
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (18)
Semelhante a Viral hepatitis 2013
Semelhante a Viral hepatitis 2013 (20)
Mais de Mario Mondelli
Último
Último (20)
Viral hepatitis 2013
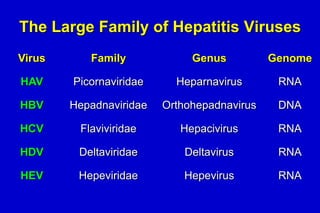
- 1. The Large Family of Hepatitis Viruses Virus Family Genus Genome HAV Picornaviridae Heparnavirus RNA HBV Hepadnaviridae Orthohepadnavirus DNA HCV Flaviviridae Hepacivirus RNA HDV Deltaviridae Deltavirus RNA HEV Hepeviridae Hepevirus RNA
- 2. HAV
- 3. Geographical Distribution of HAV Infection Prevalence of anti-HAV High Intermediate Low Very low
- 4. n. of cases Cases of Hepatitis A in Italy, 1987-2005 11000 10000 9000 8000 7000 6000 5000 4000 3000 2000 1000 0 Year
- 5. HAV: Mode of Transmission • Person-to-Person contacts (intrafamiliar, sexual, kinder garden) • Contaminated food or water (raw seafood, clams, mussels) • Blood exposure (very rare: blood transfusion)
- 6. HAV in Biological Fluids Stool Serum Saliva Urine 100 102 104 106 Infectious doses/ml Source: Viral Hepatitis and Liver Disease 1984;9-22 J Infect Dis 1989;160:887-890 108 1010
- 7. HAV Infection: Typical Serological Profile Symptoms Anti-HAV IgG Titre ALT HAV Faeces 0 1 anti-HAV IgM 2 3 4 5 Months after exposure 6 12 24
- 8. Hepatitis A – Clinical Presentation • Incubation: – Mean 30 d (15-50 d) • Jaundice by age class: – <6 a., <10% – 6-14 a., 40%-50% – >14 a., 70%-80% • Complications: – Fulminant hepatitis (rare) – Cholestasis – Long-term ALT fluctuations with virus shedding • Evolution to chronic infection: No
- 9. Prophylaxis • Improve hygiene, sewage, safe water supply • At least 4 different types of inactivated vaccine plus one recombinant in combination with HBV • Post-exposure prophylaxis with normal immunoglobulin which must contain antibodies to HAV
- 10. Who Should be Vaccinated Recommended to: all children leaving in endemic areas persons at risk of acquiring HAV: travellers to endemic areas, militaries, food workers, contacts with patients
- 11. HEV
- 12. Geographical Distribution of Cases of Hepatitis E Cornwall Sporadic cases in Spain, Italy, France, US…
- 13. Epidemiology of HEV Infection • Large epidemics described in the past (New Delhi 1955; Burma 1976; Algeria 1980; Messico 1986…) associated with faecal contamination of drinking water. • Human transmission extremely rare • History of travel in endemic areas • Game meat eating (UK)
- 14. Hepatitis E: a Zoonosis ? • Anti-HEV detected in pigs, poultry, dogs, rats, and cattle presente in both industrialized and developing countries: strongly suggestive of an animal reservoir. • Animal HEV strains genetically correlated with human HEV strains. and epidemiologically • Genetically homologous HEV strains detected in human faeces and pigsty sewages. • Cross-species infection possible: pig primate pig. • Prevalence of anti-HEV higher in rural than in urban areas. • HEV infection associated with eating game meat
- 15. HEV Infection: Typical Serological Profile Symptoms ALT Titre IgG anti-HEV IgM anti-HEV Virus in stools 0 1 2 3 4 5 6 7 8 Weeks after Exposure 9 10 11 12 13
- 16. HEV: Clinical Evolution Acute Illness Immune suppression? Chronic Infection (prevalence unkown) Recovery 20% pregnant women Fulminant Hepatitis Death
- 17. Hepatitis E: Clinical Presentation • Incubation: Mean 40 d (range 15-60 d) • Mortality: 1%-3%, pregnant 15%-25% • Severity of symptoms: Increase with age • Cronic evolution: Rare (immunosuppressed +++)
- 18. Prophylaxis of Hepatitis E • Improve hygiene as for HAV • A safe and effective vaccine is available but not commercially available yet because financially not profitable.
