

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a 23204937
Semelhante a 23204937 (20)
Mais de radgirl
Último
Último (20)
23204937
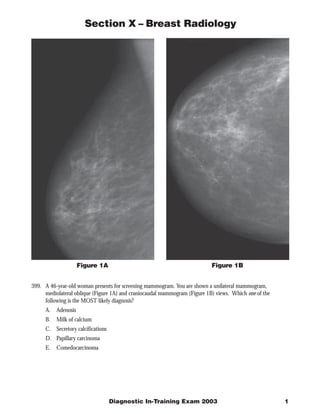
- 1. Section X – Breast Radiology Figure 1B Figure 1A 399. A 46-year-old woman presents for screening mammogram. You are shown a unilateral mammogram, mediolateral oblique (Figure 1A) and craniocaudal mammogram (Figure 1B) views. Which one of the following is the MOST likely diagnosis? A. Adenosis B. Milk of calcium C. Secretory calcifications D. Papillary carcinoma E. Comedocarcinoma Diagnostic In-Training Exam 2003 1
- 2. Section X – Breast Radiology Question #399 Findings: The mammograms show a segmental distribution of pleomorphic calcifications. Rationales: A) Incorrect. Adenosis produces calcifications that amorphous or indistinct, and usually in a clustered of diffuse pattern. B) Incorrect. Milk of calcium produces a teacup configuration in the MLO projection and round shapes with indistinct margins in the CC projection. C) Incorrect. Secretory calcifications are rod and linear in shape. Although they do conform to the duct, as do comedocarcinoma, secretory are thick and do not break up into heterogeneous small particles. D) Incorrect. Papillary carcinoma most commonly produces a mass without calcifications E) Correct. These calcifications are pleomorphic in a ductal distribution. These are classic in appearance for comedocarcinoma Citations: Kopans DB. Breast Imaging 2nd ed. Lippincott-Raven 1998 pp. 315-338 2 American College of Radiology
- 3. Section X – Breast Radiology Figure 2 400. A 51-year-old woman presents with a lump in her left axilla. You are shown a unilateral mammogram, a mediolateral oblique film (Figure 2). Which one of the following is the LEAST likely diagnosis? A. Metastatic breast cancer B. Lymphoma C. Melanoma D. Colon cancer E. Lung cancer Diagnostic In-Training Exam 2003 3
- 4. Section X – Breast Radiology Question #400 Findings: The mammogram shows the development of lymphadenopathy that by the history given is unilateral. The rest of the mammogram shows no abnormal findings. Rationales: A) Incorrect. Metastatic breast cancer can commonly through lymphatics to the axilla. Therefore this is not a least likely choice, and hence incorrect. B) Incorrect Lymphoma, particularly Non-Hodgkin’s lymphoma can present with 30-40% axillary involvement, 13% bilaterally. C) Incorrect. Melanoma and Lung Cancer can both commonly spread hematogenously and lymphatically to lymph nodes. Should be considered in cases in which the mammogram is otherwise normal. D) Correct. Colon carcinoma. The spread of carcinoma from the colon is most commonly hematogenously to the liver. Although metastic colon carcinoma in very advanced stages can spread to the axilla via the lymphatics and thoracic duct, the remaining cancers on the list more commonly spread hematogenously and lymphatically to the axilla than colon carcinoma. E) Incorrect. Melanoma and Lung Cancer can both commonly spread hematogenously and lymphatically to lymph nodes. Should be considered in cases in which the mammogram is otherwise normal. Citations: Cardenosa G. Breast Imaging Companion, 2nd ed. Lippincott Williams and Wilkins, 2001 pp. 342-346 Kopans DB. Breast Imaging 2nd ed. Lippincott-Raven 1998 pp. 607 4 American College of Radiology
- 5. Section X – Breast Radiology Figure 3 401. Regarding the screening mammogram of a 54-year-old woman shown (Figure 3), which one of the following is the MOST likely diagnosis? A. Involuting fibroadenoma B. Ductal carcinoma in situ C. Lobular carcinoma in situ D. Sclerosing adenosis E. Secretory disease Diagnostic In-Training Exam 2003 5
- 6. Section X – Breast Radiology Question #401 Findings: A view from the screening mammogram shows a spiculated mass and numerous associated calcifications that extend beyond the mass toward the nipple. Rationales: A) Incorrect. Fibroadenomas are the most common palpable mass in women younger than 35 years. They can involute after pregnancy or after menopause. Involution involves hyalinization, often leading to calcification. The calcification usually begins as the periphery of the mass and ultimately develops into large “popcorn” calcifications. The fine central calcifications in this case argue against the diagnosis of Involuting fibroadenoma. B) Correct. Ductal carcinoma in situ is a proliferation of cancer cells within the breast ducts, usually the tiny ducts near or within the lobules. It usually presents as a mass with spiculated margins in addition to numerous associated calcifications. The calcifications extend beyond the mass toward the nipple and are usually pleomorphic or fine, linear branching structures as in the test case. C) Incorrect. Lobular carcinoma in situ is a proliferation of small, uniform cells that distend the lobules. It is not associated with any specific mammographic findings, and calcifications are rare. D) Incorrect. Adenosis is due to proliferation of the breast lobules. When it is associated with fibrosis, it is referred to as sclerosing adenosis. The fibrosis