these concepts, very early gestational exposure, limited in general to the first 2 weeks after conception, is thought to pose little potential for teratogenicity. This is true in part because of Principles of Teratology the limited biologic availability to the embryo of an agent that is taken and eliminated by the mother before the completion of placentation. Wilson and Fraser11 outlined the basic principles of teratology in the Further, pluripotent cells of the early embryo may be resilient in recov- early 1970s to aid in identifying those agents with teratogenic potential ering from a teratogenic insult, or, alternatively, they may be particu- and to provide a basis for establishing causality. Appreciation of these larly vulnerable to a teratogenic exposure, resulting in spontaneous principles can help clinicians place into context research findings from abortion before the clinical recognition of pregnancy.11 the literature as well as individual patient histories. The principles The principle of dose response suggests that, for those agents discussed here are species specificity, genetic susceptibility, gestational that are teratogenic, there is a threshold dose below which no effect is timing, dose response, route of administration, spectrum of outcomes, detected, and higher doses produce stronger effects relative to lower and specific mechanisms leading to pathogenesis. doses, with the highest doses being lethal. For example, when the The principle of species specificity, in combination with the concept anticonvulsant valproic acid is ingested by a pregnant woman during of genetic susceptibility, holds that agents that are teratogenic in one the critical window for neural tube closure, the risk for that defect species may not be so in another. Similarly, the manifestations of a increases by approximately 10- to 20-fold, from a baseline risk of 0.1% teratogenic exposure may differ across susceptible species, and, even to a risk of 1% to 2% . However, there is evidence that the risk is dose- within species, certain strains or individuals may be at higher risk than related, because valproate-treated mothers who deliver infants with others. spina bifida on average have taken significantly higher doses than val- These two principles have implications for the predictive value of proate-treated mothers of normal newborns.19 preclinical animal reproductive toxicity studies; for example, thalido- The principle of route of administration is closely linked to the mide was not teratogenic in the species initially tested, and only after principle of dose response from the standpoint of influencing the its recognition as a human teratogen was the most sensitive animal effective dose that is biologically available to the embryo or fetus. This species identified.12 Variability in susceptibility is also evident within is a critical element in the design of animal reproductive and develop- species, including humans, where no teratogenic agent at typical doses mental toxicity studies in terms of their comparability to human preg- has been demonstrated to produce adverse effects in 100% of concep- nancy exposures. This principle can be applied to studies regarding the tuses. Even potent, known human teratogens such as thalidomide and relative toxicity of human exposures resulting from oral dosing versus isotretinoin affect fewer than 50% of exposed infants. In some cases, topical application. For example, retinoids as a class have been identi- this variability in susceptibility has been linked to specific genetic fied as human teratogens with effects that depend on the dose and polymorphisms that interact with the agent to create a particularly timing of exposure in gestation. Isotretinoin taken as an oral medica- susceptible subgroup of mothers or fetuses. tion is one of the most potent known human teratogens. Exposure to For example, women with infants who have cleft lip with or without isotretinoin limited to as little as a few days in early pregnancy results cleft palate or isolated cleft palate are approximately twice as likely to in an approximate 20% risk of a pattern of brain, heart, ear, and report heavy first-trimester tobacco use than are mothers of normal thymus abnormalities and mental deficiency in liveborn children.20 In newborns; however, women who have a certain transforming growth contrast, topical retinoids, when used sparingly in the first trimester factor-α (TGF-α) polymorphism and who smoke heavily have a 3 to for blemishes or to reduce signs of skin aging, have not been associated 11 times higher risk of having a child with an oral cleft, suggesting a with a measurably increased risk for the same pattern of adverse gene-environment interaction. Furthermore, this risk appears to be effects.21,22 These findings do not rule out the teratogenic potential of lessened by maternal multivitamin use.13,14 Similarly, a low level of topical retinoids but simply suggest that the maternal blood levels of epoxide hydrolase enzyme activity influenced by epoxide hydrolase retinoids delivered via skin absorption may represent a teratogenic risk polymorphisms has been implicated as a risk factor for fetal hydantoin that is so low as to be undetectable without very large sample sizes. syndrome in children whose mothers have taken phenytoin for the The principle of spectrum of outcomes indicates that, depending on treatment of a seizure disorder during pregnancy.15 dose and timing in gestation, adverse outcomes associated with a given The principle of gestational timing, or critical developmental teratogen may encompass effects ranging from spontaneous abortion windows of exposure, requires that the exposure occur during the stage or stillbirth to major and minor structural defects, prenatal or postna- in development when the maturational process is most susceptible. For tal growth deficiency, preterm delivery, and functional deficits or learn- example, the critical window for an agent that interferes with closure ing disabilities. For example, moderate to heavy maternal alcohol of the neural tube in the human embryo is approximately the first intake, particularly if consumed in a “binge” pattern, has been demon- 3 weeks after conception. Carbamazepine, an anticonvulsant linked strated to increase the risks for spontaneous abortion, stillbirth, a to a 10-fold increased risk for neural tube defects, does not produce characteristic pattern of minor craniofacial abnormalities, selected the defect if maternal exposure occurs after the second month of specific major structural defects including heart defects and oral clefts, pregnancy.16,17 prenatal and postnatal growth deficiency, deficits in global IQ, and A corollary to this principle is that, depending on the precise ges- specific behavioral and learning abnormalities.23 Animal and human tational timing of teratogenic exposure, a range of adverse outcomes studies consistently support the notion that the entire spectrum of may be induced. For example, coumarin-derived anticoagulants are outcomes associated with alcohol may not be manifested in any single associated with a pattern of nasal hypoplasia and skeletal abnormalities affected pregnancy; rather, the results vary by dose and pattern of when prenatal exposure occurs during a critical window in the latter drinking, differ with gestational timing of exposure, and are influenced
- 3. CHAPTER 20 Teratogenesis and Environmental Exposure 349 by genetic susceptibility and other modifying factors such as maternal potential for human teratogenicity. For almost all known human nutrition. teratogens, there is an animal model; however, animal studies are not Finally, the principle of specific mechanisms leading to pathogenesis completely predictive of human pregnancy outcomes due to species specifies that teratogenic agents do not increase the risk of all adverse sensitivity and differences in dosing and exposure timing. outcomes; rather, they act on specific targets to produce a characteristic pattern of effects. This principle underlies the methods by which many human teratogens have been recognized; that is, a pattern of abnor- Adverse Case Reports malities associated with a particular teratogenic exposure helps to When new medications are marketed in the United States, initial identify that exposure as a cause of the outcome. For example, the reports of pregnancy exposures with adverse outcomes may appear as characteristic pattern of abnormalities comprising the fetal alcohol case reports in the literature, or through safety data provided to the syndrome includes minor craniofacial features (short palpebral fis- FDA by manufacturers, or in voluntary reports by clinicians or patients. sures, smooth philtrum, and thin vermilion of the upper lip) accom- Although individual adverse outcome reports have the potential to panied by microcephaly, growth deficiency, and cognitive and generate a hypothesis regarding teratogenicity—especially if the behavioral deficits. The prenatal effects of alcohol, although pervasive, outcome reported is an unusual pattern of malformation—these data nevertheless represent a constellation or pattern of features that is sources lack critical information about the number of exposed preg- unlikely to randomly occur without exposure to alcohol in substantial nancies with normal outcomes and therefore can confuse the process doses and during certain gestational weeks. of determining whether the adverse event reports represent an excess It therefore appears likely that there are a few general mechanisms risk over the baseline for that