
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Orthopedic considerations in neuromuscular disorder
Similar to Orthopedic considerations in neuromuscular disorder (20)
Recently uploaded
Recently uploaded (20)
Orthopedic considerations in neuromuscular disorder
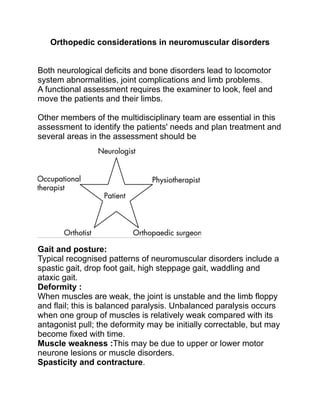
- 1. Orthopedic considerations in neuromuscular disorders Both neurological deficits and bone disorders lead to locomotor system abnormalities, joint complications and limb problems. A functional assessment requires the examiner to look, feel and move the patients and their limbs. Other members of the multidisciplinary team are essential in this assessment to identify the patients' needs and plan treatment and several areas in the assessment should be Gait and posture: Typical recognised patterns of neuromuscular disorders include a spastic gait, drop foot gait, high steppage gait, waddling and ataxic gait. Deformity : When muscles are weak, the joint is unstable and the limb floppy and flail; this is balanced paralysis. Unbalanced paralysis occurs when one group of muscles is relatively weak compared with its antagonist pull; the deformity may be initially correctable, but may become fixed with time. Muscle weakness :This may be due to upper or lower motor neurone lesions or muscle disorders. Spasticity and contracture.
- 2. Cerebral palsy : The term cerebral palsy includes a group of disorders that result from non‐progressive brain damage Children usually have delayed developmental milestones and later present with a number of problems, including ataxia, dystonia, athetosis, weakness and spasticity. With better management, patients with cerebral palsy are living longer orthopaedic manifestations characteristic of CP primary • abnormal tone • loss of motor control • impaired balance • spasticity • (hypotonia) • (dyskenesias such as chorea and athetosis) secondary (growth and spasticity related) • contractures: starts as dynamic contractures, become static with time (continuous muscle contraction results in shortening) and growth (growth of bones occurs at a faster longitudinal rate than muscles in spastic cerebral palsy) • upper extremity deformities • hip subluxation and dislocation
- 3. • spinal deformity • foot deformities • gait disorders • fractures often associated with non-ambulatory secondary to low bone mineral density. GMFCS Management : physical therapy, bracing/orthotics, medications for spasticity • spasticity control : • botulinum - A usually lasts 2-3 months • used to maintain joint motion during rapid growth when a child is too young for surgery • often injected into gastrocnemius • helpful treatment in dynamic contractures; little benefit with static contractures • baclofen • intra-thecal administration is preferred route to avoid cognitive impairment seen with oral administration. • Intra-thecal baclofen tends to be used for non-ambulatory CP. Spastic hip disorder vs DDH There is adductor contracture ,extreme anteversion and increased neck shaft angle. Level I Near normal gross motor function, independent ambulator Level II Walks independently, but difficulty with uneven surfaces, minimal ability to jump Level III Walks with assistive devices Level IV Severely limited walking ability, primary mobility is wheelchair Level V Nonambulator with global involvment, dependent in all aspects of care
- 4. Acetabular deficiency posterior superior as apposed to ddh which is anterior. Huge relation to GMFCS. GMFCS 1 LESS THAN 10% GMFCS 5 MORE THAN 80% Hip at risk managed surgically if MI >25 ,increased valgus ,excessive anteversion and shallow acetabulum. Adductor tightness carefully looked for as it is progressive. If MI MORE THAN 50 HIGH IN GMFCS 5 this requires bone and soft tissue surgery. Often younger child tend to have recurrence even if they have proper care after surgery. Pelvic osteotomy: sometime only VDRO is needed and sometimes dega osteotomy Dega leads to decrease in acetabular volume. Knees: exam is critical Popliteal angle is very important Hip/knee flexion contractures:
- 5. Big knee flexion contracture DFEO w/pt advancement as only hamstring lengthening will not be helpful. Intra op coorection to max 30 degree pop angle Becareful from over lengthening . Stiff rectus : some of patient can’t clear foot can’t bend knees from sit to stand Rectus transfer and release . Ankle/feet: important to know what to lengthen with the aid of silverskiiold test Equinus : strayer vs TAL KEEP IN MIND RECURRENCE IS VERY HIGH IN CHILD LESS THAN 8 YEARS 70% Equinovarus: most coomon in hemiplegic Also seen in high GMFCS QUADS most often children remain quite flexible and typically treated with orthotics Valgus hindfoot: if no pain can brace stretch and adaptive shoe wear. If they need surgery: soft tissue proceeders will not benefit Lateral column lengthening (evans/mosca) Address any malrotation and bunion they tend to be dorsal and painful. Gait: True vs apperant equinus : ▪ SEMLS surgery (Single-Event, Multi-Level Surgery) ▪ concept arose to limit multiple surgeries, anesthetics, and rehabilitation time for children
- 6. ▪ most successful when combined with a thorough gait lab assessment that predicts improvemenet in function with multiple level surgical interventions ▪ simple lengthenings can cause deterioration in gait when other contractures are "uncovered"; SEMLS management seeks to avoid these iatrogenic complications ▪ can be done on bilateral lower extremities in efforts to improve gait Upper extremity issues: typically internal roation of the shoulder,forearm pronation ,wrist flex/ulnar deviation thumb in palm. Best candidates for ue surgery: • Spastic • Reasonable intelligence/motivation • Stable trunk • Good hand propirioception • No fixed contravtures • Resonable hand function(placement and control). Casting , passive night stretch ,ot for mild contractures Transfere release depending on specific patteren.
- 7. Spine issue occurs mostly in quads : - Often very large hyperlordosis 2nd to hip flexion contractures Compensatory below rigid thoracic hyperkyphosis - Hyperkyphosis Young child with poor spinal extension Over several levels almost always flexible Any degree of pelvic obliquity should be addressed as this may be unresponsive to bracing and worsen with age. - Scoliosis 75% of quads Young age poor sitting balance pelvic obliquity increase risk Curve more than 40 Unresponsive to bracing Surgery if curve becomes inflexible or sitting balance tolerance decrease. Stroke : patients who have had a stroke may cont to improve upto 6 months after their vascular event; - patients with traumatic brain injury may improve upto 18 mo after injury to walk independently, the hemiplegic requires: - adequate balance to stand independently - hip flexion to advance the limb - normal strength of uninvolved side - normal proprioception - if the patient does not have these requirements, walking may not be a realistic goals Orthotic aims in stroke differ dramatically according to the time from onset.
- 8. In early stroke, orthoses may be used to challenge stability, optimise alignment and be used alongside physiotherapy to promote best recovery; in the chronic stages after stroke, they are more likely to be used to provide stability to maximise function. Intensive home stretching and physiotherapy are required, often with muscle relaxants and phenol treatment in some patients. Surgical treatment is frequently needed. The indications for surgery are: 1. Deterioration or uncontrollable spastic posture 2. Fixed deformity that interferes with function 3. Secondary complications such as bony deformities, dislocation of the hip and joint instability. Surgical options are limited and mainly consist of releasing tight muscles or lengthening tendons, augmenting weak muscles by tendon transfers and correcting of fixed deformities by osteotomy, arthrodesis. Treatment of principal limb deformities in stroke Deformi ty Orthotic intervention Surgery Foot Flaccid equinus Spring‐loaded dorsiflexion Lengthen tendo Achillis Foot Spastic equinova rus Limiting orthosis to eversion and dorsiflexion Lengthen tendo Achillis and transfer lateral half of tibialis anterior to cuboid Knee Flexion Knee–ankle–foot orthosis Hamstring release Hip Adducti on Seating adaptation Obturator neurectomy or adductor muscle release Shoul der Adducti on Positioning pillow Subscapularis release
- 9. The muscular dystrophies : These are a group of hereditary disorders of the skeletal muscle that produce progressive degeneration of the skeletal muscle and associated weakness. The X linked dystrophies such as Duchenne's( caused by absent dystrophin protein )and Becker's muscular dystrophy(dystrophin protein is decreased instead of absent). (DMD and BMD) are the most common dystrophies encountered in clinical. The major goal of early treatment is to maintain functional ambulation as long as possible. Orthopedic treatment : Patients with DMD are susceptible to the development of contractures and scoliosis. Stretching exercises and nightly bracing can help to prevent the contractures from becoming severe. At the age of 8–15 years, children with DMD have a sensation of locking of the knees. It is easier to keep children with DMD walking than to induce walking once they have stopped, therefore, contractures should be treated early to maintain ambulation, because, if it is Elbow Flexion Night orthosis Release elbow flexors Wrist Flexion Wrist orthosis Lengthen or release wrist flexors Finger s Flexion Night orthosis Lengthen or release flexors