- 19. General Prophylactic Measures for Travellers to Countries Where HEV Is Endemic • Avoid unsafe water and seafood. Avoid eating game meat from endemic regions. • Commercially available Ig preparations do not usually contain antibodies to HEV. • The efficacy of Ig preparations from convalescent or immune patients is unknown • Vaccination when available
- 20. Hepatitis B: Essential Epidemiology World population 7 billions About 2 billions have markers of exposure to HBV Every year about 4 millions new HBV infections 400 millions are chronic HBV carriers Mortality: about 1 million/yr Source: WHO
- 21. HBV Infection: Clinical Significance • Most frequent cause of cirrhosis and HCC • East: • Prevalence 5-20% of the general population • Perinatal or early childhood infecton • West: • Prevalence 0.2-1% of the general adult population • 5-10% of all chronic liver diseases
- 22. Excess Mortality Associated with Chronic HBV Infection Survival curves of total mortality stratified by HBsAg status 1.0 Survival HBsAg(-) n=19,655 HBsAg(+) n=4,155 0.9 P<0.01 0.8 0 1 2 3 4 5 6 7 Year of Follow-Up Iloeje U, et al. Gastroenterology 2006; 130:678–686 8 9 10 11 12
- 23. Crude Mortality Rate by Sex and HBsAg Status in Haimen City, China Mortality Rate per 100,000 PYs 1500 1000 Liver deaths HCC CLD 500 0 HBsAg+ Males Chen G, et al., Int J Epidemiol 2005;34:132-7 HBsAg+ Females HBsAgMales HBsAgFemales
- 24. HBV
- 25. HBV Ultrastructure DNA polymerase HBV DNA Envelope (HBsAg) Nucleoproteine core (HBcAg) HBsAg HBeAg
- 26. HBV Life Cycle Covalently closed circular DNA cccDNA Nuclear transport Binding and penetration cccDNA Uncoating NUCLEUS Re-entry MINICHROMOSOME Pregenomic RNA HBV RNA HBV polymerase Envelope protein L, M, S Pre-core protein Core protein Virion Secretory pathway HBsAg HBeAg
- 27. Worldwide Distribution of HBV Genotypes F A B C A G D D H D G D E F D D C Ba F C Bj A (Fung & Lok, Hepatology 2004;40:790-2)
- 28. HBV: Mode of Transmission • Sexual • Parenteral • Perinatal
- 29. Concentration of HBV In Biological Fluids High Blood Exudates Moderate Low/Absent Seminal fluid Vaginal secretions Saliva Urine Stools Sweat Tears Maternal milk
- 30. N. of Cases of Hepatitis B in Italy, 1987-2005. Source: ISS N. of cases 4000 3000 2000 1000 0 Year 2005: dati provvisori
- 31. Clinical Evolution of HBV Infection Acute Infection 90% neonates ~0.1% 25–30% infants <1% adults %? Chronic Infection 15–40% Fulminant Hepatitis Chronic Hepatitis Inactive Carrier Cirrhosis 2 - 4%/year Decompensation EASL Consensus Guidelines. J Hepatol 2003; Lok, McMahon. Hepatology 2004 (AASLD Guidelines) Death Transplant HCC