event. that lead to abnormal development. For example, a teratogenic agent can interact with a receptor, bind to DNA or protein, degrade cell membranes or proteins, inhibit an enzyme, or modify proteins. These Pregnancy Registries mechanisms ultimately manifest as one or more types of abnormal Additional sources of pregnancy safety information on new drugs embryogenesis, including excessive or reduced cell death, failed cell sometimes include pregnancy registries. Registries typically collect interactions, reduced biosynthesis, impeded morphogenetic move- data regarding exposures to a specific drug or class of drugs, both ment, or mechanical disruption of tissues. For this reason, several retrospectively and prospectively. The outcome of primary interest in specific teratogens may have the same end result on development by traditional pregnancy registries is major birth defects. Registry data are acting through a common pathway. For example, some anticonvul- periodically summarized and reviewed for possible “signals” that might sants, trimethoprim, and triamterine may increase the risk for neural lead to recommendations for initiation of a hypothesis-testing study. tube defects via folate antagonism.24 Angiotensin I–converting enzyme Strengths of registries include their potential for gathering early infor- (ACE) inhibitors such as enalapril and lisinopril may induce the mation about a new drug and the possibility of identifying a unique risk for ACE-inhibitor fetopathy, which consists of renal tubular pattern of malformation that is associated with exposure to the drug dysplasia and hypocalvarium, possibly through the mechanism of interest. However, traditional registries lack formal comparison of drug-induced fetal hypotension leading to hypoperfusion and groups and typically have outcome data on relatively small numbers oligohydramnios.25 of pregnancies. As a result, they usually have insufficient sample size to detect increased frequencies of specific and relatively rare birth defects.26 Nevertheless, collaborative registry designs such as the Antiepileptic Drugs in Pregnancy Registry have demonstrated success Sources of Safety Data on in identifying signals or establishing higher than expected rates for Exposures in Pregnancy major birth defects after selected exposures.27 In the ideal world, clinicians would have access to complete informa- tion about the human teratogenic potential of all environmental expo- Observational Cohort Studies sures, including medications, recreational drugs, nutrients and nutrient Another source of pregnancy safety data originates from observational supplements, occupational exposures, toxic exposures or poisonings, cohort studies that are initiated with the goal of testing a specific household chemicals and cosmetics, environmental contaminants or hypothesis. These include prospectively designed exposure cohort pollutants, and physical agents such as heat and radiation. Unfortu- studies in which women with and without the exposure of interest are nately, for many if not most exposures, reliable information is limited. enrolled during pregnancy and followed to outcome. Such studies have Sufficient human data are commonly lacking for even prescription the ability to evaluate a spectrum of outcomes, including major and medications whose safety is monitored by the FDA. In one study minor malformations, and to collect early information on a new drug. reviewing the human safety data for prescription medications mar- They also have the advantage of including a comparison group or keted in the United States over the previous 20 years, Lo and Friedman8 groups, allowing for the control of key factors that may be confound- concluded there were insufficient data to confirm or rule out terato- ers, such as maternal age, socioeconomic status, and alcohol or tobacco genicity for more than 80% of these agents. use. Such a study design was successful identifying carbamazepine as There are many reasons for this situation, some inherent to the a human teratogen.28 One disadvantage of this approach is that the difficulty of conducting pregnancy outcome research and some related sample sizes are typically too small to rule out anything but the most to the lack of a standard surveillance system for studying agents to dramatically increased prevalence of specific major birth defects. which women of reproductive age are likely to be exposed. Clinical trials for prescription medications are not typically conducted in human pregnancy, and the pharmaceutical industry has no incentive Database Cohorts to do so even when there is an apparent clinical need. Animal repro- A variation of the observational cohort involves construction of an ductive and developmental toxicity studies are used to estimate the historical cohort using archived information in existing databases. For
- 4. 350 CHAPTER 20 Teratogenesis and Environmental Exposure example, health maintenance organization claims data and records TABLE 20-1 FDA PREGNANCY CATEGORIES from government-supported healthcare agencies are increasingly being analyzed for information on pregnancies with or without specific Category Definition medication exposures. The strengths of this approach include the A Adequate and well-controlled studies have failed to potential cost savings for collecting data for a given number of preg- demonstrate a risk to the fetus in the first trimester nancies, but the limitations include sample sizes that are too small to of pregnancy (and there is no evidence of risk in detect increased risks for many, if not most, specific birth defects. In later trimesters). addition, because database studies rely on information not collected B Animal reproduction studies have failed to primarily for research purposes, validation of exposure and outcome, demonstrate a risk to the fetus and there are no as well as data on some key potential confounders, may be difficult or adequate and well-controlled studies in pregnant impossible to obtain. Nevertheless, database cohorts have been used, women. for example, to identify a possible link between paroxetine and con- C Animal reproduction studies have shown an adverse effect on the fetus and there are no adequate and genital heart defects.29 well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks. Case-Control Studies D There is positive evidence of human fetal risk based In case-control study designs, pregnancies are retrospectively selected on adverse reaction data from investigational or for having a specific outcome, such as a particular birth defect. The marketing experience or studies in humans, but frequency of exposure to an agent of interest among mothers of potential benefits may warrant use of the drug in affected infants is compared with the frequency among mothers whose pregnant women despite potential risks. pregnancies did not result in that birth defect. A major strength of X Studies in animals or humans have demonstrated fetal case-control studies is that, with proper numbers of cases and controls, abnormalities and/or there is positive evidence of human fetal risk based on adverse reaction data they can provide sufficient power to detect increased risks for rare from investigational or marketing experience, and outcomes. In addition, because they include a comparison group, they the risk involved in use of the drug in pregnant can collect information on important potential confounding variables women clearly outweighs potential benefits. such as age, socioeconomic status, and alcohol and tobacco use. The case-control approach was used successfully to identify the association of misoprostol (used to induce abortion) with a very high risk for a rare congenital facial nerve paralysis, Möbius syndrome.30 Limitations associated with prescription drugs. However, this category system is to case-control studies include the lag time inherent in collecting infor- frequently misunderstood by health care providers and patients alike. mation on a new drug, especially if it is infrequently used by pregnant The categories are summarized in Table 20-1. women. Another limitation is the inability to evaluate an agent for In practice, the FDA category assigned to a medication often mis- a spectrum of outcomes that are as yet unidentified as part of represents or oversimplifies the actual evidence. For example, the the anomaly pattern. Finally, it is possible that women who are category assignments do not take into consideration factors such as already aware of a negative outcome of their pregnancy may recall exposure timing in gestation or dose and route of administration. exposures more carefully (or incorrectly) than those who had a normal Although several drugs assigned to category X (i.e., contraindicated in outcome. pregnancy) are indeed known human teratogens (e.g., isotretinoin), others, such as ribavirin and the “statins,” were assigned to that cate- gory based on theoretical concerns or animal data without conclusive Summary of Data Sources human data to establish a teratogenic risk.32 Further, incorporation of In summary, the strengths and weaknesses of the methodologies that new data into the label and classification updates is often slow. are available to evaluate for potential teratogenicity reveal that no Communication of potential risk to a woman regarding a category single approach is sufficient. From the clinical perspective, this means X exposure that has already taken place varies substantially from that that conclusions drawn from one type of study must be interpreted for an exposure that is anticipated. An example