

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Rickets
Semelhante a Rickets (20)
Mais de orthoprince
Mais de orthoprince (20)
Último
Último (20)
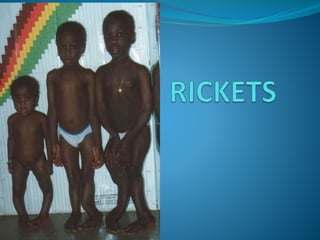
Rickets
- 2. Clinical condition in which there is inadequate mineralisation of growing bone. Primarily due to Vit D deficiecy or a disturbance in its metabolism. Rickets – children Osteomalacia bones of adults.
- 5. VIT.D DEFICIENCY decrease absorption of ca. & p from the gut decrease ca. level in blood increase PTH mobilization of ca. & po4 from bones and decrease tubular reabsorption of p in kidneys normal serum ca. & low serum po4 decrease ca. available for bones ca. & po4 will be far below 40 failure of calcification around the mature cart. cells and osteoblasts in the ostoeid tissue.
- 6. Normal bone growth THERE ARE 4 ZONES : 1.ZONE OF RESTING CARTILAGE : 1 layer 2.ZONE OF PROLIFERATING CART. : 6 layers 3.zone OF PROVISSIONAL CALCIFICATION "epiphyseal line " : the cart. cells in this layer become mature, they containe alkaline phosphatase release the phosphate in the matrix which already contains ca. & po4 in solution increase production of ca. & po4 once the production exceeds 40 precipitation of ca.phosphate in the matrix around the cartilage cells death of the cells. 4.ZONE OF BONE FORMATION : The layer of prov. calc. is invaded by capillaries and osteoblast which deposit a layer of organic bone matrix "osteoid tis.“ rapidly meniralized and the calcified cartilage ultimitly replaced by bone.
- 8. PATHOLOGY 1. The mature cartilage cells will not die and the proliferating zone will be formed of many layers and invades the adjacent zone of of provis. calc.- irrIegularity of epiphseal line. 2. The prov. calc. zone and newly formed ost. tis. will fail to calcify or will calcified irregularly. wide irregular frayed zone of non rigid tis. " RACHITIC METAPHSIS " is produced. 3. In the shaft the preformed bone is replaced by uncalcified ost. soft rarified cortical bone bone deformities & green stick fractures.
- 9. CAUSES Vitamin D deficiency Lack of sunlight exposure Dietry lack of meat & dairy products Malsbsorption Failure of 1,25 vit D synthesis Chronic renal failure Hyperphosphataemia & kidney damage Vit D dependent rickets ( type 1) - AR Inactivating mutation in 1,25,hydroxylase enzyme.
- 10. Vitamin D receptor defects Vit D dependent rickets type2 (AR) Mutation in vit D receptors Defects in phosphate metabolism Primary hypophosphataemic rickets(XLH) renal phosphate wasting. Fanconi syndromes Proximal renal tubular acidosis. Hypophosphatasia Mutation of bone specific ALP
- 11. NUTRITIONAL RICKETS VIT D DEFICIENCY 3-18 MONTHS LACK OF SUNLIGHT EXPOSURE & NO DIETARY SUPPLEMENTATION PROLONGED BREAST FEEDING CALCIUM DEFICIENT DIET BOTH VEGETARIANS WHO AVOID DAIRY PRODUCTS
- 12. GASTROINTESTINAL RICKETS ABSORPTION OF CALCIUM & VITAMIN D PREVENTED GLUTEN SENSITIVE ENTEROPATHY CROHNS DISEASE ULCERATIVE COLITIS SARCOIDOSIS SHORTGUTSYNDROMES LIVERDISEASE
- 13. X LINKED HYPOPHOSPHATEMIA MOST COMMON INHERITED ETIOLOGY X LINKED DOMONANT DISORDER DEFECT IN PHEX GENE(REGULATE TRANSPORT OF RENAL PHOSPHATES) RENALPHOSPHATE WASTING HYPOPHOSPHATEMIA RICKETS SHORT STATURE DENTAL ABSCESSES
- 14. McCUNE-ALBRIGHT SYNDROME HYPOPHOSPHATEMIC RICKETS CAFÉ AU LAIT SPOTS PRECOCIOUS PUBERTY FIBROUS DYSPLASIA OF MULTIPLE LONG BONES CONSTITUTIONAL ACTIVATION OF C-AMP-PKA SIGNALING PATHWAY DUE TO GENETIC DEFECTS IN G SIGNALING PROTEINS
- 15. 1 ALPHA HYDROXYLASE DEFICIENCY VITAMIN D DEPENDENT RICKETS <24WKS OF AGE WEAKNESS PNEMONIA SEIZURES BONEPAIN BONE CHANGES OF RICKETS
- 16. END ORGAN INSENSITIVITY 3 TO 30 FOLD HIGHER THAN NORMAL VALUE OF 1,25(OH)2VITD3 NEAR TOTAL LOSS OF HAIR FROM HEAD & BODY
