13 lymphoid organs dr kirti 21 dec (2)
•Transferir como PPT, PDF•
6 gostaram•6,581 visualizações


Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a 13 lymphoid organs dr kirti 21 dec (2)
Semelhante a 13 lymphoid organs dr kirti 21 dec (2) (20)
Mais de Nepalese army institute of health sciences
Mais de Nepalese army institute of health sciences (20)
13 lymphoid organs dr kirti 21 dec (2)
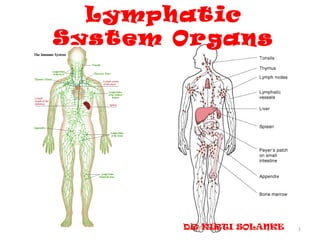
- 1. Lymphatic System Organs DR KIRTI SOLANKE 1
- 2. INTRODUCTION • Not a primary tissue type but a variety of connective tissue. • Components-1.lymphatic vessels 2.lymphatic organs 3.cells 4.lymph 2
- 3. Primary Lymphatic Organs and Tissues • The primary (central) lymphatic organs and tissues include the thymus, bone marrow and gut associated lymphatic tissue (GALT). • They are sites of – antigen-independent proliferation, and – differentiation into cells pre-programmed to recognise specific antigens. • These immunocompetent cells then enter the blood and lymph: – get dispersed in the connective tissue and – penetrate into epithelia that line mucosal surfaces. 3
- 4. Secondary Lymphatic Organs and Tissues • These are the effector lymphatic tissues. • They include the lymphatic nodules, lymph nodes, tonsils and the spleen. • Here lymphocytes undergo antigen- dependent proliferation and differentiation into effector lymphocytes and memory cells. 4
- 5. 5
- 6. Lymphatic capillaries are not ubiquitous-absent in cornea, cartilage, thymus, central and peripheral nervous sys & bone marrow. Lymphatic circulation Vascular circulation • Deep • Superficial • Valves closely placed • Less closely placed • Blind ends • Both ends open • No pericytes • Pericyte • Irregular shape in cut sec. • Cylindrical form • Basal lamina incomplete • Continuous • Greater caliber • Less caliber 6
- 7. LYMPH • Lighter specific gravity than blood • Contains no RBCs,platelets,fibrinogen but it contains numerous Lymphocytes. • Lymphocytes are added when it passes through LN. • Coagulate at much slower rate than blood • Does not carry O2 but may contain CO2. • Chyle-fat globules, lacteal 7
- 8. 8
- 9. • Lymph vessels of- thyroid gland -oesophagus -coronary and triangular ligaments of liver may drain directly into thoracic duct. 9
- 10. Functions of lymphoid system 1) To maintain – pressure & -volume of extracellular fluid by returning excess water to the circulation. 2) The site of clonal production of immunocompetent lymphocytes and macrophages in the specific immune response. 10
- 11. CELLS OF LYMPHATIC SYSTEM Chief cells are lymphocytes-type of WBC’S. • B lymphocytes • T lymphocytes • Natural killer cells • epithelioreticular cells - MESENCHYMAL • Supporting cells- – interact with lymphocyte – Present antigens to Lymphocytes • OTHER TYPE OF WBC’S -monocyte -macrophages -neutruphils -eosinophils -basophils 11
- 12. • ANTIGEN PRESENTING CELLS – dendriti cells-Bone marrow derived – follicular cells – langerhan’s cells 12
- 13. Derivation and Distribution of Lymphocytes 13
- 14. T Lymphocytes • These evolve in the thymus • part of the cell-mediated or thymus- dependent response to antigens. • Upon interaction with an antigen, they will differentiate and proliferate into - 3 types of effector T lymphocytes: 14
- 15. 1.Cytotoxic lymphocytes (killer T cells) (primary effector cells in cell-mediated immunity.) scan the surface of other cells for signs of viral infection or abnormality, killing them if necessary by causing them to lyse. 2.Helper T lymphocytes, recognise foreign antigens presented by macrophages. release interleukin hormones to stimulate ‘processed’ B cells to produce antibodies. 3.Suppresser T lymphocytes, suppress the activity of B cells. 15