is the communication with caution until they are either confirmed or refuted by other types of information regarding risk from an exposure to ribavirin (to treat of studies. This is especially important in recognizing high-risk expo- hepatitis C) that occurred during an unplanned pregnancy compared sures (and perhaps even more so for identifying agents that are not with the communication of concern if the clinician and patient are teratogenic), so that appropriate treatment decisions can be made. prospectively determining whether ribavirin is an appropriate medica- From a public health perspective, a combination of complementary tion to use. Such nuances are not reflected in the category statements. study designs is required, one that ideally is initiated in a coordinated, In recognition of these limitations and weaknesses, the FDA has worked systematic fashion so as to provide clinicians and patients with the best with an advisory committee to develop recommended revisions to the and earliest possible information.31 category system and the label format.33 Other sources of information readily available to the clinician include a number of print resources, each with different approaches to providing summary information. Some of these references are avail- Risk Assessments able in hard copy, compact disk (CD-ROM), and personal digital assis- and Resources tant (PDA) versions.34,35 Online databases that provide summary statements prepared by experts in the field of teratology and updated The U.S. FDA established a widely used pregnancy safety category on a frequent basis include TERIS and REPROTOX (available at system that is incorporated into the product label with the intent of http://www.micromedex.com/reprorisk [accessed January 14, 2008]). informing clinicians and pregnant women of the teratogenic risks In addition, the Organization of Teratology Information Specialists
- 5. CHAPTER 20 Teratogenesis and Environmental Exposure 351 (OTIS) provides individualized information to clinicians as well as the radiographs, and growth restriction. Central nervous system (CNS) public via toll-free telephone access (see http://otispregnancy.org and eye abnormalities including microcephaly, hydrocephalus, Dandy- [accessed January 14, 2008]). Clinicians or patients who are interested Walker malformation, agenesis of the corpus callosum, optic atrophy, in pregnancy registries that are open for enrollment can locate a cataracts, and mental retardation occur occasionally.36,37 The critical current list at the FDA’s Office of Women’s Health Web site (avail- period for the warfarin embryopathy appears to be between 6 and 9 able at http://www.fda.gov/womens/registries [accessed January 14, weeks’ gestation. A systematic review of 17 studies involving a total of 2008]). 979 exposed pregnancies estimated a 6% incidence of warfarin embry- opathy. In addition, 22% of exposed pregnancies ended in spontaneous abortion, 4% in stillbirth, and 13% in preterm delivery.38 A large Selected Human Teratogens multicenter study of 666 pregnancies with exposure to vitamin K antagonists reported a significant increase in the rate of major birth Table 20-2 presents the potential effects of selected human teratogens, defects overall, relative to unexposed healthy comparison women some of which are discussed further in the following sections. (odds ratio [OR], 3.86; 95% confidence interval [CI], 1.76 to 8.00). In that study, only 2 infants (0.6%) were thought to have warfarin embry- opathy. In addition, the rate of preterm delivery was increased (16.0% Vitamin K Antagonists versus 7.6%; OR, 2.61; CI, 1.76 to 3.86); the mean birth weight of term A specific pattern of congenital anomalies referred to as the fetal war- infants was significantly lower (3166 versus 3411 g); and the rate of farin syndrome has been identified in some children born to mothers spontaneous abortion was significantly higher (42% versus 14%; OR, who use medications such as phenprocoumon, acenocoumarol, fluin- 3.36; CI, 2.28 to 4.93) with exposure.18 dione, warfarin, and phenindione, which are vitamin K antagonists. In one study of 71 pregnancies occurring in 52 women with pros- The features include nasal hypoplasia, stippled epiphyses visible on thetic heart valves who were being treated with warfarin, the risk for TABLE 20-2 EFFECTS OF SELECTED TERATOGENS Drug Potential Effects Comments ACE inhibitors Calvarial hypoplasia, renal dysgenesis, oligohydramnios, IUGR, Risk seen with use in second and third and neonatal renal failure trimester Alcohol Syndrome: prenatal and postnatal growth restriction, Risk not limited to first trimester; late microcephaly, craniofacial dysmorphology (1-4/1000 live pregnancy use is associated with IUGR and births); renal, cardiac, and other major malformations developmental delay; incidence is 4-44% increased among “heavy drinkers” Antidepressants (SSRIs) Possible cardiac defects, NTDs, omphalocele; neonatal — pulmonary hypertension and withdrawal syndrome Aminopterin and Syndrome: calvarial hypoplasia, craniofacial abnormalities, limb Syndrome associated with methotrexate methotrexate defects; possible developmental delay >10 mg/wk Androgens and Masculinization of external female genitalia Labioscrotal fusion can occur with exposure; norprogesterones as many as 50% of those exposed are affected Carbamazepine NTDs (1%); possible facial hypoplasia and developmental delay — Corticosteroids Cleft lip/palate increased threefold to sixfold; IUGR increased — with high doses Diethylstilbestrol Clear cell adenocarcinoma of the vagina, vaginal adenosis, — abnormalities of the cervix and uterus, testicular abnormalities, male/female infertility Isotretinoin Syndrome: CNS malformations, microtia/anotia, micrognathia, — thymus abnormalities, cleft palate, cardiac abnormalities, eye anomalies, limb reduction defects (28%); miscarriage (22%), developmental delay (47%) Lithium Small increase in Ebstein cardiac anomaly — Penicillamine Cutis laxa with chronic use — Phenytoin Syndrome: IUGR, microcephaly, facial hypoplasia, hypertelorism, Full syndrome in 10%; up to 30% exhibit prominent upper lip (10%); possible developmental delay some features Streptomycin Hearing loss, eighth nerve damage — Tetracycline Discoloration of deciduous teeth and enamel hypoplasia Risk only in second and third trimester Tobacco Oral clefts: relative risk, 1.22-1.34; IUGR, IUFD, abruption — Trimethadione Syndrome: oral clefts, craniofacial abnormalities, developmental — delay (80%) Valproic acid NTDs (1-2%); facial hypoplasia, possible developmental delay — Warfarin Syndrome: nasal hypoplasia, stippled epiphyses, growth Greatest risk is at 6-9 wk restriction (6%); also increased microcephaly, Dandy-Walker syndrome, IUGR, preterm birth, mental retardation ACE, angiotensin-converting enzyme; CNS, central nervous system; IUGR, intrauterine growth restriction; NTD, neural tube defect.
- 6. 352 CHAPTER 20 Teratogenesis and Environmental Exposure adverse outcome was found to be significantly greater with doses Carbamazepine greater than 5 mg/day.39 A review of 85 pregnancies involving exposure Similar to valproic acid, carbamazepine has been associated with an to a coumarin drug only after the first trimester reported that 1 preg- increased risk for spina bifida (approximately 1%) with exposure in nancy ended in stillbirth, 3 in spontaneous abortion, and 19 in preterm the early first trimester.16 It has also been linked to a pattern of minor births; 1 infant had a CNS anomaly, and none had the warfarin embry- craniofacial abnormalities, including upslanting palpebral fissures, a opathy.38 In addition, in one large study that evaluated the cognitive long philtrum, and nail hypoplasia, as well as growth deficiency and performance of 307 children prenatally exposed to warfarin, compared microcephaly.28 Although some small studies have suggested develop- with that of nonexposed children, mean IQ scores did not differ mental delay after prenatal exposure to carbamazapine,57 others have significantly, but low intelligence scores (IQ < 80) occurred more not.58,59 frequently in those children whose exposure was limited to the second and third trimester.40 Other Antiepileptic Drugs A number of newer antiepileptic medications have been introduced into practice over the past several years, including lamotrigine, gaba- Antiepileptic Drugs pentin, and topiramate. Although these agents are currently being As a group, most older drugs used to treat seizure disorders are as- studied, insufficient information has been collected to rule out or sociated with an increase in the risk of congenital malformations.41,42 identify risks similar to those seen with older anticonvulsants. Further- This has been suggested to indicate that the underlying disease is the more, specific risks associated with the use of older- and newer- teratogenic cause. Newer studies have challenged this concept42-44; generation anticonvulsants for other indications, such as treatment however, it is difficult to separate the effects of the disease from those of mood disorders, has not been well studied. of treatment, especially for more severe epilepsy, which is unlikely to be untreated during pregnancy. The use of multiple anticonvulsant medications (polytherapy) as opposed to a single drug (monotherapy) is associated with greater risk of structural defects.43,45,46 It is unclear Chemotherapeutic and whether this is a result of drug-drug interactions, more severe disease Immunosuppressive Agents in women requiring treatment with polytherapy, or a combination of the