- 32. Risk of Chronic Infection Decreases with Age 100 Risk % 75 50 25 0 Neonates Toddlers Children Adults
- 33. Hepatitis B – Clinical Presentation • Incubation: Mean 60-90 d (range 45-180 d) • Jaundice: o <5 a., <10%; o 5 a., 30%-50% • Infezione cronica: <1%-90%: age major factor • Mortality from chronic liver disease:15%-25%
- 34. Virological and Serological Markers of Acute HBV Infection Jaundice Symptoms HBeAg ALT Anti-HBe Titre HBV-DNA Anti-HBc HBsAg Anti-HBs IgM anti-HBc 4 8 12 16 20 24 28 32 36 40 Weeks after Exposure 52
- 35. Chronically-Evolving Hepatitis B HBV DNA Acute (6 mos.) Chronic (yrs) HBeAg anti-HBe HBsAg Titre Total anti-HBc IgM anti-HBc 0 4 8 12 16 20 24 28 32 36 Weeks after Exposure 52 years
- 36. Natural Course of Chronic HBV Infection Perinatal Transmission Immune tolerance HBsAg+ HBeAg+ HBV DNA↑↑↑ ALT normal Adulthood Transmission HBeAg positive CHB HBsAg+ HBe Ag+ HBV DNA↑↑↑ ALT↑↑ (Patient age; gender; BMI, duration of hepatitis, baseline ALT, histology, HBV DNA load, genotype) Progressive Liver Damage Cirrhosis HCC Liver failure Death from liver disease Resolved Hepatitis HBsAg negative Seroconversion Reactivation Inactive Carrier HBeAgHBsAg+ Anti-HBe+ HBV DNA ↓ Normal ALT HBeAg neg CHB HBeAgHBsAg+ Anti-HBe+ HBV DNA ↑↑ ALT↑↑
- 37. Natural History of Inactive HBsAg Carriers Incidence per 100 person years of major events De Franchis 1993 Bellentani 2002 Manno 2004 Hsu 2002 Europe Europe Europe Asia • Number of patients 68 46 296 189 • Median follow-up (yrs) 10 9 29 8 • HCC 0 0 0.02 0.19 • Liver-related death 0 0 0.01 0 1.0 0.9 1.0 0.6 • area • HBsAg loss
- 38. ALT Profiles in Chronic HBV Infection 400 ALT IU/l 300 200 100 0 400 ALT IU/l 300 200 100 0 Years
- 39. Factors Influencing Progression of HBV Infection • Demographics: – Age – Gender – Family history (HCC) • Environmental/Metabolic: – – – – Alcohol Aflatoxin NAFLD (?) Tobacco (?) • Host immune response • Viral factors
- 40. Natural History of HBV Cirrhosis 5-year rate of HCC: 9% 5-year rate of decompensation: 16%. 5-year survival: 86% 5-year survival after decompensation: 28%. G. Fattovich, Seminars Liver Disease 2003
- 41. HCC Is Common and Increasing • 5th most common cancer in men and 7th in women • Most of the burden (85%) borne in developing countries. Incidence: – >10/100,000: Sub-Saharan Africa, South-East Asia – 5-10/100,000: Eastern, Southern & Western Europe, South Africa, Caribbean – <5/100,000: Northern Europe, the Americas, North Africa, Australia, New Zealand • Peak at 70 yrs of age, rare <40 • HCV-related HCC fastest rising cause of cancer-related deaths in the Western world World Health Organization. Available at: http://www.who.int/whosis/en/. Accessed October 6, 2008.
