Alt Story Forms.AMA News
•
1 gostou•1,428 visualizações

AMA News handbook on use of alternative story forms.

Recomendados
Mais conteúdo relacionado
Destaque
Destaque (18)
Semelhante a Alt Story Forms.AMA News
Semelhante a Alt Story Forms.AMA News (20)
Mais de Michael Roberts
Mais de Michael Roberts (20)
Último
Último (20)
Alt Story Forms.AMA News
- 1. Understand first, then be understood How clearly do you understand the story? Does the information make sense? Is it logical and believable? What is the context? For example, is the story about an increase in medical errors? Consider this: Illinois has 1,000 medical errors this year. Rhode Island has 500. Does that mean medical errors are more likely to occur in Illinois? Illinois has 10 million medical procedures performed annually while Rhode Island has 2 million procedures performed annually. Illinois’ error rate is 1,000/10,000,000 (or 1 in 10,000) and Rhode Island’s error rate is 500/2,000,000 (or 1 in 4,000). In fact, the error rate for Rhode Island is higher than that for Illinois. Vet and scrutinize the information Is the information reliable? Do you know the source and/or the motivation the source has for supplying the information? Are there holes in the data? Are there odd trends, such as a big jump in numbers for no apparent reason? It’s vital that our readers trust our scrutiny of the data and believe we have presented it faithfully. We should walk away from graphics that lack the data integrity we require. Ask more sophisticated questions to make better graphics. Going back to the medical error exam- ple, consider this: Is a 100% increase in medical errors the result of one additional medical error, or the result of many errors across the country? Does the increase represent a significant increase in errors, or has the error rate gone from one medical error committed last year to two medical errors committed this year? Can you show where errors are occurring? Is there a geographic pocket where they occur more often? Have a point Think clearly about the purpose of this graphic. Some graphics reconstruct tangible images, such as a medical experiment or building layout. Oth- ers illustrate the intangible, such as a budget or a health plan merger. Ask, what exactly do I want the reader to get from this graphic? You should be able to express the answer in one short sentence: I want viewers to see that Medicare pay has been slashed by 25%. Or, that medical errors are most- ly occurring at hospitals in rural areas. Run through seven important questions: n Can we show meaningful comparisons? n Can we offer guidance or tips? n Can we break it down to provide more context? n Does the trend tell the story? n How can we show what words alone can’t easily explain? Graphic handbook AMERICAN MEDICAL NEWS How to make a quality graphic Secondary items that represent data are an essential part of the paper and should receive the same scrutiny as stories. If it involves the explanation or presentation of any sort of data, here are some tips to help it be the best graphic it can be. n Seven questions to ask yourself when creating a graphic n The proofing process n Math concepts every journalist should know PAGE 1
- 2. n Can we forecast or handicap an issue? n Does the reader need highlights? Talk with others Think about these things, but don’t be alone in the process. It is critical that reporters, editors and art directors sit down and talk about a graphic as it is starting to take shape. Maestro-type discussions should occur. They don’t need to be long. Some may take five minutes or less. The conversation with the art director will help clarify the visual process, and make sure you are presenting the most essential information and balancing the needs of the story with the needs of the secondary elements. Turn in clean copy When you request a graphic, provide all the information necessary for its completion. Too much information is better than not enough. If your story cites a trend, and the accompanying graphic only has information for this year and the last — well, suffice it to say that two numbers do not a trend make. Also consider this: n Spell-check. n Double-check numbers against the original source. n Add numbers to make sure all rows and columns add up as they should. n Treat the graphic the way you would treat a story. Remember: Deadlines, deadlines, deadlines To create a well-thought-out visual presentation, all the information has to be available to the art director in a timely fashion. During the planning process with the topic editor and art director, a deadline will be set based on the complexity of the graphic. But generally, you should plan to file your graphic well before you file the story so the art department has time to work on it and can provide guidance on available space. If the information gets to the art department late, the graphics suffer. How to make a quality graphic Secondary items that represent data are an essential part of the paper and should receive the same scrutiny as stories. If it involves the explanation or presentation of any sort of data, here are some tips to help it be the best graphic it can be. n Seven questions to ask yourself when creating a graphic n The proofing process n Math concepts every journalist should know PAGE 2 Graphic handbook AMERICAN MEDICAL NEWS
- 3. Seven questions to ask yourself when creating a graphic A graphic should answer one of these important questions. The editor also should be asking these questions of the reporter to decide which type of graphic will aid the telling of a specific story. Stories will be measured against this list during maestros and front page discus- sions, so be prepared. n How to make a quality graphic n The proofing process n Math concepts every journalist should know 1. Can we show meaningful comparisons? Comparisons allow quick and easy scrutiny of related bits of information. Pro/con boxes and tables pairing data across specialties or regions are naturals for this treatment. While other types of boxes allow comparisons, paired data is the primary device we use to draw connections for the reader, based on how the cells of the chart are configured. n Would an advantage/disadvantage box be helpful? n Are there two views on an issue, such as pro/con? n Do the data compare clinical measures? n Can we compare geographically? n Can we compare by specialty? n Can company-to-company or product- to-product comparisons be made? 2. Can we offer guidance or tips? Specificity directly impacts usefulness. When ex- pert guidance is vague, the reader isn’t left with much to act on. These boxes work best as the marching orders with a story of anecdotes and ex- pert commentary. Essential for successful “how- to” features. n Is there a “how to”? n Does another organization have policies our readers can learn from or implement? n Are there guidelines to follow? n Is there list of considerations that would help physicians make a decision? 3. Can we break it down to provide more context? When it’s important to offer greater context than the story’s narrative structure will allow, data- driven treatment can be helpful. The story may focus on the five states leading the charge on a particular issue, while an accompanying map shows what the other 45 are doing. This device is what we use when it’s worth our readers time to know how every slice of the pie measures up. As a national publication with a multispecialty readership, this is a key element for our storytelling. n Can the story address the human side while the graphics address the numbers? n Can you go beyond the summary numbers in a study? n Do national data provide needed context for the story? n Is there something you’ll touch on broadly that can be detailed in a graphic? n What is more important — the percentage of people who fall into a category or the raw number? 4. Does the trend tell the story? A trend chart is intended to speak primarily to changes that happen over time. In some of the more complex trend charts, there may be comparisons among specialties or regions within the plotting, but this more elaborate handling should still underscore a relevant behavior over time. Be aware, though, that in many instances, PAGE 3 Graphic handbook AMERICAN MEDICAL NEWS
- 4. specific details of the data will be lost in the plotting. For example: A bar measuring 6.3% will look very similar to a bar measuring 6.6%. If that level of precision must be maintained, we often handle the data as a table. The trend is a little harder to detect, but we maintain the nuance that some data sets require. n Can we show the progress of one variable over a long time? n Is the trend as important as the comparison between variables, such as states, specialties or demographics? n Can we show how the gains of one variable impact the losses of another? n Can we add explanations to provide context for trends? 5. Can we show what words alone can’t easily explain? A formula or process presented visually can provide a clearer understanding than a narrative explanation. Flow charts or architectural/ environmental image packages fall into this category. It is difficult to estimate a final size for this graphic element, so good advance planning is essential, both to set a realistic story length and to clarify what should be handled in text and what is addressed graphically. n Are there floor plans, diagrams or before/after visuals that bring an essential aspect to the story? n Is there a mathematical or scientific formula we can show physicians in its pure form? n Is there an example to show, perhaps with commentary? For example, instead of describing the components of a tax form, can you show a sample of a finalized form? 6. Can we forecast or handicap an issue? This is a difficult treatment to pull off, but if our research or access to expertise can lead to a secondary element that quickly handicaps an issue or the players involved, it can be a potent offering. As with tips boxes, specificity is important. The story can handle nuances at greater length while the box gives the scorecard. n Are there projections of things to watch that indicate what could happen on an issue in the future? n Is there a “to-watch” list of people? 7. Does the reader need the highlights? These often come in the form of a bullet box citing significant facts from a report or news event. Be mindful of how much the content overlaps with the story and limit the bulleted points to the most essential or compelling. n Can a policy/bill/case be summarized? n Can a complicated issue be broken down and laid out in a way that makes it easy for the reader to understand? n Is there a bio box on the person we are focusing on in the story? Seven questions to ask yourself when creating a graphic When any graphic is presented, it should answer one of these important questions. If a story lacks a graphic and its omission is not due to space, the editor should be asking these questions of the reporter to decide which type of graphic will aid the storytelling. For maestros and front page discussions, stories will be measured against this list, so be prepared. n How to make a quality graphic n The proofing process n Math concepts every journalist should know PAGE 4 Graphic handbook AMERICAN MEDICAL NEWS