two. Cyclophosphamide Eight case reports documenting a unique pattern of malformation in Diphenylhydantoin infants prenatally exposed to cyclophosphamide have been published.60 Phenytoin as a treatment for seizure disorders has been associated with Features include growth deficiency, craniofacial anomalies, and absent an increased risk for oral clefts and for a pattern of anomalies known fingers and toes. In three of these cases, the infant survived and devel- as the fetal hydantoin syndrome. This pattern is estimated to occur in opmental information was available; significant delays were noted in 10% of infants with prenatal exposure and includes prenatal or post- all three. The magnitude of the risk is unknown. natal growth restriction, microcephaly, hypoplasia of the digits and nails, and craniofacial abnormalities (i.e., short nose with low nasal Methotrexate bridge, ocular hypertelorism, abnormal ears, and a wide mouth with Both aminopterin and its methyl derivative, methotrexate, have a prominent upper lip).47-49 Initial reports suggested that mental defi- been associated with a specific pattern of malformation that includes ciency was also a common feature of fetal hydantoin syndrome.50 prenatal-onset growth deficiency, severe lack of calvarial ossification, However, the limited subsequently published data suggest that neu- hypoplastic supraorbital ridges, small low-set ears, micrognathia, limb robehavioral effects may be more mild.51 For example, Scolnik and abnormalities, and, in some cases, developmental delay.61,62 The major- colleagues52 reported that average IQ scores were 10 points lower in ity of affected infants have been born to women treated with high-dose children exposed to phenytoin monotherapy, compared with unex- methotrexate for psoriasis or neoplastic disease or as an abortifacient. posed children born to mothers who were matched on age and socio- Although the magnitude of the risk is unknown, it has been suggested economic status. that the dose necessary to produce the aminopterin/methotrexate syn- drome is greater than 10 mg/wk.63,64 Valproic Acid Studies over the last 2 decades have associated early first-trimester exposure to valproic acid with an increased risk for neural tube defects, specifically spina bifida. The estimated risk is about 1% to 2%, with Adrenal Corticosteroids higher doses thought to be associated with higher risk.19,53 It has been Among four recent case-control studies, three concluded that systemic estimated that the overall risk for major birth defects is increased by corticosteroid use in the first trimester appears to be associated with a fourfold to sevenfold after valproate monotherapy, with increased risks threefold to sixfold increased risk for cleft lip with or without cleft for specific cardiovascular, limb, and genital anomalies noted in some palate and possibly cleft palate alone.65-68 It is unclear to what extent reports.27 As with other anticonvulsants, a pattern of minor malforma- this association was caused by the various underlying maternal diseases tions and growth deficiency has also been identified for valproic acid; involved in these studies. If only the positive studies are considered, it includes midface hypoplasia, epicanthal folds, short nose, broad this relative risk translates to a risk of approximately 3 to 6 cases per nasal bridge, thin upper lip, thick lower lip, micrognathia, and subtle 1000 pregnancies exposed in the critical period for lip and palate limb defects (primarily hyperconvex fingernails).54 In addition, there closure. Furthermore, an association has long been recognized between is some evidence that valproic acid monotherapy is associated with prenatal exposure to corticosteroids and intrauterine growth restric- reduced cognitive ability and additional educational needs in children tion in humans. The risk appears to be dose-related, suggesting that prenatally exposed.55,56 this concern can be minimized with lower doses.69,70
- 7. CHAPTER 20 Teratogenesis and Environmental Exposure 353 craniosynostosis (adjusted OR, 2.5; CI, 1.5 to 4.0), and omphalocele Antihypertensive Medications (adjusted OR, 2.8; CI, 1.3 to 5.7).78 A second large, multisite, case- control study did not confirm these findings with respect to cranio- Angiotensin I Converting Enzyme synostosis, omphalocele, neural tube defects, or cardiac defects when (ACE) Inhibitors and Angiotensin II all SSRIs were evaluated as a group but did find significantly increased Receptor Antagonists risks with specific drugs. With first-trimester sertraline use, the odds Based on case reports and case series, prenatal exposure to an ACE were increased for omphalocele (adjusted OR, 5.7; CI, 1.6 to 20.7) and inhibitor (benazepril, captopril, enalapril, enalaprilat, fosinopril, lisin- septal defects (adjusted OR, 2.0; CI, 1.2 to 4.0).79 With first-trimester opril, moexipril, quinapril, ramipril) or to an angiotensin II receptor paroxetine use, the odds were increased for right ventricular outflow antagonist (losartan, candesartan, valsartan, tasosartan, telmisartan) tract obstruction defects (adjusted OR, 3.3; CI, 1.3 to 8.8). during the second or third trimester of pregnancy is associated with In addition to these findings with respect to structural defects, an increased risk for fetal hypotension, renal failure, and oligohydram- several other adverse outcomes have been associated with late preg- nios leading to fetal growth restriction, joint contractures, pulmonary nancy exposure to SSRIs. These include a possible small increased hypoplasia, and stillbirth or neonatal death. Calvarial hypoplasia has risk for persistent pulmonary hypertension of the newborn80 and a also been reported as part of the fetopathy. In children who survive the well-established increased risk for a neonatal withdrawal or toxicity neonatal period, renal insufficiency often occurs. The magnitude of the syndrome consisting primarily of CNS, motor, respiratory, and risk after second- or third-trimester exposure is not known.25,71 gastrointestinal signs that are generally mild and resolve by 2 weeks First-trimester exposure to ACE inhibitors or to angiotensin II of age.81 receptor antagonists has not been well studied. One recent database linkage study suggested an increased risk for cardiovascular defects (risk ratio [RR], 3.72; CI, 1.89 to 7.30) and CNS defects (RR, 4.39; CI, Retinoids 1.37 to 14.02) in infants born to mothers who had received a prescrip- tion for an ACE inhibitor in the first trimester of pregnancy, compared Vitamin A (Retinol) with infants born to women with no exposure to antihypertensive The teratogenic potential of excessive doses of preformed vitamin A is medications during pregnancy. However, these findings have not yet well described in animal models82,83; however, the threshold dose at been replicated, and it is possible that they were confounded by inabil- which naturally occurring vitamin A might be teratogenic in humans ity to completely control for maternal diabetes.72 remains controversial. Two studies suggested that preformed vitamin A supplementation at amounts greater than 10,000 IU per day in the first trimester of pregnancy is associated with a small increased risk of Psychotherapeutic Medications selected defects that are consistent with those known to be induced by synthetic retinoids.84,85 However, other studies did not confirm these Lithium findings or suggested that the elevated risk is concentrated at doses Early reports from a lithium exposure registry73 included information greater than 40,000 IU per day.86-88 The current recommended daily on 143 infants exposed to lithium in utero; 13 of these were reported allowance (RDA) for pregnant women carrying a single fetus is 2560 IU to have malformations, 4 of which were Ebstein anomaly (downward of vitamin A. To avoid any of these potential concerns, many prenatal displacement of the tricuspid valves within the right ventricle). This vitamin formulations have replaced retinol with β-carotene. finding represented an excess over expected numbers, because the baseline incidence of Ebstein anomaly is approximately 1 in 20,000 Isotretinoin and Other Oral Synthetic Retinoids births. A subsequent prospective cohort study involving follow-up of Consistent with animal data, an increased risk of pregnancy loss 148 women with first-trimester exposure to lithium noted one case of and a characteristic pattern of malformations and mental deficiency Ebstein anomaly, with no other cardiac malformations identified in the have been identified after prenatal exposure to isotretinoin. This sample.74 In contrast, a case-control study published by Zalzstein and pattern includes CNS malformations, microtia/anotia, micrognathia, associates75 found no prenatal exposure to lithium among 59 patients cleft palate, cardiac and great vessel defects, thymic abnormalities, eye with Ebstein anomaly. In summary, the available data suggest that, if anomalies, and, occasionally, limb reduction defects.20,89 The estimated there is a risk at all, the use of lithium in the first trimester of pregnancy risks are at least as high as 22% for spontaneous abortion, 28% for is associated with a very small increased risk for Ebstein anomaly. structural defects, and 47% for mild to moderate mental deficiency, even if no structural abnormalities are present.20,90,91 Affected children Selective Serotonin Reuptake Inhibitors have been reported with exposures to usual therapeutic doses and with Although medications within the selective serotonin reuptake inhibi- treatment for durations shorter than 1 