- 10. maintained even for 1–2 years, it considerably benefits these children and delays the inevitable development of scoliosis and kyphosis. Three approaches are usually used to correct lower extremity contractures: 1. Ambulatory approach (early lower limb surgery): The goal here is to correct any contractures while the patient is still ambulatory. This is often needed early, between 4 and 6 years at the initial appearance of contractures, at the plateau of muscle strength or when there is difficulty maintaining an upright posture with the feet together. a three‐step approach to correct early contractures, consisting of bilateral tenotomy of the superficial hip flexors, aponeurectomy of the iliotibial band, and subcutaneous tenotomies of the knee and foot. 2. Rehabilitative approach: Surgery is performed at or just after the patient has lost the ability to walk, but with the intention that walking will resume. Walking and standing can be extended for a few years by the use of long leg orthoses in patients with DMD who reach the critical phase of loss of independent walking ability. Before the use of most orthoses, surgery is required to release the Achilles tendon alone or with superficial hip and medial knee flexors. 3. Palliative approach: This is used for treating contractures that interfere with shoe wear and comfortable wheelchair positioning. Even when a patient is too weak to walk, he should continue to stand using a standing frame or a stand‐up wheelchair. • physical therapy for range of motion exercises • adaptive equipment • power wheelchairs
- 11. • KAFO bracing. Scoliosis : neurogenic curve Usually by the age of 12–13 years, most children with DMD can no longer walk, and the progressive spinal deformity becomes the major problem, affecting sitting and causing breathing problems.
- 12. Three patterns of spinal deformity : begins with mild hyperlordosis progresses with general kyphosis and scoliosis with varying degrees of pelvic obliquity Conservative treatment is not effective. Bracing and wheelchair support may slow the progression but spinal fusion is ultimately required. progresses 1° to 2° per month starting at age 8 to 10 years. curve progresses rapidly from age 13 to 14 years. Treatment nonoperative • bracing is contraindicated may interfere with respiration • operative : early PSF with instrumentation • indications : curve 20-30° in nonambulatory patient treat early before pulmonary function declines can wait longer ~ 40° if responding well to corticosteroids • FVC drops ≤ 35% • rapidly progressive curve PSF with instrumentation to pelvis • indications curves ≥ 40° pelvic obliquity ≥ 10° lumbar curve where apex is lower than L1 anterior and posterior spinal fusion • rarely for stiff curves
- 13. Peripheral neuropathy: Disorders of the peripheral nerves may affect motor, sensory and autonomic nerves. Diabetic neuropathy is the most common cause of neuropathy The most common management problem is the diabetic foot, where treatment is aimed at skin care, and maintaining tissue integrity. Orthopaedic management of this group includes the treatment and prevention of ulcers and/or infection and the management of neuropathic joints. Ulcers in neuropathic feet develop because of associated ischaemia, abnormal loading/shear (due to foot deformity or tight Achilles tendons), inappropriate shoe wear or trauma. Surgery may include lengthening of the Achilles tendon to reduce forefoot loading, debridement of ulcers, total contact casting of the foot to equalize pressure distribution, removal of necrotic bone and revascularisation procedures. Nonoperative : total contact casting, shoewear modifications, first line of treatment • contact casting • • casts changed every 2-4 weeks for 2-4 months orthotics • Charcot restraint orthotic walker (CROW) boot can be used after contact casting shoe modifications