- 5. Reporting that more businesses are showing interest in preventive medicine programs, this feature targets physicians who might take advantage of the trend by sharing the experiences of those who are doing it now. To accompany another useful graphic, which outlines how to make a wellness program work, this paired data graphic is an important jump-page device to entice skimming readers into the story. By delivering simple comparisons in a familiar advantage/disadvan- tage format, the graphic acts as a box score. Interested readers will turn to the story for more information while those who have read the story will have a handy reminder of the business models discussed. PAGE 5 FOCUS ON PREVENTIVE MEDICINE Wellness programs come in many shapes and sizes, presenting a wide array of business opportunities for physicians. Here are descriptions of a few models: Contracted services An individual physician offers services to a hospital that has created a wellness clinic. You can tailor your own offerings and develop your practice accord- ing to how many wellness patients you want to see. The partnering company handles marketing, billing and other services geared to get the wellness business off the ground. You can maintain your own prac- tice while working with wellness patients for a few hours each week. You also don’t have to worry about marketing the business. You have to do your own sales and marketing. Your schedule is subject to how busy the wellness clinic becomes, and you don’t have as much control as you would if you ran the clinic yourself. You have less control over clinic operations and have to pay a management fee. You may not have the space necessary to accommodate a partnership clinic, or you might have to renovate your current space. Partnership with a management company Developing business- es offers turnkey services to physicians and hospitals for a management fee. ADVANTAGESMODEL DISADVANTAGES Wellness practice A physician group offers wellness services to local businesses. 1 Can we show meaningful comparisons? F or an afternoon every week or two, internist Richard Hilde- brand, MD, practices medicine in a way that would make most physi- cians jealous. As medical director at the Center for Preventive Medicine, part of St. Luke’s Health System in Sioux City, Iowa, Dr. Hildebrand spends two or three hours with the same patient. He focuses not on acute illnesses, but on wellness. He puts the patient through a series of tests, and actually has time to go over results with him or her once they’re completed. “Over time — and I hate to speak for everybody — we’ve gotten used to the appointments every 10 or 20 min- utes,” Dr. Hildebrand said. “This is a nice combination of very old-fash- ioned, but very high-tech. It makes a lot of sense.” Employers think so, too. More com- panies are joining in the wellness trend, sponsoring pre- ventive health pro- grams and asking — or, in some cases, requir- ing — their employees to enroll. Programs range from one-dimen- sional, single-issue pro- grams such as smoking cessation to di- verse, multipurpose strategies that look at a person’s overall health. Sensing a business opportunity, some physicians are starting to adapt their practices to fit this trend as well. Some are providing contracted ser- vices to hospitals, while others are tai- loring wellness programs and market- ing them directly to local businesses. A few doctors even are partnering with fledgling businesses providing turnkey-style support or other ser- vices to help them get their wellness practices off the ground. Regardless of the size of the busi- ness or practice, they have a straight- forward sales pitch to employers: wellness programs will save busi- nesses money. “It saves on insurance costs, and we’ve seen amazing successes in sav- ing people’s jobs from things like ad- dictions, surgeries and life stresses,” said Lee Rice, DO, a family physician and sports medicine specialist in San Diego. Dr. Rice is also CEO and med- ical director of Lifewellness Institute, a preventive medicine practice. “Busi- nesses see employees as their most im- portant asset, and they want their em- ployees to know it,” Dr. Rice said. Employers see corporate wellness programs as a way to both control health care costs and boost key em- ployees’ productivity. The theory is a AMERICAN MEDICAL NEWS AMEDNEWS.COM JUNE 5, 2006 17 BusinessPRACTICE MANAGEMENT n PERSONAL FINANCE n TECHNOLOGY Physicians score victory in class-action compliance settlement [ PAGE 19 ] Businesses are showing more interest in preventive medicine programs, providing a new business opportunity for physicians. Wellnessgoes to work MAKING WELLNESS WORK A 2005 Hewitt Associates survey says employers are developing more of an interest in corporate wellness programs. Here are some reasons why: n Insurance expenses are rising. n Healthy employees are more productive and miss less work time. n It’s a cost-effective way to prove to employees that the company cares for their well-being. Here are some condi- tions that can make wellness programs a good business opportuni- ty for physicians: POPULATION More densely populated areas could provide a large enough pool of people interested in wellness. NUMBER OF BUSINESSES The more corporate clients you can sign up, the greater percentage of your practice you dedicate to wellness. TYPES OF BUSINESSES Large manufacturing facilities might not find all-inclusive programs to be cost-effective, but they could contract for single services, such as nutri- tional counseling or tobacco cessation. Small, self-insured, white-collar businesses, meanwhile, may be interested in comprehensive care. CONTACT WITH DECISION MAKERS If you belong to a local club or know local busi- ness CEOs through work or business circles, you might have a better chance of marketing your wellness services and landing corporate clients. Continued on next page Richard Hildebrand, MD Story by Mike Norbut Photo by Greg Latza
- 6. n Allows physicians to spot areas that need improvement and lets them use the knowledge to make changes. n Lets payers reward physicians who perform better with more referrals and bonus pay. n Empowers consumers to choose physicians on the basis of both quality and cost, particularly with the number of patients using health savings accounts at 3.2 million and growing. Increased competition for patients will lead to overall quality improvement. n Quality measurement can be inaccurate if it is based on admin- istrative claims data that do not capture the entirety of a patient’s circumstances. n Compliance can be costly. Either a practice must do timely, expensive chart reviews or spend heavily on electronic medical record systems. n Quality measures can unfairly represent physicians’ performance. For example, outcome-based measures can penalize physicians who see patients who are sicker or face economic, cultural and linguistic barriers to complying with doctors’ orders. n When paired with pay-for-performance, quality measurement could merely reward larger practices that have made costly technology investments and practices in higher-income areas. Perversely, quality measurement could divert resources away from already underserved areas. PAGE 6 ASSESSING QUALITY The era of measuring physician performance is likely here to stay. Drawn from a range of perspectives, experts say these are some of the pros and cons of quality measurement. PROS CONS The headline sums up this story well: Quality quandary. Performance measures have doctors up in arms. Some physicians can see benefits if it is done right. Other physicians say the entire idea is flawed. The story focuses on the issue of physicians being worried that quality measures could leave behind the sickest and most vulnerable patients because doctors don’t want to be dinged on quality measures for patients they know won’t improve. The pro/con box that accompanies the story takes a bigger look at the pay-for- performance issue and sums up doctors’ likes and dislikes about being assessed for quality. It sums up concerns in many areas, not just the issue of patient care. 1 Can we show meaningful comparisons? MAY 22/29, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS 12 Professional Issues FSMB data show modest dip in disciplinary actions [ PAGE 15 ] HEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION C an a number tell the world how good a doctor is? A lot of people are counting on it. The government, health plans and employers are demanding a way to quantify the value they’re getting for their health care dollars. Patients, faced with higher co-pays and deductibles and increasingly invested in health savings accounts, want reliable public ratings of doctors’ performance. Only a third of physicians have access to any data about their own clinical performance, and just a quarter have the electronic medical records systems considered essen- tial for continuous quality improvement, according to a 2003 Commonwealth Fund survey of doctors. Still, a small but growing number of physicians who have assessed the quality of care they deliver as part of maintenance-of-certi- fication and pay-for-performance programs see quality measurement as helpful to care better for their patients. But many physicians, embittered by early and clumsy attempts by outsiders to gauge their performance, have deep concerns about the accuracy and fairness of quality measurement. With more than 100 pay-for-performance programs up and running, according to the Leapfrog Group, and the Centers for Medicare & Medicaid Services asking physicians to voluntarily report quality data, it seems quality measurement is here to stay. Yet as physician groups take over the reins in develop- ing quality measures for payers and the public to use, a quandary presents itself: Could attempts to improve quality by measuring it have the perverse effect of punishing doc- tors who care for the most vulnerable patient populations? Skeptical doctors say the medical experts, academicians, methodologists and statisticians charged with developing quality measures must be mindful of their potential impact on practicing physicians and the patients they serve. Concerns about patient outcomes R andall Maxey, MD, PhD, approves of the quality mea- surement idea in general but worries about whether its use could wind up penalizing physicians who prac- tice in underserved areas. While most measures gauge how often physicians deliver clinically recommended care, a few very important ones hold doctors accountable for their patients’ outcomes. “It’s going to be a lot easier to treat a little old lady from Beverly Hills,” said Dr. Maxey, an Inglewood, Calif., nephrologist who co-chairs the Commission to End Health Care Disparities and a National Medical Assn. former president. “Some communities are more compliant and more health-literate and have more resources to influence outcomes than others. I may treat you exactly correctly and give you the right pills, but if you have to choose be- tween buying pills and giving your baby milk, that drug may lose out and my performance may be judged as poor because of it.” Roy M. Poses, MD, shares Dr. Maxey’s concern. Qquandary Quality PHOTO©JOHNFORASTÉ ASSESSING QUALITY The era of measuring physi- cian performance is likely here to stay. Drawn from a range of perspectives, experts say these are some of the pros and cons of quality measurement. PROS n Allows physicians to spot areas that need improvement and lets them use the knowledge to make changes. n Lets payers reward physicians who perform better with more referrals and bonus pay. n Empowers consumers to choose physicians on the basis of both quality and cost, particularly with the number of patients using health savings accounts at 3.2 million and growing. Increased competition for patients will lead to overall quality improvement. n Quality measurement can be inaccurate if it is based on administrative claims data that do not capture the entirety of a patient’s circumstances. n Compliance can be costly. Either a practice must do timely, expensive chart reviews or spend heavily on electronic medical record systems. n Quality measures can unfairly represent physicians’ performance. For example, outcome-based measures can penalize physicians who see patients who are sicker or face economic, cultural and linguistic barriers to complying with doctors’ orders. n When paired with pay- for-performance, quality measurement could merely reward larger practices that have made costly technology investments and practices in higher-income areas. Perversely, quality measure- ment could divert resources away from already under- served areas. CONS As the movement to measure quality forges ahead, some physicians worry their patients could be left behind. Story by Kevin B. O’Reilly Outcome-based measurements need to control for patient characteristics, said internist Roy M. Poses, MD.