week in the first trimester. There tor (SSRI) class of antidepressants (fluoxetine, paroxetine, sertraline, does not appear to be a risk of malformations when the drug is dis- citalopram, escitalopram, fluvoxamine) have been studied extensively continued before conception, which is consistent with the half-life of in pregnancy, most investigations have had insufficient sample sizes to isotretinoin.92,93 Pregnancy prevention among women who are pre- rule out increased risks for specific malformations associated with scribed isotretinoin continues to be a challenge. A third-generation individual medications. Several recent studies have suggested a small restricted distribution program, iPledge, was implemented in March increased risk for cardiac defects (approximately twofold) specifically 2006; it mandates close monitoring of birth control practices and with first-trimester exposure to paroxetine.76,77 One recent large, mul- negative pregnancy testing before dispensing of prescriptions for tisite, case-control study did not find an overall increase in cardiac isotretinoin. defects but found increased risks for other selected malformations in Risks for the retinoid embryopathy are also found with other oral association with first-trimester use of all SSRIs combined. These spe- synthetic retinoids such as etretinate and its metabolite, acitretin, cific defects included anencephaly (adjusted OR, 2.4; CI 1.1 to 5.1), which are used for the treatment of psoriasis.94 The extremely long
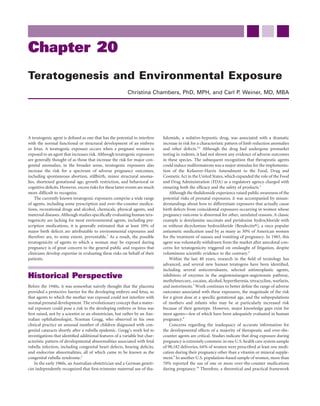
- 8. 354 CHAPTER 20 Teratogenesis and Environmental Exposure half-life of etretinate led to its removal from the U.S. market in 1998. The half-life of acitretin is considerably longer than that of isotretinoin (50 to 60 hours), and it can be converted to etretinate with maternal ingestion of alcohol. Therefore, the drug must be discontinued before pregnancy, and alcohol must be avoided during the entire period of treatment and for at least 2 months after discontinuation of therapy.95,96 Ionizing Radiation Prenatal exposure to high-dose radiation is associated with an increased risk of microcephaly, mental deficiency, and growth deficiency based on data derived from a small number of pregnant survivors of the atomic bombs in Nagasaki and Hiroshima.97 It is estimated that doses of 50 rad (50 cGy) or greater to the uterus are required to produce these effects. The highest risk appears to be associated with exposures between 8 and 15 weeks’ gestation, with a higher threshold dose at more advanced gestational ages.98 The available data do not support an increase in the risk of mental retardation associated with high-dose radiation exposure beyond 25 weeks or before 8 weeks of gestation.97 Based on dose-response calculations, it is not thought that diagnostic procedures involving radiation have the potential to pose a risk to the fetus unless the cumulative dose to the uterus is greater than 10 cGy; conservative guidelines suggest that doses should be kept below 5 cGy to the uterus during pregnancy if radiation exposure is required.99 Environmental Agents FIGURE 20-1 Nine-month-old infant with fetal alcohol syndrome. (From Streissguth AP, Aase JM, Clarren SK, et al: Fetal Methylmercury alcohol syndrome in adolescents and adults. JAMA 265:1961, 1991. Prenatal exposure to methylmercury has been recognized as a neuro- Copyright 1991, American Medical Association.) developmental teratogen since the experience of environmental contaminations in Japan (Minamata Bay) and Iraq in the mid-20th century.100,101 The reported effects, termed fetal methylmercury syn- drome or congenital Minamata disease, include cerebral palsy and a Social and Illicit Drugs variety of neurologic and functional problems as well as mental defi- ciency.102 Although the lower limit of exposure that may pose a risk in Alcohol prenatal development remains controversial, an independent U.S. A pattern of anomalies, known as the fetal alcohol syndrome (FAS), was National Research Council expert committee concluded that limiting first described more than 35 years ago in a case series of infants born maternal intake to no more than 0.1 μg/kg/day was sufficient to protect to alcoholic women.111 The characteristic features of this disorder are the fetus.103 Currently, consumption of contaminated fish or marine prenatal and/or postnatal growth retardation, microcephaly or other mammals is the major source of methylmercury exposure in most CNS dysfunction including neurobehavioral deficits and neurologic populations. The U.S. Environmental Protection Agency and FDA have impairment, and characteristic facial anomalies consisting of short advised pregnant women and women of childbearing age who may palpebral fissures and a smooth philtrum, with a smooth, thin vermil- become pregnant to avoid eating shark, swordfish, king mackerel, and ion border of the upper lip (Fig. 20-1).112,113 Although FAS is difficult tilefish and to limit their average consumption of other cooked fish to to diagnose, particularly in the newborn period, estimates of its inci- 12 ounces (340 g) per week in order to prevent fetal exposure to exces- dence in selected U.S. and Western European populations are approxi- sive amounts of methylmercury.104 Similarly, limiting tuna consump- mately 1 to 4 per 1000 live births.114 tion to no more than three servings per week is recommended because Many more children are thought to have alcohol-related neurobe- of methylmercury concerns. havioral or neurologic impairment with or without some structural features. In addition, congenital heart defects, oral clefts, and abnor- Lead malities of the eyes, brain, and kidneys are more common than expected In utero exposure to very high levels of lead (maternal blood concen- among the children of women who drink moderately to heavily during trations >30 μg/dL) has been associated with an increase in spontane- pregnancy.115-118 These children, variably described as having partial ous abortion, preterm birth, and mental deficiency.105,106 Prenatal FAS, alcohol-related neurodevelopmental abnormalities (ARND), or exposure to lower levels (>10 μg/dL) may be associated with subtle alcohol-related birth defects (ARBD), are now thought of as represent- neurobehavioral effects; however, these effects may not persist into ing a continuum known as fetal alcohol spectrum disorders (FASD). older childhood.107-109 Occupational and environmental exposures to Accurate estimates of the prevalence of FASD are lacking; however, one lead that precede pregnancy may result in fetal exposure due to mobi- population-based study in the Seattle, Washington, area suggested lization of lead stored in maternal bone. These effects may be modified that the rates may be as high as 1 per 100 children.114 Increased risks by maternal intake of calcium.110 for spontaneous abortion, stillbirth, and sudden infant death syn-
- 9. CHAPTER 20 Teratogenesis and Environmental Exposure 355 drome have also been linked to prenatal alcohol exposure, particularly 700 exposure from alcohol consumed in a heavy episodic or binge pattern.119-122 Both animal and human data support a dose-response relation in Umbilical blood flow 600 terms of risk for FAS/FASD. However, because of variabilities in diag- (mL/min) nosis and difficulties in obtaining and validating exposure information reported by pregnant women, estimates vary widely regarding the 500 magnitude of the risk. For example, estimates for the full-blown syn- drome range from about 4% to 44% of children born to women who drink heavily during pregnancy.123,124 The women at highest risk appear 400 to be those who have already had an affected child and who continue to consume alcohol in subsequent pregnancies. Lower levels of mater- 300 nal alcohol consumption have been associated with less severe neu- Umbilical vascular resistance robehavioral outcomes and persistent growth effects.125-127 However, the exact threshold doses and patterns of consumption for these effects 0.175 are not well understood. For example, full-blown FAS is typically seen (mm Hg/mL) among the children of women who report consuming an average of 0.150 six or more standard drinks (beer, wine, or spirits) per day during pregnancy. However, some studies have suggested that women who 0.125 consume more than two standard drinks per day during pregnancy are at increased risk. These risks may be mediated or ameliorated by 0.100 the pattern of drinking (i.e., binge drinking versus more frequent and lesser quantities), maternal age, nutrition, and genetic susceptibil- 0.075 ity.118,128-130 Furthermore, the duration of exposure is likely to be impor- Saline 10 20 30 tant, in that CNS development continues throughout gestation.131 Dose of nicotine At present, the data are insufficient to assign a risk to certain (μg/kg/min) common patterns of prenatal alcohol exposure, such as alcohol con- sumption limited to occasional binge episodes before recognition of FIGURE 20-2 Umbilical blood flow and umbilical vascular pregnancy. However, the data do support the notion that reduction or resistance response to maternally administered discontinuation of alcohol consumption at any point in pregnancy nicotine. Maternal administration produced a decrease in umbilical may be beneficial. A lower threshold of exposure, below which no blood flow from a baseline of 554 ± 37 to 449 ± 52 mL/min, which effects will be seen, has not been defined. Therefore, for those women was significant only at the 30 μg/kg/min dose (P < .05). Umbilical who are planning pregnancy or who have the potential