- 14. • double rocker shoe modifications will best reduce risk for ulceration at the plantar apex of the deformity medications • bisphosphonates • neuropathic pain medications • antidepressants • topical anesthetics outcomes 75% success rate Operative : resection of bony prominences (exostectomy) and TAL • indications "braceable" foot with equinus deformity and focal bony prominences causing skin breakdown • goal is to achieve plantigrade foot that allows ambulation without skin compromise deformity correction, arthrodesis +/- osteotomies • indications • severe deformity that is not "braceable" • very high complication rate (up to 70%) amputations • indications • failed previous surgery (unstable arthrodesis) • recurrent infection • goal is for a partial or limited amputation if vascularity allows. ◦ partial calcanectomy +/- Achillis tendon lenghtening ▪ indications ▪ large heel ulcers with associated calcaneal osteomyelitis ▪ outcomes ▪ preserves limb length and decreases morbidity compared to higher level amputations ◦ Syme amputation
- 15. ▪ indications ▪ forefoot gangrene and a palpable posterior tibial artery pulse ◦ Keller resection arthroplasty ▪ indications ▪ IPJ plantar neuropathic ulcer with hypomobile/stiff MTPJ that has failed total contact casting Poliomyelitis: Poliomyelitis is caused by a viral infection of the anterior horn cells of the spinal cord, which may lead to permanent paralysis of isolated groups of muscles and death. Postpolio syndrome • an aging phenomenon where more nerve cells become inactive with time it does not represent reactivation of the virus • occurs after middle age occurs in up to 50% of polio cases • patients should exercise at sub-exhaustion levels to tone affected muscle groups without causing muscle breakdown hallmark is motor weakness with normal sensation. Treatment :- Post-polio Syndrome • nonoperative • limited exercise with periods of rest, +/- lightweight orthosis indications first line of treatment to maintain but not overuse muscles • operative • tendon transfers, contracture releases, and arthrodesis • indications used to optimize functional capacity Polio foot deformities • nonoperative lightweight orthoses
- 16. first line of treatment help patient remain functionally independent • operative • contracture release, tendon transfer, and arthrodesis • indication • if orthoses do not achieve satisfactory standard of living Charcot-Marie-Tooth Disease : Description ◦ Charcot-Marie-Tooth Disease, also known as peroneal muscular atrophy, is a hereditary motor sensory neuropathy (HMSN) that results in muscles weakness and sensory changes ▪ muscle weakness leads to cavovarus foot, scoliosis, and other orthopaedic conditions most common inherited progressive peripheral neuropathy • Pathophysiology ◦ Type I ▪ abnormal myelin sheath protein is the basis of this degenerative neuropathy. ▪ results in a combination of motor and sensory disturbances. ◦ Type 2 ▪ intact myelin sheath with wallerian axonal degeneration that results in mild sensory and motor conduction velocities. ◦ pathoanatomy ▪ affected muscles become weak ▪ peroneus brevis ▪ peroneal involvement is typically first and most profound ▪ results in muscle imbalance and varus deformity
- 17. ▪ tibialis anterior ▪ weakness results in dropfoot ▪ intrinsic muscles of hand and foot ▪ wasting of 1st dorsal interosseous autosomal dominant PMP 22 may also be ▪ autosomal recessive ▪ X-linked • Orthopedic manifestations ◦ pes cavovarus ◦ hammer toes ◦ hip dysplasia ◦ scoliosis ◦ hand muscle atrophy and weakness it’s always important to check hands you want to get an AP pelvis x-ray very high risk dysplasia especially the type ones and also to pay attention to their spines as they do have a high rate of scoliosis Coleman block test this is important to assess hindfoot flexibility it is critical if you’re planning a surgical procedure they tend to get a plantar flexed first ray
- 18. trying to assess is whether or not the deformity is forefoot driven coming from the first ray or whether it’s really hindfoot driven coming from the calcaneous and these are that tend to be fixed in Varus with coleman block test many of these patients treated early with a full light semi rigid insole it’s important to depress the first right and to add a lateral wedge Surgery : soft tissue vs bony ! tenden transfers alone which can leads to high failure rate Plantar fascial release is critical for all of these procedures you might consider peroneous longus to brevis transfere as well as transferring PTT to the dorsum of the foot if there is sever tip weakness Jones procedure comes is for clients and involves transferring EHL to 1st MT and lesser extensors to MT neck first metatarsal dorsiflexion osteotomy is incredibly powerful tools at a flexible Varus And fixes calcaneus if there is fixed varus in the heel