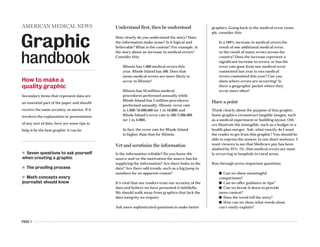
- 7. PAGE 7 To bring greater clarity to a story about the link between quality and volume in nonsurgical care, this graphic presented valuable data for comparison. It is based on a study of pneumonia patients, and in a simple manner, lays out key findings for four levels of patient volume. A few key findings are explained to set up the top of the story, but it’s the graphic that carries the essential details. 1 Can we show meaningful comparisons? n Doctors say the decision opens the door for “junk science.” AMY LYNN SORREL AMNEWS STAFF If a New York appeals court ruling that loosened rules for expert witness testimony allowed in medical liability cases stands, physicians say it will open the gate for unreliable scientific evidence to enter the courtroom. In a unanimous opinion, the Appel- late Division of the Supreme Court, the state’s intermediate level, said ex- perts did not need to show peer-re- viewed medical literature to prove that their medical opinion was accept- ed in the scientific community. Judges found that a lower court ap- plied the testimony rule “too restric- tively” when it wouldn’t allow the tes- timony and dismissed the case. Physicians say the appeals court ruling defies state precedent uphold- ing rigorous scrutiny of what testimo- ny is permitted to be heard by jurors. If the courts don’t adhere to the stan- dard, physicians say, ripple effects could cause meritless lawsuits to en- ter the legal system. Lawyers for the physician in the case are asking the appeals court to reconsider. If that doesn’t happen, they will ask the state’s high court to overturn the ruling. The medical com- munity has weighed in on the physi- cian’s side, with doctors and a phar- maceutical company fearing that the ruling would be used as an example for other courts to relax the rule if it’s not reversed. “There should be a high standard, and it’s up to the courts to make sure that any medical theory being [pre- sented] actually has the support of the profession,” said Donald Moy, general counsel to the Medical Society of the State of New York, which filed a friend-of-the-court brief with the American Medical Association and Pfizer. The company didn’t manufac- ture the drug in the lawsuit but does not want to see a precedent set. Allowing only peer-reviewed liter- ature is critical, Moy explained, be- cause it is often difficult for a jury to differentiate between credible science and “junk science.” Mary Beth Ott, who represents the plaintiff, said the appeals court ruling is correct, “and that’s the law as it stands now.” Ott declined to comment further, citing the pending litigation. Did a drug trigger a disease? The case, Zito v. Zabarsky, stems from a November 2003 trial court hearing to screen expert witness testimony. New York courts require the testimo- ny with the plaintiff’s filing of a med- ical liability case to determine the va- lidity of claims made. Judges follow the Frye standard, derived from a 1923 federal ruling that established that novel scientific evidence presented in court must “have gained general ac- ceptance” in the relevant scientific community. Pamela Zito sued Queens internist Gary Zabarsky, MD, alleging that he had prescribed her an “excessive” dose of the cholesterol drug, Zocor (simvastatin), which caused her to de- velop an autoimmune disease, court records show. Dr. Zabarsky denies the n For diseases such as pneumonia, higher patient volume could mean worse physician performance. KEVIN B. O’REILLY AMNEWS STAFF Practice makes perfect? Not always. That’s the find- ing of a recent study that sought to find out whether physicians who cared for a higher volume of pneu- monia patients in a given year were more likely to follow quality guidelines and achieve superior outcomes. Hundreds of studies have used patient volume as a proxy in quality measurement for high-risk surgi- cal procedures, such as coronary bypass artery graft or care for complex diseases such as HIV/AIDS. Nearly 70% of studies examining physi- cian performance in those areas found a statistical- ly significant association between higher patient volume and superior outcomes, according to a 2002 medical literature review published in the Annals of Internal Medicine. But the much-touted volume-outcome correla- tion appears to fall apart for care such as pneumo- nia, according to a study published in the Feb. 21 Annals of Internal Medicine. The evaluation of 9,741 doctors who cared for AMERICAN MEDICAL NEWS AMEDNEWS.COM MAY 1, 2006 11 Professional IssuesHEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION ETHICS FORUM: Apply standards of care equitably [ PAGE 16 ] Volume-quality correlation not clear cut, study says Continued on page 14 Court lowers bar on scientific evidence CASE AT A GLANCE Pamela Zito v. Gary Zabarsky, MD Venue: New York Supreme Court, Appellate Division, Second Department At issue: Whether medical expert testimony required in medical liability cases must include peer-reviewed literature to show that an opinion is generally accepted by the scientific community. The appeals court said no. Potential impact: Physicians say the ruling goes against precedent, exposing doctors to more lawsuits. The court said a high standard deprives injured plaintiffs of their day in court. Continued on next page New York appeals court ruling “It’s up to the courts to make sure any medical theory ... has support of the profession.” Donald Moy, MSSNY general counsel DISCOUNTING VOLUME Hundreds of studies have found that for complicated surgeries and medical care such as coronary artery bypass grafting or HIV/AIDS care, the higher the volume of cases a physician or hospital sees, the better the outcomes. But for care such as pneumonia, the relationship between the volume of cas- es and physician performance isn’t so clear, according to a recent study of 9,741 doctors who cared for 13,480 patients admitted to hospitals for pneumonia. The study’s authors broke physicians into four groups based on the volume of pneumonia patients they cared for over a year. Here are some of the results: Study groups: 1 2 3 4 Median annual pneumonia cases 4 9 15 29 per physician Percentage of time task performed First antibiotic administered less 59% 63% 62% 62% than four hours after admission Appropriate antibiotics 82% 81% 81% 79% Blood cultures obtained before 84% 84% 84% 83% administration of antibiotics Screened for or given influenza vaccine 21% 19% 20% 12% Screened for or given pneumococcal vaccine 16% 13% 13% 9% Results Mean length of stay (in days) 6.0 6.0 6.2 6.6 Percentage of patients who died 5.8% 6.0% 5.7% 6.6% in the hospital Percentage of patients who died 10.9% 11.8% 11.0% 12.5% within 30 days SOURCE: “VOLUME, QUALITY OF CARE, AND OUTCOME IN PNEUMONIA,” ANNALS OF INTERNAL MEDICINE, FEB. 21 VOLUME OF CASES QUALITY INDICATOR OUTCOMES DISCOUNTING VOLUME Hundreds of studies have found that for complicated surgeries and medical care such as coronary artery bypass grafting or HIV/AIDS care, the higher the volume of cases a physician or hospital sees, the better the outcomes. But for care such as pneumonia, the relationship between the volume of cases and physician performance isn’t so clear, according to a recent study of 9,741 doctors who cared for 13,480 patients admitted to hospitals for pneumonia. The study’s authors broke physicians into four groups based on the volume of pneumonia patients they cared for over a year. Here are some of the results: Study groups: 1 2 3 4 Median annual pneumonia cases 4 9 15 29 per physician Percentage of time task performed First antibiotic administered less 59% 63% 62% 62% than four hours after admission Appropriate antibiotics 82% 81% 81% 79% Blood cultures obtained before 84% 84% 84% 83% administration of antibiotics Screened for or given influenza vaccine 21% 19% 20% 12% Screened for or given pneumococcal vaccine 16% 13% 13% 9% Results Mean length of stay (in days) 6.0 6.0 6.2 6.6 Percentage of patients who died 5.8% 6.0% 5.7% 6.6% in the hospital Percentage of patients who died 10.9% 11.8% 11.0% 12.5% within 30 days SOURCE: “VOLUME, QUALITY OF CARE, AND OUTCOME IN PNEUMONIA,” ANNALS OF INTERNAL MEDICINE, FEB. 21 VOLUME OF CASES QUALITY INDICATOR OUTCOMES
- 8. PAGE 8 Heart disease kills more women than any other disease. This story focuses on the fact that other diseases are better screened and looks at which women are at the highest risk for heart disease. The graphic shows the five leading causes of death for women and gives context for the story. Easy comparison is drawn from the plotting to emphasize just how many more women die from cardiovascular-related issues than from the second leading cause, cancer. By including factoids on cardiovascular disease, the graphic teases out more statistics about how women are impacted. 1 Can we show meaningful comparisons? SOURCE: CENTERS FOR DISEASE CONTROL AND PREVENTION AND THE NATIONAL HEART, LUNG AND BLOOD INSTITUTE n Cardiovascular disease (CVD) ranks first among all disease categories in hospital dis- charges for women. n Of the approximately 5.5 million stroke survivors alive today, 56% are women. n Misperceptions still exist that CVD is not a real problem for women. n CVD is a particularly important problem among mi- nority women; the death rate due to CVD is higher in black women than in white women. n 38% of women compared with 25% of men will die within one year after a heart attack. SOURCE: AMERICAN HEART ASSN. Cardiovascular death: 484,000 Alzheimer’s disease: 45,000 Diabetes mellitus: 39,000 LEADING CAUSES OF DEATH FOR WOMEN in the United States, 2003 Cancer: 268,000 . . . . . Chronic lower respiratory diseases: 66,000 28 Health&Science Risk of second melanoma is higher than previously thought [ PAGE 33 ] C ardiovascular disease kills nearly twice as many women each year as does cancer, yet annual mammograms and Pap smears continue to be an easier sell than lipid profiles or regular blood pressure tests. Despite years of warnings that women face an even greater risk for cardiovascu- lar disease than men, the word has been slow to filter out. Women and their physi- cians still don’t always acknowledge this threat, nor do they take steps to slow its onset, according to many experts. “It is really impor- tant to keep educating patients and physicians about this being such a devastating illness for women,” said Norma Keller, MD, chief of cardiolo- gy at Bellevue Hospital in New York City. Figures from the Centers for Disease Control and Prevention illuminate the problem. In 2003, 484,000 women died from cardiovascular disease compared with 427,000 men. Cancer, the next highest killer disease for women, claimed 268,000 lives that same year. The challenge for primary care physicians is to pick out women most likely to benefit from treatment, said Lori Mosca, MD, MPH, PhD, director of preventive cardiology at New York-Presbyterian Hospital in New York City and chair of the panel that drafted the American Heart Assn.’s Evidence-based Guidelines for Cardiovascular Disease Prevention in Women. “It is clear we are undertreating very high-risk women and that there are many low-risk women who would be better served by lifestyle changes than drug therapy.” So how to determine which group is which? Go back to the basics, she advises. Evaluating traditional risk factors remains key for prima- ry care physicians, Dr. Mosca said. “We have many physi- cians who have not discussed with their patients their risk factors for heart disease, including lifestyle and family histo- ry.” Instead of preventive care, too many physicians are rely- ing on