to become vascular resistance increased from a baseline of 0.110 ± 0.013 to pregnant, the U.S. Surgeon General has recommended that the safest 0.161 ± 0.020 mm Hg/mL, which was significant only at the 30 μg/kg/ course is to avoid alcohol entirely during pregnancy.132 min dose (P < .05). For the 20 μg/kg/min dose, n = 6. For saline solution and all other doses, n = 8. (From Clark KE, Irion GL: Fetal hemodynamic response to maternal intravenous nicotine Tobacco administration. Am J Obstet Gynecol 167:1624, 1992.) Maternal cigarette smoking is associated with a variety of harmful effects on the embryo and fetus, including increased risks for specific congenital malformations, spontaneous abortion, placental complica- tions, preterm delivery, reduced birth weight, and sudden infant death The deleterious effects of cigarette smoking on other pregnancy syndrome. The structural malformations that have been significantly outcomes are well documented. Intrauterine growth restriction is the associated with first-trimester smoking include oral clefts and gastro- most consistently reported adverse outcome. On average, babies born schisis. A recent meta-analysis of 24 studies estimated the risk for oral to women who smoke during pregnancy are 200 g lighter than those clefts to be low: the relative risk for cleft lip with or without cleft palate born to comparable women who do not smoke, with a clear dose- was 1.34 (CI, 1.25 to 1.44), and for cleft palate alone it was 1.22 (CI, response gradient.141 This may be a result, in part, of the reduction in 1.10 to 1.35).133 Some studies have suggested gene-environment inter- uterine blood flow associated with rising levels of plasma nicotine in actions in susceptibility for oral clefts when mothers smoke during women who smoke (Fig. 20-2).142 Lesser reductions in birth weight early pregnancy. Infants who have a null deletion of the detoxifying have also been noted when exposure is limited to environmental gene GSTT1, or infant genotype at the Taq1 site for transforming or passive smoke.143 A strong gene-environment and gene-gene– growth factor-α and whose mothers smoke are at higher risk for environment interaction has been demonstrated between the cyto- certain oral clefts than infants with either risk factor alone.134,135 The chrome P450 isozyme CYP1A1 and GSTT1 maternal metabolic genes elevated risks for gastroschisis after maternal smoking are also esti- and infant birth weight in mothers who smoke.144 mated to be low.136 However, as with oral clefts, there is some evidence Perinatal mortality is also increased with maternal smoking, in part for gene-environment interaction between maternal smoking and because of the increased risks of placental complications and preterm polymorphisms of fetal genes involved in vascular response.137 Other delivery. In one large study, the combined risk for fetal or infant death defects reported to occur with increased frequency after pregnancy for primiparous women who smoked less than one pack per day was exposure to tobacco smoke include craniosynostosis and club estimated to be 25% higher than that for nonsmoking women, and the foot.138-140 Most studies with dose information available have suggested risk was 56% higher for those who smoked one pack per day or more.145 a dose-response relation for each of these defects, with the heaviest However, if smoking is discontinued in the first half of gestation, evi- smokers being at highest risk. dence indicates that the effects on birth weight can be eliminated.146-148
- 10. 356 CHAPTER 20 Teratogenesis and Environmental Exposure 2. Forrest JM, Turnbull FM, Sholler GF, et al: Gregg’s congenital rubella 35 patients 60 years later. Med J Aust 177:664, 2002. 33.33 3. McBride WG: Thalidomide and congenital abnormalities. Lancet 2:1358, 1961. 30 4. Lenz W: Diskussionbemerkung zu dem Vortrag von RA Pfeiffer and K Kosenow: Zur Frage der exogenen Entstehung schwere Extremitatens- 25 missbil-dungen. Tagung Rheinischwestful Kinderarztevere Dusseldorf 25.0 19:11, 1961. Premature birth (%) 5. Krantz JC: New drugs and the Kefauver-Harris amendment. J New Drugs 20 6:77, 1966. 6. Kutcher JS, Engle A, Firth J, et al: Bendectin and birth defects II: Ecological analyses. Birth Defects Res A Clin Molec Teratol 67:88, 2003. 15 7. Koren G, Pastuszak A, Ito S: Drugs in pregnancy. N Engl J Med 338:1128, 13.6 1998. 8. Lo WY, Friedman JM: Teratogenicity of recently introduced medications 10 11.36 in human pregnancy. Obstet Gynecol 100:465, 2002. 11.18 9. Andrade SE, Gurwitz JH, Davis RL, et al: Prescription drug use in preg- nancy. Am J Obstet Gynecol 191:398, 2004. 5 7.06 10. Werler MM, Mitchell AA, Hernandez-Diaz S, et al: Use of over-the-counter 6.39 medications during pregnancy. Am J Obstet Gynecol 193:771, 2005. 11. Wilson JG, Fraser FC (eds): Handbook of Teratology. Vol. 1: General 1–5 6–10 11–15 16–20 21–30 31 Principles and Etiology. New York, Plenum Press, 1977, pp 49-62. Number cigarettes per day 12. Fratta ID, Sigg EB, Maiorana K: Teratogenic effects of thalidomide in rabbits, rats, hamsters, and mice. Toxicol Appl Pharmacol 7:268, 1965. FIGURE 20-3 Dose-response relationship of cigarette smoking 13. Shaw GM, Wasserman CR, Lammer EJ, et al: Orofacial clefts, parental and prematurity. (From Simpson WJ: A preliminary report on cigarette smoking, and transforming growth factor-alpha gene variants. cigarette smoking and the incidence of prematurity. Am J Obstet Am J Hum Genet 58:551, 1996. Gynecol 73:808, 1957.) 14. Shaw GM, Wasserman CR, Murray JC, et al: Infant TGF-alpha genotype, orofacial clefts, and maternal periconceptional multivitamin use. Cleft Palate-Craniofac J 35:366, 1997. Furthermore, based on dose-response data, any reduction in the 15. Buehler BA, Delimont D, van Waes M, et al: Prenatal prediction of risk of number of cigarettes smoked may reduce risk for low birth weight, the fetal hydantoin syndrome. N Engl J Med 322:1567, 1990. preterm birth, and placental complications (Fig. 20-3).149-153 16. Rosa FW: Spina bifida in infants of women treated with carbamazepine during pregnancy. N Engl J Med 321:674, 1991. Cocaine 17. Matalon S, Schechtman S, Goldzweig G, et al: The teratogenic effect of Various structural defects have been reported in newborns prenatally carbamazepine: A meta-analysis of 1255 exposures. Reprod Toxicol 16:9, 2002. exposed to cocaine and are thought to be the result of intrauterine 18. Schaeffer C, Hanneman D, Meister R, et al: Vitamin K antagonists and vascular accidents; they include cavitary CNS lesions, genitourinary pregnancy outcome: A multi-centre prospective study. Thromb Haemost anomalies, terminal transverse limb reduction defects, and intestinal 95:949, 2006. atresia/infarction.154-157 In addition to these structural defects, an 19. Omtzigt JG, Los FJ, Grobbee DE, et al: The risk of spina bifida aperta after increased risk for placental abruption and premature rupture of mem- first-trimester exposure to valproate in a prenatal cohort. Neurology branes was documented in a systematic review.158 However, assessment 42:119, 1992. of the absolute risk for these outcomes after cocaine exposure is com- 20. Lammer EJ, Chen DT, Hoar RM, et al: Retinoic acid embryopathy. N Engl plicated by the fact that affected pregnancies often involve use of other J Med 313:837, 1985. drugs, tobacco, and alcohol as well as cocaine; the purity and dose of 21. Shapiro L, Pastuszak A, Curto G, et al: Safety of first-trimester exposure the drug is often not known, and multiple potential other confounding to topical tretinoin: Prospective cohort study. Lancet 250:1143, 1997. 22. Loureiro KD, Kao KK, Jones KL, et al: Minor malformations characteristic factors could be involved. of the retinoic acid embryopathy and other birth outcomes in children of The most consistently reported effects of prenatal cocaine exposure women exposed to topical tretinoin during early pregnancy. Am J Med are a small but statistically significant increase in intrauterine growth Genet A 136:117, 2005. restriction159,160 and abnormalities in neonatal state regulation and 23. Floyd RL, O’Connor MJ, Sokol RJ, et al: Recognition and prevention of motor performance.161 However, based on a synthesis of 36 published fetal alcohol syndrome. Obstet Gynecol 106:1059, 2005. studies of children 6 years of age or younger, Frank and colleagues162 24. Hernandez-Diaz S, Werler MM, Walker AM, et al: Neural tube defects in concluded that no consistent negative association existed between relation to use of folic acid antagonists during pregnancy. Am J Epidemiol prenatal cocaine exposure and postnatal physical growth, develop- 153:961, 2001. mental test scores, receptive language, or standardized parent and 25. Barr M: Teratogen update: angiotensin-converting enzyme inhibitors. teacher reports of child behavior. An association between prenatal Teratology 50:399, 1994. 26. Honein MA, Paulozzi LJ, Cragan JD, et al: Evaluation of selected charac- cocaine exposure and decreased emotional expressiveness has been teristics of pregnancy drug registries. Teratology 60:356, 1999. suggested.163 27. Wyszynski DF, Nambisan M, Surve T, et al: Antiepileptic Drug Pregnancy Registry: Increased rate of major malformations in offspring exposed to valproate during pregnancy. Neurology 64:961, 2005. References 28. Jones KL, Lacro RV, Johnson KA, et al: Pattern of malformations in the 1. Moore KL, Persaud TVN: The Developing Human: Clinically Oriented children of women treated with carbamazepine during pregnancy. N Engl Embryology, 7th ed. Philadelphia: Saunders, 2002. J Med 320:1661, 1989.