- 16. HELPER T CELL SUBTYPES(CYTOKINES) • Th1 cell • Th2 cells • interact with cytotoxic • interact with B CD8,NK ,macrophages. lymphocyte • CMI • HIR • For controling • Exracellular pathogens intracellular pathogens • Viruses & microorganisms. • IL 2,Interferon gamma • IL4, 5 ,10,13. 16
- 17. B Lymphocytes • These evolve in bone marrow and GALT, and are part of the humoral response. • They will only react with the antigen they have been genetically programmed for. • Once activated by this antigen, they may differentiate and proliferate into either: • Plasma cells, that produce antibodies. 17
- 18. • The antibody binds, forming an antibody-antigen complex, that may be phagocytosed by macrophages. • Memory cells, which, after exposure to the specific antigen, will be able to participate in a rapid, secondary response with the same antigen. • They do not participate in an initial or primary response. 18
- 19. 19
- 20. B – Lymphocytes T-Lymphocyte – Prog In Thymus – Prog In B M – Long life span – Variable lifespan – For CMI – For H.I. – Graft Rejection – Plasma Cells – Ab – 60% to 8o% – 20 to 30% – CD 2,CD3,CD7 – CD9,CD19,CD20 & CD24 – T cell receptors(TCRs) – Bcell receptors – CD4,CD8 – MHC II 20
- 21. NK LYMPHOCYTE/NULL CELLS • Neither T nor B cells • Specialised to kill certain types of target cells • 5 to 10% • Do not mature in thymus • Kill in the same way as that of CTLS • After recognition of tranformed cell,secrete perforins & fragmentins • CD 56, CD94. 21
- 22. Macrophages • These are involved in both types of immune response. • They can process and present the antigen to the B cells or helper T cells. • Or they can destroy the antigen by digestion after it has been processed by other cells of the immune system. 22
- 23. CLASSIFICATION I. FUNCTIONAL LYMPHOID ORGANS CENTRAL PERIPHERAL THYMUS LYMPH NODE BONE MARROW SPLEEN MALT, GALT 23
- 24. II. MORPHOLOGICAL LYMPHOID ORGANS DISCRETE DIFFUSE LN, SPLEEN BM, PEYER’S PATCHES THYMUS, TONSIL 24
- 25. LYMPH NODE • Oval/Kidney Shape, 0.1 – 0.5cm Long • Normal young body contains up to 450,of which 60 to 70 in head and neck,100 in thorax,250 in abd& pelvis • Greatest no. lie close to the viscera mainly mesenteries. 25
- 26. Lymph Node: Gross Appearance 26
- 27. 27
- 28. 28
- 29. 29
- 30. 30
- 31. • Capsule – Trabeculae, hilus- collagenous framework • Lymph flow – Retculin Meshwork-sinuses – Subcapsular Sinus – Cortical Sinuses – Medullary Sinuses – Eff Lymph Ch • Cortex medulla-diff in arrangement 31
- 32. 3 2 1 32
- 33. • Role of germinal centre-affinity maturation • Two zones in GC-dark zone-centroblast- undergoing rapid proliferation- hypermaturation of their antibody mol. • light zone-centrocytes- ineract with the FDC- carrying unprocessed antigen on their surface. 33
- 34. Lymph Node 34
- 35. 35
- 36. Lymph Node A - Afferent lymphatic channels B - Subcapsular sinus C - Follicle D - Sinuses E - Paracortical region F - Medullary cords G - Efferent lymphatic channel 36
- 37. Variations in nodes • In large nodes –trabeculae are prominent • In small nodes-thin and frequently interrupted • Hemal nodes • lymphadenitis 37
- 38. • Diffusely distributed lymphatic nodules represent local immune response to antigen that are present in tissue fluid. • LN-lymph. • Spleen-circulating blood-mainly HIR. 38
- 39. The Spleen • The spleen is the largest lymphatic organ, located in the upper left quadrant of the abdominal cavity. • The spleen functions to filter the blood, and react immunologically to blood-borne antigens mainly HIR,to dispose of defective blood cells,store blood cells &platelets,hematopoiesis 39