around the lobules distorts the acinar structures into compressed elongated shapes. As a result, the calcifications may have a linear branching distribution, rather than the uniform, round morphology and lobular configuration usually associated with adenosis. Adenosis rarely appears as a mass on mammography. Calcifications are a more common presentation. Although the linear calcifications in this case resemble those of sclerosing adenosis, the presence of a spiculated mass does not support the diagnosis. E) Incorrect. Secretory disease, also known as ductal ectasis, is a condition of unknown etiology. It begins in the peri menopausal or postmenopausal period. The walls of the larger ducts often a subareolar location undergoes hyalinization and atrophy with dilation of the educt lumen. Secretions trapped in the duct can calcify. The calcifications are solid, relatively large because they occur in the larger ducts, and often have rod-like appearance. The rod-like appearance helps to distinguish them from the smaller, discontinuous branching calcifications of ductal carcinoma in situ. 6 American College of Radiology
- 7. Section X – Breast Radiology Figure 4A 402. A 42-year-old woman presents with a palpable lump. You are shown a craniocaudal view from a mammogram (Figure 4A) and one view of a sonogram (Figure 4B). Which one of the following is the MOST likely diagno- sis? A. Complex cyst B. Intraductal papilloma C. Hematoma D. Fibroadenoma E. Fat lobule Diagnostic In-Training Exam 2003 7
- 8. Section X – Breast Radiology Figure 4B 8 American College of Radiology
- 9. Section X – Breast Radiology Question #402 Findings: The mammogram shows a solitary partially well defined mass with partial obscured margins. The ultrasound shows a well-defined oval shaped, hypoechoic mass AND a small tubular structure along the posterior margin of the mass. This tubular structure is the duct. Rationales: A) Incorrect. A complex cyst is a cyst with both cystic and solid components, such as an intracystic papilloma, cavitating carcinoma or intracystic carcinoma. The appearance of the ultrasound does not show a fluid and solid components within a cyst. (pp. 675 No AM Clinics) B) Correct. The ultrasound shows a solitary hypoechoic well defined mass with “a tail” which represents the duct. This is the sign to look for to help rule in B as the answer. A malignant lesion is also a possibility but not on the list. C) Incorrect. Hematoma can produce a mass that is hypoechoic on ultrasound. One can often solicit a trauma history from the patient though. Therefore, since this was not the presentation, this is not the most likely choice. D) Incorrect. Fibroadenoma. Because this patient is young enough to be pre-menopausal, she could present with a fibroadenoma. However, they arise from the lobular structures in the breast, and are therefore not intraductal. E) Incorrect. Fat lobules on mammography are radiolucent. Moreover, this lesion is hypoechoic in that it is lower in echogenicity than the surrounding fat. Therefore, this is not a possible choice. Citations: Bassett LW. “Imaging of Breast Masses” Breast Imaging. The Clinics of North America. July 2000. pp. 669-691. Diagnostic In-Training Exam 2003 9
- 10. Section X – Breast Radiology Figure 5B Figure 5A 403. You are shown mammograms of each breast of a 59-year-old asymptomatic female (Figures 5A to 5F). No abnormality was seen on a sonogram. Which one of the following is the next BEST step? A. 6-month follow up exam B. Routine screening C. Biopsy D. 3-month follow up E. Repeat ultrasound 10 American College of Radiology
- 11. Section X – Breast Radiology Figure 5D Figure 5C Diagnostic In-Training Exam 2003 11
- 12. Section X – Breast Radiology Figure 5F Figure 5E 12 American College of Radiology
- 13. Section X – Breast Radiology Question #403 Findings: The mammogram of this patient shows a noncalcified density with irregular margins. Rationales: A) Incorrect. Short-term interval (6-month) follow-up mammography is usually reserved for probably benign lesions in patients without prior mammograms. The lesion in this case does not fall into this category as does some circumscribed masses and some areas of asymmetric breast tissue. B) Incorrect. Additional mammographic imaging is not indicated since it would not likely provide any useful management information. C) Correct. The appropriate response for this case of a single, dominant mass with indistinct margins is to recommend biopsy D) Incorrect. As noted above, a short-term interval follow-up mammography is usually reserved for probably benign lesions in patients without prior mammograms. The lesion in this case does not fall into this category. E) Incorrect. Ultrasonography would be unlikely to provide any useful management information. The lesion has no mammographic characteristics to suggest a cyst. Moreover, many solid small masses are not visualized on sonography, especially in a fatty breast, in which the surrounding echotexture is low. The likelihood that a repeat sonogram would be positive is low. Diagnostic In-Training Exam 2003 13