- 11. CHAPTER 20 Teratogenesis and Environmental Exposure 357 29. Glaxo Smith Kline: Paroxetine Studies: EPIP083. Available at http://ctr. 57. Ornoy A, Cohen E: Outcome of children born to epileptic mothers treated gsk.co.uk/summary/paroxetine/studylist.asp (accessed January 14, 2008). with carbamazepine during pregnancy. Arch Dis Child 75:517, 1996. 30. Pastuszak AL, Schuler L, Speck-Martins CE, et al: Use of misoprostol 58. Nulman I, Scolnik D, Chitayat D, et al: Findings in children exposed in during pregnancy and Mobius’ syndrome in infants. N Engl J Med utero to phenytoin and carbamazepine monotherapy: Independent effects 339:1553, 1998. of epilepsy and medications. Am J Med Genet 68:18-24, 1997. 31. Mitchell AA: Systematic identification of drugs that cause birth defects: A 59. Wide K, Henning E, Tomson T, Winbladh B: Psychomotor development new opportunity. N Engl J Med 349:2556, 2003. in preschool children exposed to antiepileptic drugs in utero. Acta Paediatr 32. Polifka J, Friedman JM: Developmental toxicity of Ribavirin/IFalpha com- 91:409, 2002. bination therapy: Is the label more dangerous than the drugs? Birth 60. Vaux KK, Kahole NCO, Jones KL: Cyclophosphamide, methotrexate and Defects Res A Clin Molec Teratol 67:8, 2003. cytarabine embryopathy: Is apoptosis the common pathway? Birth Defects 33. Scialli A, Buelke-Sam JL, Chambers CD, et al: Communicating risk during Res A Clin Mol Teratol 67:403, 2003. pregnancy: A workshop on the use of data from animal developmental 61. Milunsky A, Graef JW, Gaynor MF Jr: Methotrexate-induced congenital toxicity studies in pregnancy labels for drugs. Birth Defects Res A Clin malformations. J Pediatr 72:790, 1968. Molec Teratol 70:7, 2004. 62. Del Campo M, Kosaki K, Bennett FC, et al: Developmental delay in fetal 34. Weiner CP, Buhimschi C: Drugs for Pregnant and Lactating Women, 2nd aminopterin/methotrexate syndrome. Teratology 60:10, 1999. ed. New York: Churchill Livingstone, 2007. 63. Feldkamp M, Carey JC: Clinical teratology counseling and consultation 35. Schaeffer C, Peters PWJ, Miller RK (eds): Drugs During Pregnancy and case report: Low dose methotrexate exposure in the early weeks of preg- Lactation: Treatment Options and Risk Assessment. New York: Academic nancy. Teratology 47:553, 1993. Press, 2007. 64. Lewden B, Vial T, Elefant E, et al: Low dose methotrexate in the first tri- 36. Holzgreve W, Carey JC, Hall BD: Warfarin-induced fetal abnormalities. mester of pregnancy: Results of a French collaborative study. J Rheumatol Lancet 2:914, 1976. 31:2360, 2004. 37. Hall JG, Pauli RM, Wilson KM: Maternal and fetal sequelae of anticoagu- 65. Rodriguez-Pinilla E, Martinez-Frias ML: Corticosteroids during preg- lation during pregnancy. Am J Med 68:122, 1980. nancy and oral clefts: A case-control study. Teratology 58:2, 1988. 38. van Driel D, Wesseling J, Sauer PJ, et al: Teratogen update: Fetal effects 66. Czeizel AE, Rockenbauer M: Population-based case-controls study of tera- after in utero exposure to coumarins overview of cases, follow-up findings, togenic potential of corticosteroids.Teratology 56:335, 1997. and pathogenesis. Teratology 66:127, 2002. 67. Carmichael SL, Shaw GM: Maternal corticosteroid use and risk of selected 39. Cotrufo M, DeFeo M, DeSanto LS, et al: Risk of warfarin during congenital anomalies. Am J Med Genet 86:242, 1999. pregnancy with mechanical valve prostheses. Obstet Gynecol 99:35, 68. Pradat P, Robert-Gnasia E, Di Tanna GL, et al: First trimester exposure to 2002. corticosteroids and oral clefts. Birth Defects Res A Clin Mol Teratol 67:968, 40. van Driel D, Wesseling J, Sauer PJ, et al: In utero exposure to coumarins 2003. and cognition at 8-14 years. Pediatrics 107:123, 2001. 69. Reinisch JM, Simon NG, Karow WG, et al: Prenatal exposure to predni- 41. Gilmore J, Pennell PB, Stern BJ: Medication use during pregnancy for sone in humans and animals retards intrauterine growth. Science 202:436, neurologic conditions. Neurol Clin 16:189, 1998. 1978. 42. Canger R, Battino D, Canevini MP, et al: Malformations in offspring of 70. Rayburn WF. Glucocorticord therapy for rheumatic diseases: Maternal, women with epilepsy: A prospective study. Epilepsia 40:1231, 1999. fetal, and breast-feeding considerations. Am J Reprod Immunol 28:138, 43. Holmes LB, Harvey EA, Coull BA, et al: The teratogenicity of anticonvul- 1992. sant drugs. N Engl J Med 344:1132, 2001. 71. Alwan S, Polifka JE, Friedman JM: Angiotensin II receptor antagonists 44. Yerby MS: Epilepsy and pregnancy: New issues for an old disorder. Neurol treatment during pregnancy. Birth Defects Res A Clin Mol Teratol 73:123, Clin 11:777, 1993. 2005. 45. Kaneko S, Otani K, Fukushima Y, et al: Teratogenicity of antiepileptic 72. Cooper WO, Hernandez-Diaz S, Arbogast PG et al: Angiotensin convert- drugs: An analysis of possible risk factors. Epilepsia 29:459, 1988. ing enzyme inhibitors and the risk of major congenital malformations. N 46. Koch S, Losche G, Jager-Roman E, et al: Major and minor birth malforma- Engl J Med 354:2443, 2006. tions and antiepileptic drugs. Neurology 42:83, 1992. 73. Weinstein MR, Goldfield M: Cardiovascular malformations with lithium 47. Hanson JW, Smith DW: The fetal hydantoin syndrome. J Pediatr 87:285, use during pregnancy. Am J Psychiatry 132:529-531, 1975. 1975. 74. Jacobson SJ, Jones K, Johnson K, et al: Prospective multicentre study of 48. Hanson JW, Myrianthopoulos NC, Harvey MA, et al: Risks to offspring of pregnancy outcome after lithium exposure during first trimester. Lancet women treated with hydantoin anticonvulsants with emphasis on the fetal 339:869, 1992. hydantoin syndrome. J Pediatr 89:662, 1976. 75. Zalzstein E, Koren G, Einarson T, Freedom RM: A case-control study on 49. Kelly TE, Rein M, Edwards P: Teratogenicity of anticonvulsant drugs I: the association between first trimester exposure to lithium and Ebstein’s Review of the literature. Am J Med Genet 19:413, 1984. anomaly. Am J Cardiol 65:817-818, 1990. 50. Hanson JW: Teratogen update: Fetal hydantoin effects. Teratology 33:349, 76. Kallen BAJ, Olausson PO: Maternal use of selective serotonin re-uptake 1986. inhibitors in early pregnancy and infant congenital malformations. Birth 51. Adams J, Voorhees CV, Middaugh LD: Developmental neurotoxicity of Defects Res A Clin Mol Teratol 79:301, 2007. anticonvulsants: Human and animal evidence on phenytoin. Neurotoxicol 77. Berard A, Ramos E, Rey E, et al: First trimester exposure to paroxetine and Teratol 12:203, 1990. risk of cardiac malformations in infants: The importance of dosage. Birth 52. Scolnik D, Nulman I, Rovet J, et al: Neurodevelopment of children exposed Defects Res B Reprod Toxicol 80:18, 2007. in utero to phenytoin and carbamazepine monotherapy. JAMA 271:767, 78. Alwan S, Reefhuis J, Rasmussen SA, et al: Use of selective serotonin- 1994. reuptake inhibitors in pregnancy and the risk of birth defects. N Engl 53. Robert E, Guibaud P: Maternal valproic acid and congenital neural tube J Med 354:2684, 2007. defects. Lancet 2:937, 1982. 79. Louik C, Lin AE, Werler MM, et al: First-trimester use of selective sero- 54. DiLiberti JH, Farndon PA, Dennis NR, et al: The fetal valproate syndrome. tonin-reuptake inhibitors and the risk of birth defects. N Engl J Med Am J Med Genet 19:473, 1984. 356:2675, 2007. 55. Adab N, Jacoby A, Smith D, et al: Additional educational needs in children 80. Chambers CD, Hernandez-Diaz S, Van Marter LJ, et al: Selective sero- born to mother with epilepsy. J Neurol Neurosurg Psychiatry 70:15, tonin-reuptake inhibitors and risk fo persistent pulmonary hypertension 2001. of the newborn. N Engl J Med 354:579, 2006. 56. Adab N, Kini V, Vinten J, et al: The longer-term outcome of children born 81. Moses-Kolko EL, Bogen D, Perel J, et al: Neonatal signs after late in utero to mothers with epilepsy. J Neurol Neurosurg Psychiatry 75:1575, 2004. exposure to serotonin reuptake inhibitors JAMA 293:2372, 2005.