- 40. Structure of the Spleen • There is an external capsule of dense connective tissue. • trabeculae extend into the substance of the organ. • myofibroblasts, and is thus contractile. • medial surface of the spleen, the hilum allows passage of the splenic vessels, nerves and lymphatic vessels. • The substance of the spleen is known as the splenic pulp. • white pulp areas, • surrounded by red pulp. 40
- 41. Spleen 41
- 42. The White Pulp • This mainly consists of lymphocytes. • Branches of the splenic artery course through the trabeculae and then enter the white pulp, known as the central artery • The lymphocytes aggregated around the central artery in a cylindrical fashion -periarterial lymphatic sheath (PALS) of the artery. • Lymph nodules in the PALS may displace the central artery from its central position in the white pulp. 42
- 43. The Red Pulp • This has large numbers of red blood cells (RBCs). • It consists of splenic sinuses, separated by splenic cords (of Billroth). 43
- 44. 44
- 45. 45
- 46. 46
- 47. 47
- 48. 48
- 49. 49
- 50. 50
- 51. Spleen 51
- 52. SPLENIC A SEGMENTAL A TRABECULAR A CENTRAL A FOLLICULAR A PENICILLAR A ELLIPSOIDS PRE CAPILLARY A SINUSOIDS TRABECULAR VEINS SPLENIC VEIN
- 53. 53
- 54. Splenic Circulation • The splenic artery branches into the trabecular, the central arteries. • The central arteries of the white pulp then branch into penicillar arterioles in the red pulp. • These are actually capillaries, and may be sheathed by aggregations of macrophages. • Blood from these penicilli leaves the vascular system to populate the splenic pulp, before re-entering the red pulp. 54
- 55. Two theories • Closed Circulation Model • In this model, the splenic arterioles are a "continuous vascular channel". • They only empty into the splenic sinuses of the red pulp. • The blood then leaves the sinuses before re-entering them. • • Open Circulation Model • In this model, the arterioles empty directly into the splenic cords. • Thus, blood percolates through the reticular meshwork of the pulp. • It then only enters the splenic sinuses from the extravascular side. • This model has more supporting evidence than the former. • FUNCTIONS 55
- 56. THYMUS • Introduction • Gross anatomy • development • Histology -Circulation -Relation with immunology • Functions • Age changes • Recent advances 56
- 57. The Thymus (neuroendocrine organ) • The thymus -4-6 cm long 2.5-5 cm wide 1cm thick,20 gm bi-lobed organ • left lobe higher superior mediastinum, anterior to the heart and great vessels • Thyrothymic ligament • b/d supply-inf thyroid A,Internal thorasic A. • Lymphatics- parasternal,brachiocephalic,trache obronchial 57
- 58. Structural components • Stroma-capsule -trabeculae • Parenchyma –epithelioreticular cells -lymphocytes -macrophages -mast cells 58
- 59. Development • 3rd &4th endodermal pouch-epithelial reticular cells • Local cardiac neural crest mesenchyme control dev of gland. 59
- 60. Development • . 60
- 61. 61
- 62. Histology • Important environment-acquiring immune tolerance • Dev of T lymphocyte-interaction between -thymocyte & -epithelioreticular cells,APC,chemical factors • Capsule-incomplete trabeculae-irregular lobule-0.5-2mm in dia. 62
- 63. Thymus 63
- 64. CIRCULATION • Thymic cortex and medulla functionally independent. lymphoid stem cells from BM outer cortex progeny proliferate & differentiat inner cortex medullary venules at CM junction. 64
- 65. cortex medulla • Dark staining-small L • Paler staining-large L • Less in no • Macropgages,dendritic cells are more • Plasma cells absent • Plasma cells present • b/d supply mainly by • Mainly thymic A,arteriole capillaries 65
- 66. Epithelioreticular cells • Parenchyma: epithelioreticular cells. – are epithelial cells having stellate shape – form cytoplasmic reticulum: a framework for the thymic lymphocytes. – correspond to the other reticular cells in lymphatic tissues, – but no reticular fibres in the thymus. – Feature of both epithelial (intercellular junctions, intermediate filament)and reticular cells(framework) --thymic nurse cells – crosstalk 66
