
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Clavicular fracture & acj injury
Semelhante a Clavicular fracture & acj injury (20)
Último
Último (20)
Clavicular fracture & acj injury
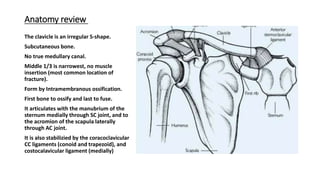
- 1. Anatomy review The clavicle is an irregular S-shape. Subcutaneous bone. No true medullary canal. Middle 1/3 is narrowest, no muscle insertion (most common location of fracture). Form by Intramembranous ossification. First bone to ossify and last to fuse. It articulates with the manubrium of the sternum medially through SC joint, and to the acromion of the scapula laterally through AC joint. It is also stabilizied by the coracoclavicular CC ligaments (conoid and trapezoid), and costocalavicular ligament (medially)
- 4. Mechanism of injury Fall onto the shoulder (87%) direct blow to lateral aspect of shoulder 6% fall on an outstretched arm or direct trauma
- 5. Classification:- Allman with Neer’s modification
- 6. Group I (Middle third) 80% Non-Displaced :- Less than 100% displacement Non-operative displaced :- Greater than 100% displacement Nonunion rate of 4.5% operative
- 7. Group II -Lateral third (10-15%)
- 8. Type 1 minimal displacement (interligamentus) • Stable because conoid and trapezoid ligaments remain intact • Nonoperative
- 9. Type II displaced 2ndry to a fracture line medial to the CC ligament Type II A :- conoid and trapezoid attached (fracture medial to CC ligaments) Medial clavicle unstable Up to 56% nonunion rate with nonoperative management Operative
- 10. Type II B :- conoid torn, trapezoid attached (fracture between the CC ligaments) Medial clavicle unstable Up to 30-45% nonunion rate with nonoperative management Operative
- 11. Type III fracture of the articular surface Conoid and trapezoid intact therefore stable injury Non-operative
- 12. Type IV periosteal sleeve fracture (children) Conoid and trapezoid ligaments remain attached to periosteum and overall the fracture pattern is stable Non-operative
- 13. Type V Comminuted fracture Conoid and trapezoid ligaments remain attached to comminuted fragment Medial clavicle unstable Operative
- 14. Presentation:- Symptoms anterior shoulder pain Physical exam Deformity perform careful neurovascular exam tenting of skin (impending open fracture) Associated injury ipsilateral scapular fracture scapulothoracic dissociation rib fracture pneumothorax neurovascular injury
- 17. deformity forces on clavicular fracture •the sternocleidomastoid muscle pulls the medial fragment posterosuperiorly •pectoralis and weight of arm pull the lateral fragment inferomedially
- 18. Diagnosis plain X-ray:- • standard AP view of bilateral shoulders to measure clavicular shortening • 15° cephalic tilt (ZANCA view) determine superior/inferior displacement CT scan • may help evaluate displacement, shortening, comminution, articular extension, and nonunion • useful for medial physeal fractures and sternoclavicular injuries
- 20. Treatment Non-operative sling immobilization with gentle ROM exercises at 2-4 weeks and strengthening at 6-10 weeks. Operative • Closed Reduction, Intramedullary Fixation • Open Reduction, Plate and Screw Fixation
- 21. Indications: • minimally displaced. • shortening and displacement <2cm • no neurologic deficit Indications: absolute • open fxs • displaced fracture with skin tenting • subclavian artery or vein injury • floating shoulder (clavicle and scapula neck fx) • symptomatic nonunion • symptomatic malunion • unstable fracture patterns (Type IIA, Type IIB, Type V) relative and controversial indications • displaced Group I (middle third) with >2cm shortening • bilateral, displaced clavicle fractures • brachial plexus injury (questionable b/c 66% have spontaneous return) • closed head injury • seizure disorder • polytrauma patient
- 23. Close reduction and intramedullary fixation (titanium elastic nail) Advantage:- 1. Small incision and less soft tissue disruption 2. Less prominent 3. Avoid supraclavicular cutaneous nerve injury Disadvantage:- 1. Hardware migration 2. Biomechanically inferior to plating
- 27. Open Reduction, Plate and Screw Fixation Superior of anteroinferior plating Hook plate
- 31. complications
- 32. Non-operative complication 1-non-union Risk factor:- • Fracture comminution • Fracture displacement • Smoker • Advancing age
- 34. 2-mal-union shortening >3cm, angulation >30 degrees, translation >1cm Complains:- • increased fatigue with overhead activities • thoracic outlet syndrome • dissatisfaction with appearance • difficulty with shoulder straps, backpacks
- 38. 1-infection
- 43. 4-neurovascular injury superior plates associated with increased risk of subclavian artery or vein penetration. 5-pneumothorax. 6-non-union. 7-adhesive capsulitis.