- 43. REVEAL: High HBV Viral Load is Associated with Increased Incidence of Cirrhosis Cumulative incidence liver cirrhosis All participants (n=3,582) Baseline HBV DNA Level ≥106 ≥104–<105 103–<104 300–103 <300 .4 .3 .2 .1 0 0 1 2 3 4 5 6 7 8 Year of follow-up Iloeje UH, et al. Gastroenterology 2006;130:678–686 9 10 11 12 13
- 44. REVEAL: High HBV Viral Load is Associated with Increased Incidence of HCC All participants (n=3,653) Cumulative incidence of HCC .16 Baseline HBV DNA Level ≥106 ≥104–<105 103–<104 300–103 <300 .14 .12 .1 .08 .06 .04 .02 0 0 1 2 3 4 5 6 7 8 Year of follow-up Chen CJ, et al. JAMA 2006; 295:65–73 9 10 11 12 13
- 45. Treatment Options in Chronic Hepatitis B Decision to treat IFN (PegIFN alfa-2a) Nucleos(t)ide analogues
- 46. Potency and Genetic Barrier for Resistance of Current Anti-HBV Drugs Potency LDT LAM ETV TDF FTC ADF IFN Genetic Barrier Ruiz-Sancho A, et al. Expert Opinion Biol Ther 2007
- 47. Cumulative Rates of Resistance With Oral Agents in Nucleos(t)ide-Naϊve Patients Not head-to-head trials; different patient populations and trial designs Yr 1 Yr 2 Yr 3 Yr 4 Yr 5 Yr 6 Drug Generation 1st 2nd 3rd LAM 24% 38% 49% 67% 70% ADV 0% 3% 11% 18% 29% LdT ETV TDF 4% 0.2% 0% 17% 0.5% 0% 1.2% 0% 1.2% 1.2% EASL. J Hepatol. 2009;50:227-242. Tenny DJ, et al. EASL 2009. Abstract 20. Marcellin P, et al. AASLD 2009. Abstract 481. Heathcote E, et al. AASLD 2009. Abstract 483. 1.2%
- 48. Natural Life Cycle of a Chronic HBsAg Carrier HBsAg+ Mother X Infected Neonate Female Chronic HBsAg Male Carrier
- 49. Prevalence of HBsAg Carriers among 6 Year-Old Children in Taiwan Prevalence (%) 12 10.5 10 8 6.3 6 4 1.7 2 0 1989 1991 Year studied Hsu et al. J Infect Dis 1999;179:367-70 1993
- 50. Average Annual Incidence of Hepatocellular Carcinoma in Children Aged 6-14 years before and after Introduction of the HBV Immunisation Programme Average annual incidence/100,000 10.8 - 0.70 0.57 0.6 0.36 0.4 0.2 01981-1986 1986-1990 Years Chang et al. N Engl J Med 1997;336:1855-9 1990-1994
- 51. Italian Strategy for Hepatitis B Vaccination Age 24 24 12 12 0 0 1991 Years 2003 STOP Vaccination of teens
- 52. Incidence of Acute Hepatitis B by Age Class SEIEVA, 1985-2003 45 40 35 30 25 20 15 10 5 0 Vaccinazione Anti-HBV 0-14 15-24 > 24
- 53. Impact of Hepatitis B Vaccination Prevalence of anti-HBc in military recruits 16.8% 5.8% <1% 1981 Journal of Hepatology 1997 1990 2001
- 54. Hepatitis D (Delta) Virus antigen HBsAg RNA
- 55. Geographical Distribution of HDV Infection Taiwan Pacific Islands Prevalence of HDV High Intermediate Low (ITALY ~6%, 2000) Very low No Data
- 56. HDV: Replication and Mode of Transmission • Satellite virus: requires HBV for replication • Percutaneous exposure – IVDU • Mucosal exposure – Sexual contacts
- 57. Hepatitis D – Clinical Presentation • HBV-HDV Coinfection – Severe acute hepatitis – Relatively low risk of chronic evolution • HDV Superinfection of a Chronic HBV Carrier – High probability of chronic HBV-HDV co-infection – High probability of developing severe chronic liver disease
- 58. Virological and Serological Profile of HBV–HDV Coinfection Symptoms Titre ALT ↑ anti-HBs IgM anti-HDV HDV RNA HBsAg Total anti-HDV Time after Exposure
- 59. Virological and Serological Profile of HBV–HDV Superinfection Symptoms Total anti-HDV Titre ALT HDV RNA HBsAg IgM anti-HDV Time after Exposure
- 60. HDV: Prophylaxis • Primary prophylaxis • Hepatitis B vaccine prevents HDV infection
- 61. About 170 Millions of Hepatitis C Carriers Woldwide 3-4 millions new infections/year Prevalence > 10% 2.5%-10% 1%-2.50% NA World Health Organization 2008. Available at: http://www.who.int/ith/es/index.html.