technology that has not been proven to be associated with beneficial outcomes, she added. Jim King, MD, a family physician in rural Selmer, Tenn., keeps pushing this message to his female patients: “Watch your cholesterol, blood pressure and weight, and don’t smoke.” He notes that risk factors are the same for men and women, although women’s risk starts to increase about 10 years later than men’s. His female patients also are still more afraid of breast cancer. “They have to un- derstand that heart disease is a more important threat.” The highest risk African-American women are at the top of the risk scale for heart disease, but they are the group least likely to be diagnosed and treated effectively, said Patricia Davidson, MD, a cardiologist at Washington Hospital Center in Washington, D.C. “African-Ameri- can along with Mexican-American and Native American women have more risk factors lumped together.” Weight is a problem. Sixty-eight percent of African-American women, 71% of Mexican-American women and 60% of Native Ameri- can women are overweight, she noted. “With weight gain comes insulin resistance, which leads to diabetes, which raises your blood pressure.” The lack of aggressive treatment to goal is another pitfall, Getting to the matter the heartof STORY BY SUSAN LANDERS JUNE 5, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS SOURCE: CENTERS FOR DISEASE CONTROL AND PREVENTION AND THE NATIONAL HEART, LUNG AND BLOOD INSTITUTE PUBLIC HEALTH n CLINICAL ISSUES n PATIENTS n Cardiovascular disease (CVD) ranks first among all disease categories in hospital dis- charges for women. n Of the approximately 5.5 million stroke survivors alive today, 56% are women. n Misperceptions still exist that CVD is not a real problem for women. n CVD is a particularly important problem among minority women; the death rate due to CVD is higher in black women than in white women. n 38% of women compared with 25% of men will die within one year after a heart attack. SOURCE: AMERICAN HEART ASSN. Cardiovascular death: 484,000 Alzheimer’s disease: 45,000 Diabetes mellitus: 39,000 LEADING CAUSES OF DEATH FOR WOMEN in the United States, 2003 Cancer: 268,000 . . . . . Chronic lower respiratory diseases: 66,000 PHOTO ILLUSTRATION BY PETE MCARTHUR PHOTOGRAPHY
- 9. PAGE 9 1 Can we show meaningful comparisons? MEDICATION Methylphenidate, amphetamine, dextroamphetamine Modafinil Growth hormone Testosterone Nicotinic alpha-7 THERAPEUTIC INDICATION Narcolepsy, childhood ADHD Narcolepsy, sleep apnea, shift-work sleep disorder Dwarfism, idiopathic short stature, AIDS- and cancer-related wasting Hypogonadism, andropause Alzheimer’s, schizophrenia ENHANCEMENT USE Intensify mental focus, alertness Combat jet lag, increase wakefulness Delay aging with increased muscle, thicker skin, denser bones, less total body fat Delay aging with increased muscle, denser bones, better mood, higher libido, enhanced cognition Improve memory, psychomotor skills ETHICAL/SOCIAL CONCERNS Social pressures could lead to people using it to be competitive Could lead to compulsory workplace doping to increase effectiveness, safety Could redefine aging as a disease; stigmatize those with short stature Could redefine aging as a disease; pose threat to personal identity Could present a greater danger than enhancement use of stimulants SCOPE OF USE Up to 25% of students at competitive Northeastern universities reported nontherapeutic use of stimulants 90% of prescriptions are for off-label uses About 30% of prescriptions are for off-label uses 500% increase in total testos- terone prescription sales have been seen since 1993 At least 25% of people 85 and older experience dementia; the oldest of the country’s 75 million baby boomers just turned 60 SOURCES: “DRUGS FOR ENHANCING COGNITION AND THEIR ETHICAL IMPLICATIONS: A HOT NEW CUP OF TEA,” EXPERT REVIEW OF NEUROTHERAPEUTICS, MARCH; “PROVISION OR DISTRIBUTION OF GROWTH HORMONE FOR ‘ANTIAGING,’” JOURNAL OF THE AMERICAN MEDICAL ASSOCIATION, OCT. 26, 2005; “RISKS OF TESTOSTERONE-REPLACEMENT THERAPY AND RECOMMENDATIONS FOR MONITORING,” NEW ENGLAND JOURNAL OF MEDICINE, JAN. 29, 2004; “SELECTIVE ALPHA7 NICOTINIC ACETYLCHOLINE RECEPTOR LIGANDS,” CURRENT MEDICINAL CHEMISTRY, VOL. 13, NO. 13, 2006. TREATMENTS TURNED ENHANCEMENTS GRAPHIC REPORTED BY KEVIN B. O’REILLY The story discusses the quandaries emerging as some new treatments intended to heal the sick are also being prescribed to enhance those who are healthy. The table and story work together, with the text handling what experts are saying and the table highlighting the types of drugs being discussed. The heavily-researched table adds a valuable dimension by presenting factors at a level of detail that would have bogged down the story. The final two columns (ethical/social concerns and scope of use) add meaningful content not available in the story and describes the magnitude of the issue. The success of the graphic ultimately rests in its ability to thoroughly present the essential details for a relevant list of drugs. AMERICAN MEDICAL NEWS AMEDNEWS.COM AUGUST 28, 2006 11 Professional Issues North Carolina considers limits on physician role in executions [ PAGE 13 ] HEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION TO HEAL, OR TO ENHANCE? L ecturing a group of students last fall, Martha J. Farah, PhD, commented that there was proba- bly someone in the audience making use of modafinil, approved to treat narcolepsy but mostly prescribed off-label to long-haul truckers, jet- lagged ocean hoppers and anyone else too busy to sleep. “You were right about that!” said a graduate student who approached Dr. Farah, director of the University of Pennsylvania’s Center for Cognitive Neuroscience, after the talk. Once a week, said the student, who is also a teaching assistant, he would find himself falling behind on answering e-mail and grading work. With modafinil, he could stay up all night and still work through the next day. Dr. Farah’s observation was far from a shot in the dark. Increasingly, students at highly competitive universities such as Penn are us- ing modafinil, or stimulants intended to treat attention- deficit/hyperactivity disorder, to enhance their already considerable abilities. Some students are asking doc- tors for these so-called smart pills, though most obtain them illegally from campus dealers. College kids aren’t alone in looking to doctors to do more than just cure their ills. Middle-aged men ask physi- cians for testosterone boosters. Some adults even seek growth hormones, one of the engines that allegedly helped Barry Bonds overtake Babe Ruth on baseball’s all- time home run list. But should doctors say yes when patients ask for en- hancement instead of healing? It’s a question that medicine has grappled with on a smaller scale for years. Cosmetic surgery posed similar questions decades ago and continues to outpace med- ically necessary reconstructive surgeries. Peter Kramer’s 1993 book, Listening to Prozac, alerted the nation to patients who sought to feel “better than well.” And it didn’t take long after Viagra’s 1998 approval be- fore some normally functioning men be- gan using the drug to enhance their sexu- al experiences. The question of whether to abide pa- tient requests for enhancement treat- ments will only continue to intensify as new drugs hit the market. For example, Alzheimer’s medication that is in the pipeline could potentially en- hance healthy individuals’ memory. In fact, the potential for genetic enhancement is so great that the National Institutes of Health is funding an investigation of the ethical implications of the re- search. The AMA’s Council on Ethical and Judicial Af- fairs also is studying human enhancement and may is- sue ethical guidelines for physicians. MAKING THE CALL Doctors can be faced with tough choices when patients ask for something to boost their abilities. Franklin G. Miller, PhD, a bioethicist at the National Institutes of Health, and Howard Brody, MD, PhD, a family physician and Michigan State University bioethicist, offer two principles to consider: 1. The more clearly an intervention also serves a legitimate medical goal — such as preventing disease, promoting health, relieving pain and suffer- ing, or avoiding premature death — the more easily it can be justified. 2. The greater the risks involved, the more difficult it is to justify an enhancement intervention in the absence of a clear health rationale. SOURCE: “ENHANCEMENT TECHNOLOGIES AND PROFESSIONAL INTEGRITY,” MAY-JUNE 2005 AMERICAN JOURNAL OF BIOETHICS New treatments intended to heal the sick also may help the healthy flourish. Where should doctors draw the line? STORY BY KEVIN B. O'REILLY ILLUSTRATION BY TED GRUDZINSKI Continued on next page
- 10. PAGE 10 This story explores a study that concluded doctors like the idea of patient-centered care, but haven’t adopted it. The story touches on highlights from the study, while the graphic allows readers to do comparisons on a couple of levels. First, the graphic shows how three different groupings of physicians ----- primary care, specialists and all physicians ----- have adopted aspects of patient- centered care. It also allows the reader to quickly compare numbers of how many have adopted aspects vs. how many say they plan to. 1 Can we show meaningful comparisons? n A study reaching that conclusion comes as some physician organizations are trying to help practices redesign how they provide care. DAMON ADAMS AMNEWS STAFF Physicians are pretty good at providing same-day appointments for patients who want them. And they usually receive timely test results of patients they referred to another doctor. They don’t do as well at routinely using electron- ic medical records or communicating with patients via e-mail. Those conclusions are based on what 1,837 physi- cians, in practice at least three years, told re- searchers. The nationwide survey led the authors of a new study in the April 10 Archives of Internal Med- icine to find that physicians favor such patient-cen- tered care practices, but few practice all of them. Physicians were asked about 11 patient-centered practices, such as same-day appointments, e-mail with patients, reminder notices for preventive or follow-up care, electronic medical records and patient survey feedback. The study said that about one in four doctors us- es electronic medical records and about half send reminder notices to patients about preventive or fol- low-up care. Three in four primary care physicians had prob- lems with the availability of patients records, test results or other information at the time of a sched- uled visit. But researchers found that doctors favor many elements of patient-centered care. The study said 87% of primary care physicians support improved teamwork among health care professionals while 85% of all surveyed physicians favor easy access to patients of medical records. “They have the right attitude. They thought a team approach to care was a good thing, and they’re planning to look into electronic medical records,” said lead study author Anne-Marie Audet, MD, vice president for quality improvement at the Common- wealth Fund, a private foundation in New York City. New models of care The findings come at a time when some physician organizations are making patient-centered care a key component of efforts to redesign how physi- AMERICAN MEDICAL NEWS AMEDNEWS.COM MAY 15, 2006 9 Professional IssuesHEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION Some New York doctors join the Teamsters [ PAGE 14 ] PUTTING IT INTO PRACTICE A new study in the Archives of Internal Medicine found that a