- 12. 358 CHAPTER 20 Teratogenesis and Environmental Exposure 82. Geelen JA, Langman J, Lowdon JD: The influence of excess vitamin A on 110. Hertz-Picciotto I, Schramm M, Watt-Morse M, et al: Patterns and neural tube closure in the mouse embryo. Anat Embryol (Berl) 159:223, determinants of blood lead during pregnancy. Am J Epidemiol 152:829, 1980. 2000. 83. Rosa FW, Wilk AL, Kelsey FP: Teratogen update: Vitamin A congeners. 111. Jones KL, Smith DW, Ulleland CN, et al: Pattern of malformation in off- Teratology 33:355, 1986. spring of chronic alcoholic mothers. Lancet 1:1267, 1973. 84. Rothman KJ, Moore LL, Singer MR, et al: Teratogenicity of high vitamin 112. Streissguth AP, Aase JM, Clarren SK, et al: Fetal alcohol syndrome in ado- A intake. N Engl J Med 333:1369, 1995. lescents and adults. JAMA 265:1961, 1991. 85. Botto LD, Loffredo C, Scanlon KS, et al: Vitamin A and cardiac outflow 113. Hoyme HE, May PA, Kalberg WO, et al: A practical clinical approach to tract defects. Epidemiology 12:491, 2000. diagnosis of fetal alcohol spectrum disorders: Clarification of the 1996 86. Werler MM, Lammer EJ, Rosenberg L, et al: Maternal vitamin A supple- institute of medicine criteria. Pediatrics 115:39, 2005. mentation in relation to selected birth defects. Teratology 42:497, 1990. 114. Sampson PD, Streissguth AP, Bookstein FL, et al: Incidence of fetal alcohol 87. Mills JL, Simpson JL, Cunningham GC, et al: Vitamin A and birth defects. syndrome and prevalence of alcohol-related neurodevelopmental disor- Am J Obstet Gynecol 177:31, 1997. der. Teratology 56:317, 1997. 88. Martinez-Frias ML, Salvador J: Epidemiological aspects of prenatal 115. Moore CA, Khoury MJ, Liu Y: Does light-to-moderate alcohol consump- exposure to high doses of vitamin A in Spain. Eur J Epidemiol 6:118, tion during pregnancy increase the risk for renal anomalies among off- 1990. spring? Pediatrics 99:E11, 1997. 89. Rizzo R, Lammer EJ, Parano E, et al: Limb reduction defects in humans 116. Shaw GM, Lammer EJ: Maternal periconceptional alcohol consumption associated with prenatal isotretinoin exposure. Teratology 44:599, 1991. and risk for orofacial clefts. J Pediatr 134:298, 1999. 90. Dai WS, LaBraico JM, Stern RS: Epidemiology of isotretinoin exposure 117. Williams LJ, Correa A, Rasmussen S: Maternal lifestyle factors and risk for during pregnancy. J Am Acad Dermatol 26:599, 1992. ventricular septal defects. Birth Defects Res A Clin Mol Teratol 70:59, 91. Adams J, Lammer EJ: Neurobehavioral teratology of isotretinoin. Reprod 2004. Toxicol 7:175, 1993. 118. Martínez-Frías ML, Bermejo E, Rodríguez-Pinilla E, et al: Risk for con- 92. Dai WS, Hsu M-A, Itri LM: Safety of pregnancy after discontinuation of genital anomalies associated with different sporadic and daily doses of isotretinoin. Arch Dermatol 125:362, 1989. alcohol consumption during pregnancy: A case-control study. Birth 93. Kallen B: Restriction of the use of drugs with teratogenic properties: Defects Res A Clin Mol Teratol 70:194, 2004. Swedish experiences with isotretinoin. Teratology 60:53, 1999. 119. Kesmodel U, Wisborg K, Olsen SF, et al: Moderate alcohol intake in preg- 94. Geiger J-M, Baudin M, Saurat J-H: Teratogenic risk with etretinate and nancy and the risk of spontaneous abortion. Alcohol Alcohol 37:87, acitretin treatment. Dermatology 189:109, 1994. 2002. 95. Maradit H, Geiger J-M: Potential risk of birth defects after acitretin dis- 120. Kesmodel U, Wisborg K, Olsen SF, et al: Moderate alcohol intake during continuation. Dermatology 198:3, 1999. pregnancy and the risk of stillbirth and death in the first year of life. Am 96. Grønhøj Larsen F, Steinkjer B, Jakobsen P, et al: Acitretin is converted to J Epidemiol 155:305, 2002. etretinate only during concomitant alcohol intake. Br J Dermatol 143:116, 121. Iyasu S, Randall LL, Welty TK, et al: Risk factors for sudden infant death 2000. syndrome among northern plains Indians. JAMA 288:2717, 2002. 97. Otake M, Schull WJ: In utero exposure to A-bomb radiation and mental 122. Carpenter RG, Irgens LM, Blair PS, et al: Sudden unexplained infant retardation: A reassessment. Br J Radiol 57:409, 1984. death in 20 regions in Europe: Case control study. Lancet 363:185, 98. Yamazaki JN, Schull WJ: Perinatal loss and neurological abnormalities 2004. among children of the atomic bomb: Nagasaki and Hiroshima revisited, 123. Abel EL: An update on the incidence of FAS: FAS is not an equal oppor- 1949 to 1989. JAMA 265:605-609, 1990. tunity birth defect. Neurotoxicol Teratol 17:437, 1995. 99. Brent RJ: The effect of embryonic and fetal exposure to x-ray, microwaves, 124. Jones KL, Smith DW: The fetal alcohol syndrome. Teratology 12:1, and ultrasound: Counseling the pregnant and nonpregnant patient about 1975. these risks. Semin Oncol 16:347, 1989. 125. Streissguth AP, Barr HM, Sampson PD: Moderate prenatal alcohol expo- 100. Matsumoto H, Koya G, Takeuchi T: Fetal Minimata disease: A neuro- sure: Effects on child IQ and learning problems at age 7 1/2 years. Alcohol pathological study of two cases of intrauterine intoxication by a methyl- Clin Exp Res 14:662, 1990. mercury compound. J Neuropath Exp Neurol 24:563, 1965. 126. Day NL, Leech SL, Richardson GA, et al: Prenatal alcohol exposure pre- 101. Bakir F, Damluji SF, Amin-Zaki L, et al: Methylmercury poisoning in Iraq: dicts continued deficits in offspring size at 14 years of age. Alcohol Clin An interuniversity report. Science 181:230, 1973. Exp Res 26:1584, 2002. 102. Kondo K: Congenital Minamata disease: Warnings from Japan’s experi- 127. Jacobson SW: Specificity of neurobehavioral outcomes associated with ence. J Child Neurol 15:458, 2000. prenatal alcohol exposure. Alcohol Clin Exp Res 22:313-320, 1998. 103. Mahaffey KR: Recent advances in recognition of low-level methylmercury 128. Jacobson SW, Jacobson JL, Sokol RJ, et al: Maternal age, alcohol abuse poisoning. Curr Opin Neurol 13:699, 2000. history, and quality of parenting as moderators of the effects of prenatal 104. U.S. Environmental Protection Agency and U.S. Food and Drug Admin- alcohol exposure on 7.5-year intellectual function. Alcohol Clin Exp Res istration: What You Need to Know about Mercury in Fish and Shellfish. 28:1732, 2004. Available at http://www.epa.gov/waterscience/fishadvice/advice.html 129. Khaole NC, Ramchandani VA, Viljoen DL, et al: A pilot study of alcohol (accessed January 14, 2008). exposure and pharmacokinetics in women with or without children with 105. Rom WN: Effects of lead on the female and reproduction: A review. Mt fetal alcohol syndrome. Alcohol Alcohol 39:503, 2004. Sinai J Med 43:542-53, 1976. 130. Warren KR, Li T-K: Genetic polymorphisms: Impact on the risk of fetal 106. Hertz-Picciotto I: The evidence that lead increases the risk for spontane- alcohol spectrum disorders. Birth Defects Res A Clin Mol Teratol 73:195, ous abortion. Am J Ind Med 38:300, 2000. 2005. 107. Bellinger D, Leviton A, Waternaux C, et al: Longitudinal analyses of pre- 131. Goodlett CR, West JR: Fetal alcohol effects: Rat model of alcohol exposure natal and postnatal lead exposure and early cognitive development. N Engl during the brain growth spurt. In Zagon IS, Slotkin TA (eds). Maternal J Med 316:1037, 1987. Substance Abuse and the Developing Nervous System. San Diego, Aca- 108. Dietrich KN, Krafft KM, Bornschein RL, et al: Low-level fetal lead expo- demic Press, 1992, pp 45-75. sure effect on neurobehavioral development in early infancy. Pediatrics 132. U.S. Department of Health and Human Services, Office of the Surgeon 80:721, 1987. General: News Release: U.S. Surgeon General Releases Advisory on 109. Tong SL, Baghurst P, McMichael A, et al: Lifetime exposure to environ- Alcohol Use in Pregnancy, February 21, 2005. Available at http://www. mental lead and children’s intelligence at 11-13 years: The Port Pirie surgeongeneral.gov/pressreleases/sg02222005.html (accessed January 14, cohort study. BMJ 312:1569, 1996. 2008).