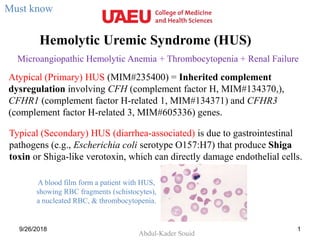
![Typical (Secondary) HUS (diarrhea-associated) is due to gastrointestinal pathogens
(e.g., Escherichia coli serotype O157:H7) that produce Shiga toxin or Shiga-like
verotoxin, which can directly damage endothelial cells.
9/26/2018 2
[Moake JL. Thrombotic
microangiopathies. N Engl J Med.
2002;347:589-600. PMID: 12192020]](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a HUS.ppt
Semelhante a HUS.ppt (20)
Mais de AbdulKaderSouid
Mais de AbdulKaderSouid (14)
Último
Último (20)
HUS.ppt
- 1. Hemolytic Uremic Syndrome (HUS) Abdul-Kader Souid 9/26/2018 1 Microangiopathic Hemolytic Anemia + Thrombocytopenia + Renal Failure Atypical (Primary) HUS (MIM#235400) = Inherited complement dysregulation involving CFH (complement factor H, MIM#134370,), CFHR1 (complement factor H-related 1, MIM#134371) and CFHR3 (complement factor H-related 3, MIM#605336) genes. Typical (Secondary) HUS (diarrhea-associated) is due to gastrointestinal pathogens (e.g., Escherichia coli serotype O157:H7) that produce Shiga toxin or Shiga-like verotoxin, which can directly damage endothelial cells. Must know A blood film form a patient with HUS, showing RBC fragments (schistocytes), a nucleated RBC, & thrombocytopenia.
- 2. Typical (Secondary) HUS (diarrhea-associated) is due to gastrointestinal pathogens (e.g., Escherichia coli serotype O157:H7) that produce Shiga toxin or Shiga-like verotoxin, which can directly damage endothelial cells. 9/26/2018 2 [Moake JL. Thrombotic microangiopathies. N Engl J Med. 2002;347:589-600. PMID: 12192020]
- 3. 9/26/2018 3 A 22-Month-old Toddler Presents with Diarrhea, Pallor and Bruises ↓Platelets + Anemia + ↑RBC Fragments → Intravascular (Microangiopathic) Hemolysis Laboratory monitoring: CBC Reticulocyte count Blood film Urinalysis Serum creatinine Serum electrolytes Biomarkers of hemolysis Total bilirubin LDH (lactate dehydrogenase) Haptoglobin 75 80 85 90 95 100 105 110 115 0 100 200 300 400 500 2 4 6 8 10 12 14 Hemoglobin Platelets Hemoglobin(g/L) Plateletcount(x10 9 /L) Days Schistocytes Must know
- 4. 9/26/2018 4 Biochemical Studies ↑Creatinine = Renal Failure ↑LDH + ↓Haptoglobin = Hemolysis 75 80 85 90 95 100 105 110 115 30 40 50 60 70 80 2 4 6 8 10 12 14 Hemoglobin Serum creatinine Hemoglobin(g/L) Serumcreatinine(mol/L) Days Normal creatinine concentration Eculizumab
- 6. 9/26/2018 6 Patient’s Further Investigations ↓Platelets + ↑ Intravascular Hemolysis + ↑Renal Failure = Hemolytic Uremic Syndrome (HUS) Weekly eculizumab (terminal complement inhibitor) was started. • Stool culture → Salmonella • Total complement (CH50) is <10 kUmL (normal, 32-58). • Serum levels of C3 and C4 are normal.