majority of physicians like patient-centered care, but have adopted some aspects faster than others. Here is a look at some patient-centered areas and the percentage of physicians who adopted the practices: Doctors favor patient-centered care but haven’t adopted it fully “They thought a team approach to care was a good thing, and they’re planning to look into electronic medical records.” Anne-Marie Audet, MD, Commonwealth Fund SOURCE: “ADOPTION OF PATIENT-CENTERED CARE PRACTICES BY PHYSICIANS,” ARCHIVES OF INTERNAL MEDICINE, APRIL 10 ISSUE. Continued on page 13 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% PRACTICE ADOPTION PRACTICE ATTITUDE A B C D E F n Total physicians n Primary care physicians n Specialists Local hospitals could hold key to boost residencies n Increasing the physician work force means training more residents, and a medical school has found how to do so. MYRLE CROASDALE AMNEWS STAFF After more than 20 years as a practicing gastroen- terologist, Richard Greenwald, MD, is helping turn his community hospital into a teaching institution. This year Dr. Greenwald, now vice president of medical affairs at Boca Raton Community Hos- pital, helped develop a module covering gastroen- terology, the liver and nutrition for medical stu- dents from the new University of Miami School of Medicine program at Florida Atlantic University in Boca Raton. The hospital’s partnership with FAU and the University of Miami to teach med- ical students is the first step in a long-range plan to cultivate more physi- cians for southeast Florida. By 2010, some 100 to 125 medical residents are ex- pected to be training there. Boca Raton Community Hospital may be the first hospital in recent years to take advantage of a little- used opportunity to get Medicare funding for new residencies. Because the hospital has never sponsored a residency, it is eligible for Medicare graduate medical education dollars, money that has been capped for existing programs since 1996. Given concerns that a physician shortage may develop by 2020, Boca Raton could become a mod- el for those looking for ways to expand residen- cies and physician numbers, work-force experts say. Right now, opening residencies at hospitals that haven’t previously had them is the only route to get new government funding. Richard Reynolds, MD, senior vice president of medical advancement at Boca Raton Commu- nity Hospital, wouldn’t be surprised if others fol- lowed his hospital’s lead. “As we look ahead, with the growth and aging of the population, we’re go- ing to have a doctor shortage,” he said. “Current schools are going to expand, and other [communi- ty] hospitals will become teaching hospitals.” Many consider such expansion good news. But if more community hospitals do begin training residents, some say the practice raises a broader policy issue of how to best spend graduate med- ical education dollars. “Hospitals are feeling a need to increase resi- dency size, and they aren’t getting the Medicare funding to do it,” said Karen Fisher, senior asso- ciate vice president of health care affairs at the Assn. of American Medical Colleges. “If commu- nity hospitals are interested in taking on GME, that’s great. However, from a public policy per- spective, wouldn’t it make more sense to expand GME through quality existing programs as well 64 77 58 54 48 57 27 23 28 26 26 26 10 19 6 20 23 19 Continued on page 15 Med schools expanding to meet future demand. Page 17 A | Always or often provide a same-day appointment to a patient who requests one B | Send patients computerized or manual reminder notices about regular preventive or follow-up care C | Use electronic patient medical records routinely or occasionally D | Medical record(s), test results, or other relevant clinical information never or rarely not available at the time of patient’s scheduled visit E | Plan to send reminder notices about regular preventive or follow-up care within the next year F | Plan to use electronic patient medical records within the next year PUTTING IT INTO PRACTICE A new study in the Archives of Internal Medicine found that a majority of physicians like patient-centered care, but have adopted some aspects faster than others. Here is a look at some patient-centered areas and the percentage of physicians who adopted the practices: SOURCE: “ADOPTION OF PATIENT-CENTERED CARE PRACTICES BY PHYSICIANS,” ARCHIVES OF INTERNAL MEDICINE, APRIL 10 ISSUE. 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% PRACTICE ADOPTION PRACTICE ATTITUDE A B C D E F n Total physicians n Primary care physicians n Specialists 64 77 58 54 48 57 27 23 28 26 26 26 10 19 6 20 23 19 A | Always or often provide a same-day appointment to a patient who requests one B | Send patients computerized or manual reminder notices about regular preventive or follow-up care C | Use electronic patient medical records routinely or occasionally D | Medical record(s), test results, or other relevant clinical information never or rarely not available at the time of patient’s scheduled visit E | Plan to send reminder notices about regular preventive or follow-up care within the next year F | Plan to use electronic patient medical records within the next year
- 11. PAGE 11 The success of this table is largely due to the specificity we provide with the data and how it complements the main story. Allowing the story to focus primarily on the potential versatility of this type of employee, the graphic addresses another key part of the equation: Salary. The graphic offers great depth by showing average salaries based on years of experience as well as geographic region. 1 Can we show meaningful comparisons? A ccording the U.S. Bureau of Labor Statistics, the fastest-growing health profession in the country — the fastest-growing profession, pe- riod — is medical assistant. Physicians such as Catherine Tabb, MD, are one reason why. Dr. Tabb, a solo family physician in Louisville, Ohio, started practice in 1980 with one medical as- sistant. She now has three full-time and three part-time MAs. They’re used for all tasks — front, as well as back office — not performed by her or the practice’s single nurse practitioner. Dr. Tabb likes the flexibility of staff who can assume either front- or back-office duties to make up for vacations or illness. But having people with clinical knowledge at the front desk, making them more useful to patients, is even better. “They can answer basic questions about taking medications without having to transfer the patient to me,” she says. “They help patients decide if they need to come in.” Like most doctors who make extensive use of MAs for clinical tasks, Dr. Tabb believes she’s in no financial position to hire nurses. But more than that, she says, they’re not necessary, particu- larly when most of the clinical work can be handled by MAs. Charles Reed, MD, a pediatrician with 12-doc- tor St. Christopher Pediatric Associates in Philadelphia, says MAs bring versatility atypical of other types of staff. “We can move them from of- fice to office,” he says. “We can use them for clini- cal tasks, and if we need to fill in, we can put them in the front office, registering patients and an- swering phones.” The combination of versatility and compara- tively low cost is driving the demand for MAs, 60% of whom work in physician offices. Accord- ing to an American Assn. of Medical Assistants survey of 4,057 MAs nationwide, 61.6% of an MA’s time is spent on clinical duties, including obtain- ing patient history and vital signs, assisting with patient exams, scheduling patient appointments and performing injections; 25.8% is spent on ad- ministrative duties; 7.3% is taken up with admin- istrative management; and 5.3% is spent on clini- cal management. If they’re certified, MAs make an average salary of $27,951. First-year MAs aver- age $22,650, according to the AAMA. Those in the field say doctors are just begin- ning to tap the potential of MAs. “Only a minority of physician groups know how to utilize MAs and take full advantage of what they can do,” says Don Balasa, AAMA executive direc- tor and chief counsel. But hiring and integrating MAs into your practice is not necessarily an easy task. The duties a me- dial assistant can per- form and the level of su- pervision a physician must provide can vary depending on your state and its regulations. Generally, states define what MAs may or may not do through scope-of-prac- tice laws — if a task is limited to a doctor, nurse practitioner, physician as- sistant or nurse, it’s off- limits to an MA . Finding a qualified MA isn’t easy because of the high demand. Another dif- ficulty is that few have re- ceived certification — estimates are at around 15% — through the AAMA or the American Med- ical Technologists, giving physicians less evi- dence an MA might be up to the job. Hiring an MA P lenty of colleges and institutions offer two- year programs for aspiring MAs. But doctors vary on whether they require certification, which is generally not required by law. Dr. Tabb will hire only certified MAs. Dr. Reed prefers but does not require a candi- date to be certified. He typically hires only candi- dates who have graduated from an accredited post-secondary training program. In fact, most of his hires are candidates who have completed in- ternships in his office. Nick Fabrizio is a consultant with MGMA Con- sulting Group and serves as practice administra- tor for a 12-doctor clinic that is part of the Dept. of Family Medicine at State University of New York Upstate Medical University, Syracuse. He says the best way to find a good MA is to work with a local educational organization that trains them. His group works with Bryant & Stratton College, a community college in Syracuse. By inviting stu- dents to undertake internships at his group, “we get to know the people intimately before we make AMERICAN MEDICAL NEWS AMEDNEWS.COM APRIL 17, 2006 19 BusinessPRACTICE MANAGEMENT n PERSONAL FINANCE n TECHNOLOGY Web site offers list of “average” costs of care [ PAGE 27 ] Medical assistants A key to practice efficiency MAs can be the most versatile members of your staff — if you know how to use them. Continued on next page Story by Larry Stevens and Illustration by Terry Miura MEDICAL ASSISTANT PAY Here are overall and experience-based annual and hourly pay figures from the American Assn. of Medical Assistants’ salary survey on medical assistant compensation. All figures below pertain to certified medical assistants, a designation granted by the AAMA. The national average for noncertified MAs is $26,775, compared with $27,951 for CMAs. Figures are as of 2004, the most recent survey. New England (Conn., Maine, Mass.,N.H., R.I., Vt.) Annual $28,972 $25,056 $25,809 $29,219 $30,576 Hourly $14.49 $12.31 $13.08 $14.69 $15.22 Middle Atlantic (N.J., N.Y., Pa.) $30,451 $24,042 $28,710 $27,167 $32,341 $14.60 $12.96 $14.00 $13.34 $15.45 East North Central (Ill., Ind., Mich., Ohio, Wis.) $26,835 $22,128 $23,939 $25,070 $28,869 $13.27 $11.14 $11.98 $12.80 $14.15 West North Central (Iowa, Kan., Minn., Mo., $27,335 $23,150 $24,477 $26,900 $28,691 Neb., N.D., S.D.) $13.65 $12.04 $12.49 $13.53 $14.25 South Atlantic (Del., Fla., Ga., Md., N.C., S.C., $27,785 $22,922 $24,779 $26,972 $30,218 Va., W.Va., District of Columbia) $13.24 $11.53 $12.14 $13.05 $14.23 East South Central (Ala., Ky., Miss., Tenn.) $26,726 $22,000 $25,750 $25,974 $27,953 $12.69 $10.88 $11.78 $12.30 $13.29 West South Central (Ark., La., Ok., Texas) $29,115 * $24,600 $26,875 $31,152 $13.26 * $12.27 $12.54 $14.16 Mountain (Ariz., Colo., Idaho, Mont., Nev., $27,380 * $24,800 $25,426 $29,494 N.M., Utah, Wyo.) $13.40 * $12.58 $13.08 $13.98 Pacific (Alaska, Calif., Hawaii, Ore., Wash.) $29,995 $27,472 $27,082 $29,468 $31,534 $14.90 $13.76 $14.28 $14.94 $15.42 *INSUFFICIENT RESPONSE NOTE: REGIONS ARE AS DEFINED BY THE U.S. DEPT. OF CENSUS. SOURCE: AMERICAN ASSN. OF MEDICAL ASSISTANTS REGION OVERALL 1–2 3–5 6–9 10 + YEARS YEARS YEARS YEARS