- 17. FANCONIS SYNDROME(RENAL TUBULAR ABNORMALITY) FAILURE OF RENAL TUBULAR ABSORPTION OF MANY MOLECULES SMALLER THAN 50Da KIDNEYS LOSE CALCIUM,PHOSPHATE,MAGNESIUM, BICARBONATE,SODIUM,POTASSIUM,GLUCOSE, URIC ACID AND SMALL AMINOACIDS SHORT WITH RICKETS & DELAYED BONE AGE HYPOPHOSPHATEMIA,METABOLIC ACIDOSIS,RENAL OSTEODYSTROPHY(DECREASED CALCIUM AND PHOSPHATE REABSORPTION)
- 18. HYPOPHOSPHATASIA . ALP DEFICIENCY . 1 PER 1 LAKH POPULATION AUTOSOMAL RECESSIVE CONDITION MUTATION IN ALP GENE IN CHROMOSOME 1 ABNORMAL MINERALISATION OF BONE PATHOLOGICAL FRACTURES LOSS OF TEETH FAILURE TO THRIVE,RAISED INTRACRANIAL PRESSURE & CRANIOSYNOSTOSIS
- 19. PERINATAL LETHAL FORM CHILDHOOD FORM PRESENTS WITH RICKETS AT 2 OR 3 Yrs WITH REMISSION IN ADOLESCENCE ADULT FORM-MILD OSTEOMALACIA WITH PATHOLOGICAL FRACTURES
- 20. RENAL OSTEODYSTROPHY BONY CHANGES ACCOMPANYING ESRD RF HYPERPHOSPHATEMIA HYPOCALCEMIA SECONDARY HYPERPARATHYROIDISM SUBPERIOSTEAL EROSIONS & BROWN TUMORS RICKETS VARUS OR VALGUS DEFORMITY AT THE KNEE OR ANKLES
- 21. CLINICAL FEATURES OF RICKETS Delayed milestones Irritable child Lethargy & hypotonia Stunted growth
- 22. Rickets: signs Skull Craniotabes Frontal and parietal bossing, flat occiput Anterior fontanelle is large with delay in closure.
- 23. Chest Rosary Harrison’s sulcus Pigeon chest
- 24. Extremities: Widening of wrist, Bowing of legs, Knock knee
- 27. “POT BELLY “ due to hypotonia of abdominal muscles & intestine. Downward displacement of the liver & spleen.
- 28. Investigations X-RAYS The X-RAYS of the wrists is best for early diagnosis 1.The classic triad of rickets : Broadening Cupping (concave) Fraying ( irregular) 2.Increase distance between the distal ends of radius & ulna and the metacarpal bones .
- 29. 3.Demeniralization of the shaft “ hypodensity” 4.Fractures & deformities may be present LOOSER’S ZONE pseudo # occuring at the site of stress.
- 30. SUBPERIOSTEAL EROSIONS & BROWN TUMOR IN RENALOSTEODYSTROPHY SUBPERIOSTEAL EROSIONS-LATERAL ASPECT OF DISTAL RADIUS & ULNA & MEDIAL ASPECT OF PROXIMAL TIBIA.
- 31. Biochemical findings NUTRITIONAL RICKETS S . Ca - low / normal S . Posphorus – low S . ALP - High PTH – Raised 25(OH)D - low
- 32. VDRR is suspected when rachitic patients fail to respond to Vit D & calcium. 1,25(OH)2D raised 3-30 FOLD
- 33. Hypophosphataemic rickets high ALP, low phosphorus normal 25(OH)D & 1,25(OH)D
- 34. 1 ALPHA HYDROXYLASE DEFICIENCY LOW CALCIUM AND PHOSPHORUS HIGH ALP & PTH NORMAL 25-HYDROXY VITAMIN D3 MARKEDLY DECREASED LEVEL OF 1,25(OH)2VITD3
- 35. Treatment of rickets NUTRITIONAL RICKETS Adequate exposure to sunlight. Supplementation of vit D in diet. Therapeutic doses of vit D 200-600 units/day or As single IM inj of 600000 IU induces rapid healing. If line of healing ( sclerosis on the metaphyseal side of growth plate) is not seen after 3-4 weeks , same dose is repeated.
- 36. GASTROINTESTINAL RICKETS RECTIFY THE UNDERLYING GI PROBLEM
- 37. HYPOPHOSPHATEMIC RICKETS phosphate supplements – 2-3 gm/day & active vit D metabolites .[1,25(OH)2D 0.25-1.5microgm daily]
- 38. 1 ALPHA HYDROXYLASE DEFICIENCY ORAL ADMINISTRATION OF ACTIVATED VITAMIN D3
- 39. END ORGAN INSENSITIVITY CANNOT BE COMPLETELY CURED VERY HIGH DOSES OF VITAMIN D IV HIGH DOSES OF CALCIUM FOLLOWED BY ORAL SUPPLEMENTATION
- 40. FANCONI SYNDROME SIMILAR TO X LINKED HYPOPHOSPHATEMIA- ORAL PHOSPHATE & VITAMIN D ELECTROLYTE IMBALANCE SHOULD BE TREATED
- 41. HYPOPHOSPHATASIA NO SATISFACTORY MEDICAL TREATMENT BONE MARROW TRANSPLANTATION
- 42. RENAL OSTEODYSTROPHY DIETARY PHOSPHATE RESTRICTION PHOSPHATE BINDING AGENTS CALCITRIOL RENAL TRANSPLANTATION
- 43. Orthopaedic treatment Conservative – deformities correct spontaneously as rickets heals & with splinting. Operative – after 6 months of medical treatment . Corrective osteotomies
- 44. THANK YOU