- 62. Distribution of Chronic HCV Carriers in Geographical Areas The prevalence of chronic HCV carriers differs in various countries (0.4-22%). • Italy shows an intermediate value: 1-2% • Areas of very high endemicity (>35%, South) • North-South gradient • Cohort effect caused by epidemics due to injecting therapies in the 40’s and 50’s. • I.V. treatment of Schistosomiasis in Japan (1920-40) 62
- 63. 2.5 HCV Infection: Incidence/100,000 persons year 2 1.5 1 0.5 0.4 0 ‘91 ‘92 ‘93 ‘94 ‘95 ‘96 ‘97 ‘98 ‘99 ‘00 ‘01 ‘02 ‘03 ‘04 ‘05 ‘06 ‘07 ‘08 Year Courtesy from A. Mele, ISS; SEIEVA 1991-2008
- 64. Age-Specific Prevalence of anti-HCV by Age Class and Geographical Area in Italy % 35 Sud 30 25 20 Centro 15 10 Nord 5 0 < 30 > 60 30-39 40-49 Age class 50-59
- 65. Residual Risk/Year to Acquire HCV Infection Following NAT Screening (Cases/106 blood units, 95% C.I. ) 2004 HCV HBV 2005 2006 2007 2008 2009 0.3 0.2 0.2 0.2 0.1 0.1 (0.1-0.6) (0.1-0,4) (0.1-0.3) (0.1-0.3) (0.1-0.2) (0.1-0.2) - - 1.6 1.9 1.6 1.6 (0.3-1.8) (0.9-2.7) (0.6- 2.1) (0.6-2.1) Società Italiana di Medicina Trasfusionale e di Immunoematologia – Settore Ricerca & Sviluppo Gruppo Italiano per lo Studio delle Malattie Trasmissibili con la Trasfusione
- 66. Populations at Risk of HCV Infection • 27.000-29.000 new cases diagnosed every year in the EU. • M/F= 2/1. • Populations at risk: IVDU, HIV-infected persons, prison inmates, haemodialysis patients, migrants from high endemicity countries, surgery. • Sexual transmission is rare although promiscuity is considered a risk factor. 66
- 67. Risk of HCV Infection Following Invasive Procedures Type of surgery OR (95% CI) Minor O&G Orthopaedic Abdominal Cardiovascular Oral Ophtalmologic Urologic Other Endoscopy 3.0 (1.5-6.1) 12.1 (1.2-5.5) 3.5 (1.6-7.5) 7.0 (3.2-14.9) 4.1 (1.4-11.9) 2.8 (1.4-5.7) 5.2 (1.1-23.2) 0.8 (0.1-4.8) 3.3 (1.9-5.7) 2.1 (1.2-3.6)
- 68. Hepatitis C Virus Genome 5’ UTR C E1 E2 Nucleocapsid Envelope p7 NS2 NS3 ? NS2-NS3 autoprotease NS4a NS4b NS5a NS5b NS3 protease cofactor Serine protease, helicase, NTPase ? 3’ UTR RNA-dependent RNA-polymerase ? (binds to PKR)
- 69. Phylogenetic Tree of HCV and its Major Genotypes Nakano et al. Liver Int 2012;32:339-45
- 70. A Traditional HCV Vaccine Is Difficult to Produce 6 major genotypes, several subtypes, infinite possible variants!