- 12. PAGE 12 This was an ideal opportunity for a comparative table. The story discusses an international patient survey that showed the U.S. lagging behind five other nations in nearly all areas surveyed. The story described the nature of the survey and provided numerous interesting findings, while the graphic gave side-by-side rankings of the six nations involved. At a glance, the reader can compare rankings for the subcategories that contribute to the overall rank. Any story that relies so heavily on accessible comparisons like these would suffer if it lacked a graphic presentation of the key findings. 1 Can we show meaningful comparisons? n The country was rated first only in effectiveness of care. ELAINE MONAGHAN AMNEWS STAFF Washington Adult patients in the United States are less safe, not as well informed by their doctors and more unequally treated than people in five other developed nations that spend far less treat- ing them, according to two stud- ies released earlier this month by the Commonwealth Fund. America ranked last overall when compared with Australia, Canada, Germany, New Zealand and the United Kingdom in one study, “Mirror, Mirror, on the Wall: An Update on the Quality of American Health Care Through the Patient’s Lens.” This analysis compared U.S. health leaders to the vain queen in “Snow White.” Too often, they excluded experiences of other coun- tries, looking only “at our own reflec- tion in the mirror,” the report states. Based on 2004 and 2005 surveys, it found that American patients were most likely to say they encountered a laboratory test mistake or delay in re- ceiving abnormal results, did not get questions answered by their physi- cian, struggled to get needed care at nights or on weekends, and failed to fill or take prescriptions due to cost. Janet Corrigan, PhD, president and CEO of the National Quality Fo- rum and the National Committee for Quality Health Care, said the study should not be read as an indictment of physicians, but as further evidence of the need to reform the country’s disor- ganized health system. She noted the study’s reliance on patient assess- ments. “You might get different re- sults if you asked physicians or looked at medical records.” The work, which followed an Institute of Medicine framework to evaluate health care system quality, concluded that the Unit- ed States ranked first in six out of 51 indicators, and last or tied for last in 27. Karen Davis, PhD, the fund’s president, described this outcome as “particularly disturbing considering we lead the world in health care spend- ing.” The fund is a private health foundation that supports re- search into improving quality and efficiency. To arrive at its ratings, the study used six categories: l Patient safety addressed wrong drugs or doses, mistakes in care, and delayed or incorrect test results. l Effectiveness included use of mammograms, flu shots, med- ication reviews, diet and exercise advice, hospital infections and follow-up visits. l Patient centeredness exam- ined such issues as doctor communi- cation, choice, time with the physi- cian, pain management and access to records. l Timeliness addressed appoint- ment wait times, emergency depart- ment lines and access to care at irreg- AMERICAN MEDICAL NEWS AMEDNEWS.COM APRIL 24, 2006 5 Florida passes bill limiting doctors’ share of liability [ PAGE 8 ] MEDICARE / MEDICAID n LEGISLATION AND REGULATION n NATIONAL HEALTH POLICY Government&Medicine United States fares poorly in international patient survey Continued on page 7 $40 $0 $60 $80 $100 Expenditures (in billions) ’98 ’99 ’00 ’01 ’02 ’03 ’04 ’05 8.5% growth in 2005 1.5% growth in 1998 n The Centers for Medicare & Medicaid Services also releases its projection of a 4.6% Medicare pay cut for doctors in 2007. DAVID GLENDINNING AMNEWS STAFF Washington Although Medicare spending on physi- cian services did not rise as much last year as it did the year before, the increase was still large enough to catch the attention of federal officials looking to find more efficiency in the system. The Centers for Medicare & Medicaid Services re- cently estimated that spending on physician ser- vices increased by 8.5% during 2005. In 2004, this rate of growth was 11.4%. But the nearly three percentage point drop was not due to patients using fewer or less complex Medicare services. Instead, the change is largely at- tributable to decreased growth in beneficiary enroll- ment, spending shifts stemming from the Medicare drug benefit and lower reimbursement for physi- cian-administered drugs and lab tests, CMS said. All but one percentage point of the 8.5% increase is due to physicians prescribing more services to their Medicare patients and more intensive levels of services. Physicians stepped up both the number and complexity of basic services, such as follow-up visits; minor procedures, such as physical therapy; and screening tests, such as imaging scans. The 16% growth in imaging service expenditures alone, for example, was nearly twice as high as the average rise in spending for all physician services. Doctors’ greater reliance on CT scans and MRIs is one of the biggest spending drivers in this area, the agency said. Such developments worry those who are charged with making sure the program is paying for what it views as the right patient care. “Understanding the relatively rapid growth in these services, and determining whether there are ways to promote better health while slowing the rapid increase in use of these services, is an increas- ingly important issue,” wrote Herb Kuhn, director of CMS’ Center for Medicare Management, in an April 7 letter to the Medicare Payment Advisory Commission. PHYSICIAN SERVICES Medicare expenditures under the physician fee schedule in recent years have increased by large enough percentages to catch the at- tention of federal officials. With preliminary numbers now in for 2005, here’s how spend- ing has gone up over time: SOURCE: CENTERS FOR MEDICARE & MEDICAID SERVICES Medicare physician spending growth worries U.S. officials Continued on next page HIGH SPENDING, LOW SCORE The United States spends more per person on health care than any of the other five countries studied, but it ranks last overall when scores for patient safety, ef- fectiveness, patient-centeredness, timeliness, efficiency and equity are combined. AUSTRALIA CANADA GERMANY NEW UNITED UNITED ZEALAND KINGDOM STATES OVERALL RANKING 4 5 1 2 3 6 Patient safety 4 5 2 3 1 6 Effectiveness 4 2 3 6 5 1 Patient- centeredness 3 5 1 2 4 6 Timeliness 4 6 1 2 5 3 Efficiency 4 5 1 2 3 6 Equity 2 4 5 3 1 6 Per capita health expenditures $2,903 $3,003 $2,996 $1,886 $2,231 $5,635 NOTE: BASED ON 2004 AND 2005 INTERNATIONAL HEALTH POLICY SURVEYS SOURCE: COMMONWEALTH FUND, APRIL HIGH SPENDING, LOW SCORE The United States spends more per person on health care than any of the other five countries studied, but it ranks last overall when scores for patient safety, effectiveness, patient-centeredness, timeliness, efficiency and equity are combined. AUSTRALIA CANADA GERMANY NEW UNITED UNITED ZEALAND KINGDOM STATES OVERALL RANKING 4 5 1 2 3 6 Patient safety 4 5 2 3 1 6 Effectiveness 4 2 3 6 5 1 Patient- centeredness 3 5 1 2 4 6 Timeliness 4 6 1 2 5 3 Efficiency 4 5 1 2 3 6 Equity 2 4 5 3 1 6 Per capita health expenditures $2,903 $3,003 $2,996 $1,886 $2,231 $5,635 NOTE: BASED ON 2004 AND 2005 INTERNATIONAL HEALTH POLICY SURVEYS SOURCE: COMMONWEALTH FUND, APRIL
- 13. PAGE 13 To balance a story about increases in Medicare Part D prices, this graphic compares information about specific drugs that doctors commonly prescribe. The graphic gives doctors a sense of how many health plans increased the cost of a particular drug, what percent of plans decreased the price and what the median percent change was. The chart worked well because it offered tangible information on drugs that readers commonly prescribe. Had the information been integrated into the story, it would have lost much of its utility. 1 Can we show meaningful comparisons? n Pharmaceutical manufacturers and Medicare drug plans say the studies misrepresent what seniors are actually paying for medications. DAVID GLENDINNING AMNEWS STAFF Washington In the first three months of the Medicare drug benefit, the average wholesale price for roughly 200 of the brand-name drugs most of- ten used by older Americans under- went the single biggest jump in the last six years, according to a recent study by AARP. The average price that drugmakers charged wholesalers for medications increased by 3.9% in the first quarter of the year, four times the rate of gen- eral inflation and the largest quarter- ly increase since AARP began track- ing the figures in 2000. For typical people older than 50 taking four med- ications per day, this means their av- erage annual drug bills increased roughly $240 over the 12 months lead- ing up to the end of March, compared with an increase of roughly $190 dur- ing the previous year. In a separate study, the consumer group Families USA found that Medicare drug plans are responding to the wholesale price increases by boosting what they charge for brand- name medications. For the top 20 drugs prescribed to seniors, the vast majority of Medicare Part D plans quoted higher prices in mid-April than they did in mid-November 2005, when enrollment for the drug benefit began. The study showed that for 15 out of the 20 medications, more than 80% of the plans raised prices over that time period, rather than lowering them or keeping them the same. The median percent change was 3.7%. Both groups said that seniors are being adversely affected because in- surers are passing along the price in- creases to beneficiaries. “Shortly after the [Medicare drug law] was enacted, AARP challenged drug manufacturers to keep the rate of price increase for drugs widely used by older Americans to the rate of general inflation,” the seniors’ group said. “While the rate of increase did slow down beginning in mid-2004, the first quarter 2006 results represent a disturbing reversal of that trend.” Families USA Executive Director Ron Pollack said the data in his group’s report show that federal offi- cials’ assertions about the power of the market to drive prices down are turning out to be wrong. Centers for Medicare & Medicaid Services Ad- ministrator Mark McClellan, MD, PhD, Republican lawmakers and oth- er drug benefit supporters have said that private-sector competition would do a much better job keeping costs in check than government intervention. “At the same time that the Bush ad- ministration and congressional lead- ers are touting the effectiveness of the Medicare drug plans, those plans are quietly raising the prices that they charge,” Pollack said. “As a result, se- niors will pay more and more — as will America’s taxpayers.” Both groups said that allowing the federal government to negotiate with drug companies over the prices they charge, a task that is left to pharmacy benefit managers in the private sec- tor, would help alleviate cost spikes such as the ones seen in recent months. Such direct negotiation, which would require congressional approval, is supported by a range of other groups, including the American Medical Association. More to the story Drug manufacturers and