- 44. Acromioclavicular joint injuries (A.C separation)
- 45. Anatomy • AC joint is a synovial joint with a fibrocartilaginous disk. • It has thin capsule that is stabilized by sup. Inf. Ant. and post. Ligaments. • superior and posterior ligaments are most important. • Vertical stability is provided by the CC ligaments:- • Trapezoid insert 3cm from end of clavicle. • Conoid insert 4,5cm from end of clavicle. • Normal AC joint are 5 to 6 mm in width. • Normal CC distance is 1,1 cm to 1,3 cm.
- 47. Mechanism of injury • Fall on shoulder or direct blow to the acromion with arm adducted. (most common) • Fall on outstretched arm transmitted to AC joint. • Rugby and hockey players frequently sustained this injury.
- 49. Type 1 Sprain of the A.C joint only
- 50. Type 2 A.C joint and capsule are disrupted. C.C ligaments are intact. Less than or equal to 50% vertical subluxation of the clavicle. The C.C interval is slightly increase (<25%). reducible.
- 51. Type 3 Rupture of both ACJ and CC ligaments. Complete loss of contact between clavicle and acromion. CC interval is increased from 25-100%. Reducible.
- 52. Type 4 Rupture of ACJ and CC ligaments with displacement of clavicle posteriorly through trapezoid. not reducible.
- 53. Type 5 Rupture of both ACJ and CC ligaments with gross displacement of the ACJ and detachment of deltoid and trapezius. not reducible.
- 54. Type 6 Subcoracoid displacement of the clavicle. Rare. not reducible.
- 55. • Symptoms pain • Physical exam palpate for lateral clavicle or AC joint tenderness. observe for abnormal contour of the shoulder compared to contralateral side. prominence of the distal calvicle
- 57. Imaging • bilateral AP view (compare displacement to contralateral side). • 15 cephalic tilt (zanca view) to evaluate joint displacement and intra- articular fracture. • Axillary view is mandatory to determine AP displacement
- 62. Treatment:- Non-operative:- ice, rest and sling for 3 weeks. regain functional motion by 6 weeks. return to normal activity at 12 weeks. • Indication:- type 1, 2, and type 3 if displacement less than 2cm.
- 63. Operative:- Indication:- • Type 4, 5, 6 • Type 3 in athletes, and those with cosmetic concern. rehabilitation • sling immobilization without abduction for 6 weeks • no shoulder ROM for 6 weeks • generally return to full activity after 6 months
- 64. ORIF with Bosworth CC screw fixation Advantage: Provide rigid fixation. Disadvantage 1. Hardware irritation 2. Hardware failure 3. routine screw removal at 8-12wk is advised to prevent screw breakage
- 65. ORIF with CC suture fixation Advantage:- ORIF with CC suture fixation. Disadvantage:- • suture not as stronger as screw fixation. • suture erosion causing distal third clavicle fracture.
- 66. ORIF with hook plate Advantage:- rigid fixation Disadvantage:- acromial erosion. hook pullout. require second surgery for plate removal.
- 67. CC ligament reconstruction (Modified Weaver-Dunn)
- 69. CC ligament reconstruction with free tendon graft Advantage:- graft reconstruction more closely recreates strength of native CC ligament
- 70. Complications:- 1. Residual pain at AC joint in 30-50% 2. AC arthritis:- more common with surgical management than with nonop. 3. CC screw breakage/pullout