- 67. Epithelioreticular cells • 6 types • Type l-boundary of capsule & cortex • Type ll-within cortex, compartmentalize the cortex • Type lll-between cortex and medulla • Type lV –b/w cortex & medulla,barrier at CM junction • Type V-like type ll in cortex • Type lV – corpuscles, keratohyaline granules, produce lL-4&7. 67
- 68. OTHER CELLS • Myeloid lineage-monocyte • Macrophages-PAS cells • Fibroblast • Myoid cells • Hassall’s corpuscles-distinguishing feature of thymic medulla.30-100μm in dia. IL-4,IL-7;named after Arthur Hill Hassall British physician • Plasma cells are rare in cortex. • adipocytes 68
- 70. 70
- 71. 71
- 72. THYMIC HORMONES • epithelial reticular cells - 1.thymopoietin 2.thymosin alpha Induce expression of T lymphocyte surface markers 72
- 73. THYMIC BARRIER • No afferent lymphatics • Physical barrier-Capillary endothelium -Endothelial basal lamina - pericyte -thin perivascular connective tissue sheath with macrophages - Basal lamina of the epithelioreticular cells - Epithelioreticular cell sheath 73
- 74. 74
- 75. Changes of Thymic Structure with Age (involution) • Largest at birth • fully functional at 20 weeks of foetal life. • progressive involution of adipose tissue. – Accelerated by adrenal corticosteroids and sex hormones • In juveniles: – isolation of cortical compartments, – reduction of cortical and medullary volume, and – appearance of more, larger blood vessels, • until the adult thymus is mainly dominated by fat. 75
- 76. 76
- 77. Thymus 77
- 78. 78
- 79. Applied • Myasthenia gravis • Yellow fever vaccine • DiGeorge syndrome-absent-thymus & parathyroid ,defect in cardiac outflow tract 79
- 80. QUANTIFICATION OF THYMIC FUNCTION • RTE (Recent thymic emigrant)- – newly produced peripheral naive T cells – retain some phenotypic signature of recent thymic maturation – distinguishes them from long lived 80
- 81. 81
- 82. THANK YOU 82
- 83. APPLIED -should ask about a history of thymus disorder or dysfunction, irrespective of age, including myasthenia gravis, thymoma, thymectomy, or DiGeorge syndrome, before administering yellow fever vaccine. (Barwick RS, Marfin AA, Cetron MS. Yellow fever vaccine-associated disease. In: . Washington: ASM Press, 2004: 25-34 vaccine was not one of the live vaccines assessed in the study.) 83
- 84. Involution of the thymus After puberty much of the parenchyma of the thymus, in particular cortical lymphoid tissue, is replaced by adipose tissue. The process, which is called involution, initially proceeds rapidly but slows down in adulthood. Involution is under the control of steroid hormones (both sexual hormones and stress hormones). Although most pronounced in the thymus, involution is a common feature of all lymphoid tissues. Another age-related phenomenon is the increase in size of the thymic (or Hassall's) corpuscles. Thymic corpuscles are rounded eosinophilic structures, which consist of concentrically arranged, flattened cells. Thymic corpuscles are likely to be formed by reticular cells. Similar structures occur also in the tonsils. The size of these structures varies from 20 µm to more than 100 µm in diameter. Thymic corpuscles may calcify, and their core may "dissolve" leading to the formation of a cyst. 84
- 85. DIFFUSE LYMPHATIC ORGANS • Lymphatic nodules-solitary lymphatic nodules -temporary structers -in the lamina propria • Permanent aggregates 85
- 86. PALATINE TONSIL • Shape,location,bed of palatine • Waldeyer’s ring 86
- 87. 87