Medicare drug plans challenged both reports, saying that the conclusions were flawed and misleading. Ken Johnson, senior vice president for the Pharmaceutical Research and Manufacturers of America, said that more reliable official government da- ta show recent drug prices tracking the rate of increase in the costs of medical products. Between January and May of this year, that medical in- flation figure was determined to be JULY 10, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS 10 Government & Medicine WEBLINKS http://www.familiesusa.org/ resources/publications/reports/ big-dollars-little-sense.html “Big Dollars, Little Sense: Rising Medicare Prescription Drug Prices,” Families USA, June http://www.aarp.org/research/ health/drugs/aresearch- import-869-2004-06--IB69.html “Trends in Manufacturer Prices of Brand Name Prescription Drugs Used by Older Americans — First Quarter 2006 Update,” AARP, June Consumer groups report hike in Medicare Part D drug prices Continued on page 12 PRESCRIPTION DRUG PRICES ON THE RISE In response to recently increased medication prices from pharmaceutical manu- facturers, the vast majority of Medicare drug plans between November 2005 and April 2006 raised their listed prices for the drugs physicians most commonly prescribe to seniors. Here is a sample of those increases: Drug Name % of plans that % of plans that Median percent increased prices decreased prices price change Zocor (40 mg) 100.0% 0.0% 5.7% Fosamax (70 mg) 98.7% 1.3% 4.9% Lipitor (10 mg) 97.3% 2.7% 6.5% Xalatan (0.005 %) 96.8% 3.2% 4.9% Toprol XL (50 mg) 96.2% 3.8% 3.0% Actonel (35 mg) 96.1% 3.9% 4.9% Celebrex (200 mg) 94.8% 5.2% 6.5% Norvasc (5 mg) 94.6% 5.4% 3.2% SOURCE: FAMILIES USA, “BIG DOLLARS, LITTLE SENSE: RISING MEDICARE PRESCRIPTION DRUG PRICES,” JUNE
- 14. PAGE 14 Although not labeled as a “how to,” this box gives readers tips on how a doctor and patient can challenge an insurer’s decision. Each bullet item begins with a short declarative sentence and is followed by a description of what action to take. It’s a good clip-and-save item, while the story addresses in more depth how physicians could use patients’ help when appealing insurance decisions. 2 Can we offer guidance or tips? How you and your patient can successfully challenge an insurer’s decision: n Appeal every denial. Data show appeals have a high success rate. n Record everything. When you call an insurer for preauthorization or veri- fication of a benefit, make a note of the conversation and the names of people you spoke with. n Send all written correspondence via certified mail and keep records. Time limits can be placed on insurers. Writing things such as, “If you do not respond in five business days it will be as- sumed there are no disputes with the content of this mailing” can sometimes lead to quicker action. n If you don’t get an acceptable answer, go up the chain of com- mand. Copy the plan president with your dispute. For long- standing disputes, send copies of your correspondence to the state insurance commissioner or the state’s attorney’s office. n Get the patient involved. A heartfelt letter explaining how the patient’s life would improve with a certain procedure or treat- ment can be compelling. If you anticipate difficulty, submit the patient’s letter along with the initial claim. n If another physician has more expertise that speaks to the scope of the claim, include a second opinion. n Establish a history with the patient and ensure it is well docu- mented. Insurers place more weight on the opinions of a physi- cian who has an established relationship with the policyholder. n Get the employer or labor union involved. Experts say a com- plaint from an employer who is paying for a large number of in- surance plans gets attention. Share the heavy lifting AMERICAN MEDICAL NEWS AMEDNEWS.COM FEBRUARY 5, 2007 21 BusinessPRACTICE MANAGEMENT n PERSONAL FINANCE n TECHNOLOGY Companies to fund new push for e-prescribing [ PAGE 26 ] Insurance Disputes Patients who deal directly with insurers are often more successful at resolving disputes. But asking a patient to intervene should be a carefully considered decision. Harnessing patient power M ark Granoff, MD, spent more than an hour on the phone with an in- surer trying to get approval for a non-formulary medication. Three separate phone calls and no head- way later, he handed the prover- bial baton to his patient. Dr. Granoff, an internist and geriatrician from Los Angeles, said he generally likes to handle disputes himself. But in cases where he clearly is getting nowhere, the former medical director for Blue Cross of California knows from experience that it’s the patient who holds the power to get things done. Sometimes get- ting the patient involved is key to getting a dis- pute resolved. Insurers “are not anxious to make the pa- tient unhappy,” Dr. Granoff said. “They are the ones paying.” Getting a patient directly involved with in- surance disputes can be tricky and can require some coaching from the physician. But if done at the right time and in an appropriate man- ner, it can pay off. Because patients have been paying more out of pocket for their health care in recent years, some doctors feel patients are more will- ing to fight for benefits. And the time patients spend advocating on their own behalf is time physicians can devote back to patient care. Kathryn Stewart, MD, MPH, a family physi- cian and director of care management at Mt. Sinai Medical Center in Chicago, said she used to spend a lot of time on the phone advocating for patients. “But in this day and age, it’s just not practi- cal for primary care physicians to do that any- more,” Dr. Stewart said. “Doctors are in- creasingly pressed to see more patients, and many are having a difficult time staying out of the red.” While some have taken a proactive ap- proach and gotten the patient involved before a dispute arises, others have found a patient’s voice can be the nudge that results in a change of heart. The people making the decisions “are human, too,” said New York attorney Richard Quadrino, who has represented hundreds of doctors and patients in coverage disputes. When to get patients involved T he choice to get a patient involved should be made judiciously, Quadrino said. “I don’t know if the insurance company re- ally wants to hear from the patient un- less it’s a real medical necessity. And often the doctor can speak to the medical issue.” But Dr. Stewart said having communication between the patient and the insurer can not on- ly result in quicker resolutions to disputes in certain situations, but can also be a good line of defense if the patient is requesting a proce- dure that the doctor knows will not be covered. Because the patient is the client, “it’s really up to the insurance company to explain to the patient why or why not it is being covered,” she said. For example, she recently had a patient who wanted to be transferred to a hospital outside his HMO network. After a fruitless call to the insurer, she told the patient he would have to call the insurer directly if he really thought a transfer should be granted. Jerry Bridge, president of San Diego-based Bridge Practice Management Group, encour- ages physicians to anticipate potential prob- lems and have new patients sign an appeals au- thorization on their first visit. Having that Continued on next page Story by Pamela Lewis Dolan Illustration by Jem Sullivan
- 15. PAGE 15 According to an IOM panel report, 1.5 million people are harmed annually by medication errors. This story explains the panel’s findings and more importantly, provides something the reader can act on: Guidance on how physicians can reduce some of those errors. Presented under a direct headline, “What you can do to reduce errors,” this box delivers 13 tips from the IOM report in simple, useful language. Many reports and studies outline problems, but no answers. This is a strong example of providing both. A CLOSER LOOK AT THE MONEY Commercial entities — pharmaceuti- cal companies and medical device manufacturers — poured a record amount of money into continuing medical education and related education activities in 2005. Propor- tionally, however, their dollars accounted for a smaller piece of the overall CME n A panel’s report calls on all physicians to prescribe electronically by 2010, but experts say that’s a reach. KEVIN B. O’REILLY AMNEWS STAFF At least 1.5 million people are injured annually by preventable medication errors that occur at every stage of the process, from prescribing to dispensing to patient administration, according to a July Insti- tute of Medicine report. The new report says physicians, nurses, pharma- cists, patients and drugmakers must work together to combat the many factors that contribute to the persistence of these errors, which the IOM earlier reported kill an estimated 7,000 people a year. “The 1999 report [“To Err is Human”] raised awareness about errors in general,” said J. Lyle Bootman, PhD, ScD, co-chair of the IOM Committee on Identifying and Preventing Medication Errors and dean of the University of Arizona College of Pharmacy. “The current report makes clear that we still have a long way to go.” Albert W. Wu, MD, MPH, a panel member and professor of health policy and management and in- ternal medicine at Johns Hopkins University in Baltimore, said the report’s findings make clear that medication errors are the most far-reaching of medical errors. “I’m a patient-safety researcher, and even as we went through the process I was surprised by just how common and how serious a problem this is,” Dr. Wu said. “We all need to wake up and take a part in fixing it.” Most important for physicians, the panel called on all prescribers to have a plan to implement an electronic prescribing system by 2008 and to have such systems in place by 2010. Wilson D. Pace, MD, a panel member and Green- Edelman Chair for Practice-based Research at the University of Colorado, said even the most talented physicians need electronic systems to help them prescribe safely. “With 15,000 medications available, it’s virtually impossible to track all of those anymore just using your memory,” Dr. Pace said. “Electronic prescrib- n But at the local level, some CME providers say they have found that there’s less in the pot for them. MYRLE CROASDALE AMNEWS STAFF Spending on continuing medical edu- cation over a one-year period was up nearly 10% in 2005, to $2.25 billion, but a smaller percentage of that money came from pharmaceutical compa- nies and other commercial interests than in years past, according to the re- cently released 2005 annual report of the Accreditation Council for Contin- uing Medical Education. Commercial interests — drug com- panies and medical device manufac- turers — increased their giving to CME providers to $1.35 billion in 2005 for such items as education grants and exhibit space. But because of increased money from registration fees and noncom- mercial groups, the share of spending by pharmaceutical and device manu- facturers covering CME costs as well as CME-related advertising and ex- hibit fees fell from 62% in 2004 to 60% in 2005. Part of this decrease is also attrib- uted to ACCME changing the defini- tion of commercial support to exclude money or services from nonprofit or government organizations and non- health care-related companies. Increased total spending in 2005 al- so translated into an increased num- ber of total CME activities, with the national specialty societies and large CME providers still capturing a sig- nificant portion of pharmaceutical dollars. Despite the net increase on paper, locally produced CME is facing a re- duction in commercial educational grants as state medical societies and small- and mid-sized hospitals capture a smaller share of commercial CME support, some experts say. With pharmaceutical and device manufacturers the largest contribu- tors to educational activities for prac- ticing physicians, say the experts, this could signal a reduction in the amount of CME available for physi- cians at the local level. Murray Kopelow, MD, ACCME chief executive, said he’s heard from CME providers that commercial CME funding is falling, particularly on the local level, but said the ACCME does not capture data at the local level. AMERICAN MEDICAL NEWS AMEDNEWS.COM AUGUST 21, 2006 9 Professional IssuesHEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION Calif. high court shields peer reviewers [ PAGE 13 ] MEDICATION ERRORS ADD UP The toll of preventable medication errors is uncertain, but in a July report, an Institute of Medicine panel estimates that at least 1.5 million people are harmed an- nually by preventable medication errors. Here’s a breakdown of these estimates: 400,000preventable drug-related injuries occur each year in hospitals. It costs an extra $3.5 billion to treat those injuries. 