2. Objectives
Anatomy of IJV and Subclavian veins
Basic Technique
Sono guided ?
Complications
Summary
3.
4. The sigmoid venous
sinus passes through
the mastoid portion of
the temporal bone
emerging from the
jugular foramen at the
base of skull as the IJV.
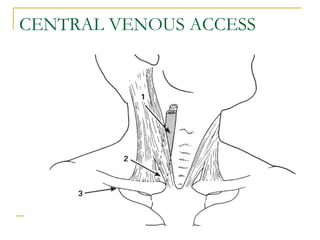
6. The Internal Jugular Vein (High)
Locate the cricoid cartilage and palpate the
carotid artery lateral to it at this level.
Keeping the artery lateral, insert a needle at
an angle of 30 to 40 degrees to the skin
advance the needle towards the ipsilateral
nipple.
The vein is usually within 2-3cm of the skin
7.
8. The subclavian vein is
the continuation of the
axillary vein. It begins
at the border of the first
rib.
9. Relations of subclavian vein
Medially : Posterior border of the
sternocleidomastoid
Laterally: anterior border of trapezius
Caudally : middle third of clavicle
It joins the IJV behind the sternal end of the clavicle
to enter the chest as the brachiocephalic vein.
12. One eye is better than being blind?
B (brightness)mode gives a 2 D image
used in transverse and longitudinal planes
dynamically
Fluid is seen as dark. Air reflects sound(echoes )
Arteries will be seen to pulsate/difficult to compress
Veins are nonpulsatile /collapse or distend
Venous patency, course and relations
Optimal patient position
13.
14.
15.
16. Internal Jugular
Central Lines are inserted into the IJ.
Can either be performed in either longitudinal or transverse views
Longitudinal view Transverse view
18. Randolph et al conducted a meta analysis of
8 RCTs on the comparison of sono guided
and landmark guided central venous access
Higher success rate
Fewer passes
Lower rate of complications
19. National Institute for Clinical
Excellence (NICE)
20 randomized clinical trials
Failed catheter placement risk
was reduced by 86%
Associated complications
reduced by 57%
First attempt success increased
by 41%
20.
21.
22. Difficult central venous access
Surface landmarks difficult
Limited sites for access
History of difficult placement/complication
Vascular anomaly
Coagulation disorder
Patient unable to tolerate supine position
Multiple long term catherisation, dialysis
Agitated / poor compliance
28. Less common complications
Thoracic duct damage
Tracheal damage
Endotracheal tube damage
Respiratory obstruction (by hematoma)
CVA dt puncture of carotid/vertebral
artery
29. Points to remember
Simple test to rule out jugular placement
Which antibiotic ointment should be used
Position of patient for the Xray ?
Type of dressing ?
Length of catheter ?