- 7. Salmonella Enteritidis & HUS • Giménez L, et al. Hemolytic-uremic syndrome. A review of 58 cases. An Pediatr (Barc) 2008;69:297-303. – 58 patients were included, mean age ~3 yr, most in the summer. 48 patients presented with typical HUS (with diarrhea). Salmonella enteritidis and Escherichia coli O157:H7 were isolated from those patients. Seven cases presented with atypical HUS (without diarrhea), most of them had a respiratory infection due to Streptococcus. 9/26/2018 7 Reading only
- 8. Eculizumab Case reports have demonstrated eculizumab is effective in complement-mediated HUS (genetic defects or autoantibodies to complement proteins). 9/26/2018 8 Eculizumab Product Label Must know
- 9. Hemolytic Uremic Syndrome • Primary HUS = Complement dysregulation (10% of cases) – E.g., mutations in Complement factors H (MIM#134370, AD/AR) and I (MIM#217030, AD) genes. – Diagnosis requires complement genotyping. • Secondary HUS – Shiga toxin-producing Escherichia coli (STEC) – Pneumococcal infection 9 Must know • Treatment Eculizumab: Blocks cleavage of C5, thereby preventing production of the membrane attack complex C5b-9 (similar to PNH). Plasma exchange or plasma infusion for secondary HUS with normal complement. AD, autosomal dominant; AR, autosomal recessive
- 10. 10 A 5-year-old boy presents with sudden onset of fatigue, pallor, and bruising. His examination reveals normal lymph nodes, liver, and spleen. His WBC count is 7 x109/L (normal, 5 to 10), hemoglobin 63 g/L (normal, 110 to 130), reticulocytes 332 x109/L (normal, 35 to 100 x109/L), and platelet count 35 x109/L (normal, 150 to 400). Blood smear shows schistocytes and markedly reduced number of platelets. PT/INR, aPTT, TT, fibrinogen, and D-Dimer level are normal. His urinalysis shows 2 RBC per high power field (normal, <5) and 3+ hemoglobin. His serum creatinine is 89 mmol/L (normal for age, 27 to 62 mmol/L). Total complement (CH50) is <10 kUmL (normal, 32-58). Which one of the following diagnoses is correct? A. Macrophage activation syndrome (MAS) B. Hemolytic uremic syndrome (HUS) C. Thrombotic thrombocytopenic purpura (TTP) D. Autoimmune hemolytic anemia (AHA) E. Disseminated intravascular coagulopathy (DIC)
- 11. Which one of the following laboratory investigations is most likely to confirm the diagnosis? A. Mutation in complement regulation gene (for HUS) B. Mutation in ADAMTS13 gene (for TTP) C. Mutation in perforin gene (for HLH) D. Positive direct antiglobulin test for IgG (for autoimmune hemolytic anemia, AHA) E. Missing CD59 on the surface of blood cells (for PNH) 11 A 5-year-old boy presents with sudden onset of fatigue, pallor, and bruising. His examination reveals normal lymph nodes, liver, and spleen. His WBC count is 7 x109/L (normal, 5 to 10), hemoglobin 63 g/L (normal, 110 to 130), reticulocytes 332 x109/L (normal, 35 to 100 x109/L), and platelet count 35 x109/L (normal, 150 to 400). Blood smear shows schistocytes and markedly reduced number of platelets. PT/INR, aPTT, TT, fibrinogen, and D-Dimer level are normal. His urinalysis shows 2 RBC per high power field (normal, <5) and 3+ hemoglobin. His serum creatinine is 89 mmol/L (normal for age, 27 to 62 mmol/L). Total complement (CH50) is <10 kUmL (normal, 32-58).
- 12. 12 A 5-year-old boy presents with sudden onset of fatigue, pallor, and bruising. His examination reveals normal lymph nodes, liver, and spleen. His WBC count is 7 x109/L (normal, 5 to 10), hemoglobin 63 g/L (normal, 110 to 130), reticulocytes 332 x109/L (normal, 35 to 100 x109/L), and platelet count 35 x109/L (normal, 150 to 400). Blood smear shows schistocytes and markedly reduced number of platelets. PT/INR, aPTT, TT, fibrinogen, and D-Dimer level are normal. His urinalysis shows 2 RBC per high power field (normal, <5) and 3+ hemoglobin. His serum creatinine is 89 mmol/L (normal for age, 27 to 62 mmol/L). Total complement (CH50) is <10 kUmL (normal, 32-58). Which one of the following treatments is correct? A. Corticosteroids (for ITP) B. Packed red cell transfusion (for AHA) C. Platelet transfusion D. Eculizumab (for HUS or PNH) E. Immunoglobulin transfusion (for ITP)
- 13. Required Reading • Geerdink LM, Westra D, van Wijk JA, et al. Atypical hemolytic uremic syndrome in children: complement mutations and clinical characteristics. Pediatr Nephrol 2012;27:1283. • Veesenmeyer AF, Edmonson MB. Trends in US hospital stays for Streptococcus pneumoniae-associated hemolytic uremic syndrome. Pediatr Infect Dis J 2013;32:731. • Al-Akash SI, Almond PS, Savell VH Jr, et al. Eculizumab induces long-term remission in recurrent post-transplant HUS associated with C3 gene mutation. Pediatr Nephrol 2011; 26:613. • Guigonis V, Frémeaux-Bacchi V, Giraudier S, et al. Late-onset thrombocytic microangiopathy caused by cblC disease: association with a factor H mutation. Am J Kidney Dis 2005;45:588. 9/26/2018 13