- 71. Hepatitis C: Clinical Presentation • Incubation Mean 30-50 d (15-150 d) • Jaundice Rare (<10%) • Chronic evolution 60%-80% (asymptomatic) • Cirrhosis 10%-20% • Liver-related mortality 1%-5% (after >20 yrs)
- 72. Markers of HCV Infection Self-limited acute hepatitis Chronically Evolving Acute Hepatitis Anti-HCV anti-HCV Symptoms+/- HCV RNA HCV RNA Titre Titre Symptoms +/- ALT ALT 0 1 2 3 4 Mos. 5 6 1 2 3 Years Time after Exposure 4 0 1 2 3 4 Mos. 5 6 1 2 3 4 Years Time after Exposure
- 73. (Slow) Female sex, young age at infection Progression 30 years Normal Liver Acute Infection Chronic Infection (60-80%) Chronic Hepatitis Cirrhosis (20 %) (Fast) 20 years Alcohol, steatosis, IR, coinfections, age>45 yrs, male sex Modified from Lauer et al., N Engl J Med 2001;345:41-52. HCC (1-4%/yr)
- 74. IL28B Polymorphism Is a Powerful Host Prognostic Marker in Chronic Hepatitis C rs12979860 IL28B locus SNPs associated with spontaneous and treatment-induced HCV clearance in genotype 1 chronic hepatitis Ge et al., Nature 2009;461:399-401
- 75. Genetic Variation in IL28B and Spontaneous HCV Clearance % of HCV clearance by rs12979860 snp Thomas DL et al., Nature 2009;461:798–801
- 76. Factors Influencing the Development of Fibrosis • Age > 40 years • Male sex • Alcohol (oxydative stress) • Metabolism (steatosis, IR, metabolic syndrome) • Coinfections (HIV or HBV) • Iron overload (?)
- 77. Broad Differences in HBV and HCV Replication HBV1,2 Host cell Host cell cccDNA Host DNA HCV1,3 H Host DNA HCV RNA H Integrated DNA Nucleus Long-term suppression of viral replication Nucleus Definitive viral clearance and SVR Adapted from 1. Soriano V, et al. J Antimicrob Chemother 2008;62:1-4. 2. Locarnini S and Zoulim F. Antiviral Therapy 2010;15 (suppl 3):3-14. 3. Sarrazin C and Zeuzem S. Gastroenterology 2010;138:447-462.
- 78. What Does Recovery Mean for HCV Infection? • Prevent liver decompensation • Prevent liver cancer • Prevent death fom end-stage liver disease
- 79. Treatment of Chronic Hepatitis C PI + PegIFN/RBV (6-12 mos)[8-10] 100 70-75 SVR (%) 80 PegIFN/ribavirin (6-12 mos)[6,7] Interferon/ ribavirin (6-12 mos)[3,4] 60 40 20 Standard interferon (6 mos)[1] Standard interferon (12-18 mos)[2,3] 38-43 50-60 PegIFN monotherapy (6-12 mos)[5,6] 25-30 15-20 8-12 0 1991 1995 1998 2001 2011 1. Carithers RL Jr., et al. Hepatology. 1997;26(3 suppl 1):83S-88S. 2. Zeuzem S, et al. N Engl J Med. 2000;343:1666-1672. 3. Poynard T, et al. Lancet. 1998;352:1426-1432. 4. McHutchison JG, et al. N Engl J Med. 1998;339:1485-1492. 5. Lindsay KL, et al. Hepatology. 2001;34:395-403. 6. Fried MW, et al. N Engl J Med. 2002;347:975-982. 7. Manns MP, et al. Lancet. 2001;358:958965. 8. Poordad F, et al. N Engl J Med. 2011;364:1195-1206. 9. Jacobson IM, et al. N Engl J Med. 2011;364:2405-2416. 10. Sherman KE, et al. N Engl J Med. 2011;365:1014-1024.
- 80. Standard Dual Treatment of HCV Infection Sustained Virological Response (%) Peginterferon + Ribavirin 100 80 60 PegIFN- 2a/RBV PegIFN- 2b/RBV 40 20 0 1 2-3 Genotype Fried MW, et al. N Eng J Med. 2002;347:975-982. Manns MP, et al. Lancet 2001;358:958-965.