800,000preventable drug-related injuries occur in long-term care settings. 530,000preventable drug-related injuries occur among Medicare recipients in outpatient clinics. In 2000, it cost $887 million to treat those injuries. 25%of all medication errors are due to similar drug names. 33%of drug errors, including 30% of deaths, are due to poor labeling and packaging. E-prescribing urged as one error-prevention strategy More dollars flow into continuing medical education Continued on next page Medication mix-ups prevalent Continued on page 12 $0.0 $0.5 $1.0 $1.5 $2.0 $2.5 2003 2004 2005 BILLIONS OF DOLLARS SPENT $2.25 $2.05 $1.77 60% 62% 65% 35% 38% 40% CME FUNDING Including pharmaceutical and medical device manufacturer spending, physician registration fees and other sources of income. WHERE CME DOLLARS CAME FROM n Commercial entities n Registration fees and other noncommercial CME income HOW COMMERCIAL SPENDING BREAKS DOWN Education, Advertising, Physician fees, grants, support exhibit income other income 2003 55% 10% 35% 2004 52% 10% 38% 2005 50% 10% 40% SOURCE: ACCME 2005 ANNUAL REPORT WHAT YOU CAN DO TO REDUCE ERRORS A July Institute of Medicine report says office-based physicians should take these steps to minimize medication errors: n Put an electronic prescribing plan in place by 2008; implement e-prescribing by 2010. n Reconcile medications at transition points — admission, discharge and transfer. n Create a routine to reconcile medication changes with the pharmacy record. n Keep an accurate medication list for each patient, including over-the-counter and complementary and alternative medications. Ask patients to bring their medications in periodically to keep the list up to date. n Do the following when prescribing new medication: Ask about allergies, inform the patient of indications for all medications, explain common or significant side effects, consult electronic or other reference sources for questions, avoid abbreviations and in- clude patient age and weight when applicable. n Ask regularly whether patients are taking their medications, including as-needed drugs. If they aren’t taking the medication, it may signal that a patient had an adverse reaction to the drug. n Monitor the patient for response to medication therapy and ask regularly about side effects or adverse drug events. n Standardize communication about prescriptions within the practice; standardize and improve handoffs to the primary pharmacist. n Ask the primary pharmacy about the patient’s refill history. n Work as a team with the primary pharmacist and nurses. n Minimize the use of free samples; when dispensing free samples, apply standards similar to those a pharmacy would use. n Exercise particular caution in high-risk situations, such as times when a physician is stressed, sleep-deprived, angry or is supervising inexperienced personnel. n Report errors and adverse drug events to the Medication Errors Reporting Program, jointly run by U.S. Pharmacopeia and the Institute for Safe Medication Practices as well as the appropriate patient-safety organization or authority, depending on the state. 2 Can we offer guidance or tips?
- 16. PAGE 16 STANFORD’S RULES Medical staff, faculty, students and trainees at the Stanford University School of Medicine, Stanford Hospital and Clinics and the Lucile Packard Children’s Hospital must follow these standards: n No personal gifts of any size from industry, under any circumstances. n No compensation for listening to a sales talk. n No compensation — including defraying costs — for attending a continuing medical education event or other activity, unless an individual is presenting at the event. n No sales representatives in patient-care areas, unless it’s to train staff for research or on how to operate clinical equipment. All visits must be by appointment. n No sales representative visits with physicians without an appoint- ment. These appointments may be made at the physician’s discretion. n No industry support directly to students and trainees. The support must be provided through the school and must be free of any actual or perceived conflict of interest and specifically for educational purposes. SOURCE: STANFORD UNIVERSITY SCHOOL OF MEDICINE 2 Can we offer guidance or tips? For this page 1 story, Stanford is the first school highlighted in an exploration of academic medical centers taking firmer stances against pharmaceutical marketing efforts on campus. It is not until well into the jump that other institutions are discussed at length, so it makes sense that Stanford’s rules get prominence. The guidelines staff and students must follow are already written clearly and make a compelling graphic about real-world expectations. The story gets into the policies of other schools and changes that have come about in response and also offers a graphic on the JAMA article challenging academic medical centers to take the lead on conflict-of-interest reforms. Providing Stanford’s clearly stated guidelines helps the story become more tangible. n Stanford, Yale and the University of Pennsylvania have adopted policies to create a brighter line between medicine and marketing. MYRLE CROASDALE AMNEWS STAFF On Oct. 1, Stanford University School of Medicine in California closed its last avenue for pharmaceutical mar- keting on campus, shutting down drug company freebies no matter what their size. The ban includes everything from free lunches to pens touting the latest medication to hit the market. Also, pharmaceutical sales representatives must make appointments if they want to talk with physicians. The stricter rules come after the school prohibited drug samples several years ago, ex- cept at medical students’ free clinics. Stanford is one of a handful of acad- emic medical centers expanding con- flict-of-interest rules beyond research to include smaller gifts aimed at influ- encing physicians’ clinical practices, namely prescribing. Although there is no hard number on how much is spent, Stanford esti- mates that drug companies lay out about $250,000 annually on meals there. Nationwide, the pharmaceuti- cal industry estimates that it spends $21 billion a year on marketing, though some contend that this figure is too low. “There’s a growing awareness that pharmaceutical promotions subtly, and not so subtly, impact physicians’ decisions,” said internist Clarence Braddock, MD, MPH, an associate professor at Stanford and a member of the Stanford Center for Biomedical Ethics. “Even if [you believe] there’s www.amednews.com AMERICAN MEDICAL NEWS 515 NORTH STATE CHICAGO, IL 60610 ★ ★ ★ CLASSIFIED ADVERTISING – PAGES 37-38 October 9, 2006 VOLUME 49 n NUMBER 38American Medical Souped-up EMR Physicians who want to integrate a patient’s genetic code into treatment using bioinformatics need the technology and ability to analyze the data. In Business, page 21 Specialty hospital fight goes to state’s high court Government & Medicine, page 7 Online prescribing spurs criminal charges Professional Issues, page 16 Hospital competition breeds quality Opinion, page 30 Doctors wary about flu vaccine deliveries Health & Science, page 32 Promise and challenges In the last of a three-part series, doctors try to look beyond today’s crisis and see what lies ahead in fixing the Medicare pay system. In Government & Medicine, page 5 Cancer, families and physicians The book A Lion in the House features insights from parents, doctors and others who cared for five children at a Cincinnati hospital. In Professional Issues, page 12 Restricting drug reps Some medical schools say no to free lunch Physician service growth rate slows, easing Medicare premium increase STANFORD’S RULES Medical staff, faculty, students and trainees at the Stanford University School of Medicine, Stanford Hospital and Clinics and the Lucile Packard Children’s Hospital must follow these standards: n No personal gifts of any size from industry, under any circumstances. n No compensation for listening to a sales talk. n No compensation — including defraying costs — for attending a continuing medical education event or other activity, unless an individual is presenting at the event. n No sales representatives in patient-care areas, unless it’s to train staff for research or on how to operate clinical equipment. All visits must be by appointment. n No sales representative visits with physicians without an appoint- ment. These appointments may be made at the physician’s discretion. n No industry support directly to students and trainees. The support must be provided through the school and must be free of any actual or perceived conflict of interest and specifically for educational purposes. SOURCE: STANFORD UNIVERSITY SCHOOL OF MEDICINE Continued on next page n Meanwhile, beneficiaries with higher incomes will pay bigger premiums next year as the result of a 2003 law. DAVID GLENDINNING AMNEWS STAFF Washington Medicare beneficiaries next year will not see their premiums rise as much as originally thought now that federal officials have downgraded their projections of how much doctor care is costing the program. The standard 2007 monthly premi- um for Medicare Part B, which covers outpatient physician care, will in- crease by $5 to $93.50. The Centers for Medicare & Medicaid Services esti- mated in July that the premium would jump by nearly $10 to $98.40. The new figure will be the smallest in- crease in six years. Beneficiaries will pay less because federal officials have revised the rate at which spending on physician care is increasing, said CMS Administra- tor Mark McClellan, MD, PhD. In par- ticular, the growth rate for physician services in 2005 slowed compared with recent years, altering projec- tions for the future. CMS originally thought that the amount of services that doctors were billing was spiking, but now officials have realized that doctors simply were filing claims more efficiently and re- ceiving payments more quickly. The effect of the higher efficiency made it look to actuaries as if doctors were boosting the total level of care they were prescribing to their patients. The amount that seniors are ex- pected to pay to receive coverage un- der the program is dependent in part on the amount and complexity of ser- vices that doctors provide. Because Part B premiums are calculated to cover 25% of the program’s costs, any increases in physician services result Continued on page 4