- 88. LYMPHATIC NODULES/FOLLICLES • In the lamina propria aggregations of small lymphocytes-a form of uncapulated lymphatic tissue • Follicular associated epithelium-covering mucosa-associated L T. • In small & large intestine these specialised cell have characterised short microvilli on their luminal surface called micrifold (M) cells • In palatine tonsils-modified stratified squamous reticulated epithelial cells. 88
- 89. 89
- 90. Gut Associated Lymphoid Tissue • In the lamina propria and submucosal of the gastrointestinal tract from the tongue to the colon are collections of lymphoid tissue. In some areas, the lymphoid tissue is more prominent: – Lingual Tonsil: at the posterior tongue are larger collections of lymphoid tissue. – Pharyngeal Tonsil: these are the structures commonly called "tonsils" and comprise tissues functionally equivalent to lymph nodes. 90
- 91. 91
- 92. 92
- 93. Gut Associated Lymphoid Tissue 93
- 94. 94
Notas do Editor
- FG23_07.JPG Title: Derivation and Distribution of Lymphocytes Notes: Hemocytoblast divisions produce lymphocytic stem cells with two different fates. One group remains in the bone marrow, producing B cells and NK cells. The second group migrates to the thymus, producing T cells. All three types circulate in the bloodstream Keywords: lymphocytes, derivation, distribution, hemocytoblast, lymphoid stem cells, B cells, NK cells, migratory lymphoid stem, thymus, T cells, red bone marrow, peripheral tissue
- Primary l org.
- Middle by CT,capsule attached to fibrous pericardium,ant to aorta inf to lt brachioc v,inf reaches at 4 th costal c sup may extend into neck dev,strap muscles in front-ST,SH,S,F,ITV,3 COSTAL carti,pleura lateraly,phrenic anterolateraly,inf.
- Hollow diverticula from v endo,solid ,grow caudally nc mesenchyme,ventral 2 aortic sac,2meet but do not fuse,ant mediastinum-neck is fully formed& heart has descended,connection with 3 rd pouch soon lost,defective development of cardiac neural crest affect heart& thymic def digeoge s.angiogenic mesenchyme s L stem cells invade by 10 w.by 17 w fully differenciated
- Thymus processed t lym,T cell precursors(thymocyte),immune body’s own comp,to describe histo dev-pharyngeal,mesenchyme,haemo,vascular(angiogenic m)
- Subcapsular cortex,b/d supply
- Innervation -sympathetic chain via cervicothoracic(stellate)ganglion & from vagus, capsule- phrenic & descending cervical n
- Epithelial –framework 4 dev T cells;reticular-correspond 2 RC &their assoc Rfiber in other lymph organ,large EC associated with 50 more thymocyte called nurse.
- Same origine but diff function,morphology.intermediate filament bundles of cytokeratin in cyto.
- KERATANISATION-dev from oropharyngeal epithelium
- Promoted by direct cellular interaction ERC &close proximity 2 stromal macrophages
- After puberty much of the parenchyma of the thymus, in particular cortical lymphoid tissue, is replaced by adipose tissue. The process, which is called involution, initially proceeds rapidly but slows down in adulthood. Involution is under the control of steroid hormones (both sexual hormones and stress hormones). Although most pronounced in the thymus, involution is a common feature of all lymphoid tissues. Another age-related phenomenon is the increase in size of the thymic (or Hassall's) corpuscles. Thymic corpuscles are rounded eosinophilic structures, which consist of concentrically arranged, flattened cells. Thymic corpuscles are likely to be formed by reticular cells. Similar structures occur also in the tonsils. The size of these structures varies from 20 µm to more than 100 µm in diameter. Thymic corpuscles may calcify, and their core may "dissolve" leading to the formation of a cyst.
- provides essential protection to people travelling to or living in areas where yellow fever is endemic or epidemic.