- 81. IL28B SNPs in 670 Patients with Chronic Hepatitis C: the HCV-AIFA Italian Study p N.S. 90 80 SVR % 70 p 0.00001 79% 81% 70% 67% p 0.03. p N.S. 83% 71% 60 50 rs12979860 C/C 40 33% 29% 30 rs12979860 C/T or T/T 20 10 103 234 0 Genotype 1 (337 pts) 63 102 Genotype 2 (165 pts) 40 55 Genotype 3 (95 pts) 6 24 Genotype 4 (30 pts)
- 82. HCV Replication and Directly-Acting Anti-Virals NS5B Polymerase Inhibitors NS3/4 Protease Inhibitors
- 83. HCV Protease and Co-Factor NS4A Active site “catalytic triad“ NS4A Zn finger
- 84. PI Registered for Triple Therapy of HCV G1 Infection in Combination with PEG-IFN + RBV • Telaprevir: NS3/4A • Boceprevir: NS3 – High risk of resistance if used without PEGIFN/RBV backbone
- 85. Percent SVR in Patients With Genotype 1 Naïve and Non-Responders to SOC 100 100 SOC 80 80 SOC + Telaprevir or Boceprevir 63-75[1-2] SVR (%) SVR (%) 59-66[3-4] 60 38-44[1-2] 40 60 40 17-21[3-4] 20 20 0 Naïve Experienced 0 Naïve Experienced 1. Poordad F, et al. N Engl J Med 2011;364:1195-206. 2. Jacobson IM, et al. AASLD 2010. Abstract 211. 3. Bacon BR, et al. N Engl J Med. 2011;364:1207-17. 4. Foster GR, et al. APASL 2011. Abstract 1529.
- 86. The HCV Polymerase Has the Shape of a Closed Right Hand Thumb Fingers Active Site Palm
Notas do Editor
- Once a decision has been made to treat a patient with chronic hepatitis B, therapy must be selected from either peginterferon alfa-2a or 1 of the oral agents, namely, entecavir and tenofovir.
- ADV, adefovir; ETV, entecavir; LAM, lamivudine; LdT, telbivudine; TDF, tenofovir. Exposure to oral anti-HBV agents presents a risk of evolving drug resistance. Cumulative rates of resistance differ between agents, with higher rates reported with the use of older agents. In nucleos(t)ide-naive patients, treatment with lamivudine was associated with relatively high rates of resistance: 24% at Year 1, rising to 70% by Year 5. Reported rates of resistance were lower with use of the second-generation drugs adefovir and telbivudine. Data on telbivudine are limited to 2 years of follow-up, at which point resistance was reported in 17% of patients on first-line therapy. The cumulative rate for adefovir was 29% at Year 5. The resistance profile of the third-generation agents entecavir and tenofovir is different. For tenofovir, 3-year follow-up of naive patients found no evidence of emergent resistance. For entecavir, the rate of resistance in comparable populations remained low: 1.2% at Year 6 of therapy. For more information, go online to http://www.clinicaloptions.com/Hepatitis/Conference%20Coverage/Copenhagen%202009/Tracks/HBV%20Treatment/Capsules/20.aspx
- HCV, hepatitis C virus; NA, not available. Currently, the World Health Organization estimates that at least 170 million persons are chronically infected with HCV, and every year another 3-4 million people are newly infected. This slide shows how the prevalence of chronic HCV varies throughout the world varies. Areas of particularly high prevalence include South America, Central Africa, and Central Asia.
- BOC, boceprevir; GT1, genotype 1; SOC, standard of care; SVR, sustained virologic response; TPV, telaprevir. This slide is a summary of data. It is clearly not a head-to-head comparison but an illustration of the data for boceprevir and telaprevir in patients who were treatment naive or previous nonresponders. If one compares the blue box on the left with the blue box on the right, one can see that in treatment-naive patients, approximately 30% more patients can be cured with the addition of either boceprevir or telaprevir to peginterferon/ribavirin. The difference is even more pronounced in previous nonresponders. Here one can see success rates of 17% to 21% with repeat peginterferon/ribavirin treatment; however, a 59% to 66% SVR rate can be attained in these previous nonresponders when a protease inhibitor is added. So you clearly see how important, especially for patients who have been previously unsuccessfully treated, the addition of a protease inhibitor will be.