PHYSIOLOGY OF SWALLOWING: A COORDINATED PROCESS
•Transferir como PPT, PDF•
103 gostaram•27,198 visualizações

Oral, Pharyngial and Neural conrol in detail

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (14)
Semelhante a PHYSIOLOGY OF SWALLOWING: A COORDINATED PROCESS
Semelhante a PHYSIOLOGY OF SWALLOWING: A COORDINATED PROCESS (20)
Mais de Liju Rajan
Mais de Liju Rajan (8)
Último
Último (20)
PHYSIOLOGY OF SWALLOWING: A COORDINATED PROCESS
- 1. PHYSIOLOGY OF SWALLOWING PRESENTED BY Dr. Liju Rajan
- 2. REFERENCE Scott Brown otorhinolaringology and Head and Neck Surgery – 7th Edition Cummings ORL-HNS 6th Edition Glyton And Hall text book of Physiology
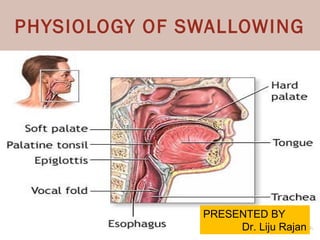
- 3. Swallowing requires the coordinated activity of muscles in three regions of the head and neck: the oral cavity, The pharynx and larynx, and the oesophagus.
- 4. Swallowing involves the passage of a bolus of food or liquid from the oral cavity to the stomach via the pharynx and oesophagus, passing over the entrance to the laryngeal vestibule The elevators and depressors of the jaw play a key role in bolus preparation before the swallow is initiated by grinding and reducing the food between the teeth.
- 6. Bolus formation is also a function of the tongue, the intrinsic muscles of which are mainly responsible for changing the shape of the tongue and the extrinsic muscles altering its position in the mouth. The actions of these two groups of muscles are not independent since changes in shape result in changes in position and vice versa
- 7. The actions of the tongue and jaw muscles in bolus formation are aided by that of the lips in maintaining a seal, the buccinator muscle of the cheek in returning food from the vestibule into the oral cavity and the soft palate in preventing nasal regurgitation and premature movement of material into the oropharynx
- 8. On leaving the oral cavity, food enters the pharynx, a midline tube approximately 15 cm long continuous with the oesophagus below and the nasal cavities above and the larynx which opens on its anterior wall a natural division of the pharynx into three regions: nasopharynx, oropharynx and laryngopharynx,
- 9. The remainder of the pharynx is composed, like the whole of the gastrointestinal tract, of four layers: the outer areolar, the muscular, the submucous and the inner mucous membrane. The muscular layer is composed of circular and longitudinal muscles
- 10. The circular muscles are arranged as a triad, the superior, middle and inferior constrictors, with the latter being further subdivided into a thyropharyngeus and cricopharyngeus part With the exception of the cricopharyngeus, the constrictor muscles are paired and attach to a posterior midline raphe. The cricopharyngeus forms a distinct sphincter at the point where the laryngopharynx joins the oesophagus. There are two discrete longitudinal muscles on each side, the palatopharyngeus and the stylopharyngeus.
- 12. ORAL PHASE ( Preparatory and Proper)
- 13. Oral Phase - Preparatory The oral preparatory phase is where food is readied for swallowing by reducing and mixing it with saliva by the muscles of the jaw and oral cavity. The jaw is closed by the jaw elevators, temporalis, masseter and medial pterygoid and chewing uses a combination of elevators and depressors.
- 15. The lips maintain a tight seal under the action of the orbicularis oris The buccinator is used to return food from the vestibule during the process of mastication. Throughout this phase the soft palate is lowered under the action of the palatoglossus and palatopharyngeus which approximate the arches of the same name to the dorsal aspect of the posterior part of the tongue. The airways remain open. Traditionally, the oral cavity was thought to be sealed posteriorly though recent work indicates that this may not always be the case.
- 17. ORAL PHASE PROPER The oral phase proper involves several distinct muscle actions. The tongue is moved by the action of the intrinsic muscles together with the genioglossus which elevates the tongue tip and blade of the tongue towards the hard palate. A prerequisite for this is mandibular elevation and although the mouth does not have to be completely closed during swallowing, it is hard to swallow with the mouth more than a little open The elevation of the mandible assists the suprahyoid muscles in raising the hyoid bone.
- 19. The elevation of the floor of the mouth is accompanied by lifting the tongue under the action of the stylohyoid. Simultaneously,the tongue is flattened and the bolus is moved back by these muscles together with the superior longitudinal and transversus muscles as the tongue fills the oral cavity. As the bolus reaches the back of the tongue,now deeply grooved, the soft palate is elevated to protect the nasopharynx from the entry of food and closes the airways. The soft palate is elevated by the levator and tensor veli palatini.
- 21. PHARYNGEAL PHASE
- 22. Pharyngeal phase As the bolus is moved back by the tongue to enter the pharynx, a sequence of events is initiated that ensures that the airways are protected during bolus transport Firstly, diaphragmatic contraction is inhibited making simultaneous breathing and swallowing impossible under normal circumstances. At the same time, the soft palate is elevated to ensure a sphincteric closure of the nasopharynx. Finally, the vocal cords start to close to protect the airways.
- 23. The initiation of swallowing involves contact of the food with the faucial arches or with the mucosa overlying the posterior pharynx in the region that is innervated by the glossopharyngeal nerve Recent work involving simultaneous videofluoroscopy and endoscopy suggests that the ‘trigger point’ may be the ‘summation of afferent signals for the entire oropharyngeal sensory field’.
- 24. bolus enters the oropharynx touches keytrigger points a reflex is initiated in which the constrictors relax to dilate the pharynx The pharynx and larynx are raised by the longitudinal muscles The bolus is propelled over the epiglottis by the action of the constrictors contracting in sequence. The larynx is then closed by contraction of the muscles of the laryngeal inlet
- 25. Bolus material is seen in the valleculae and even the pyriform sinuses in60 percent of liquid and 76 percent of solid swallows before the swallow is triggered. This calls into question the term ‘premature spillage’ as an indicator of dysphagia It is often said that once the bolus of food has passed the palatoglossal and palatopharyngeal arches then swallowing becomes reflexive. While it is true that swallowing is automatic once initiated, many people can voluntarily delay their swallowing up to a certain point
- 26. The bolus enters the pharyngeal space there is widening of pharynx and its raised This is partly due to the relaxation of the pharyngeal constrictors and partly to the anterior movement of the pharynx as the hyoid bone is drawn forward under the elevating action of the suprahyoid muscles. Laryngeal elevation also occurs as the suprahyoid muscles move the hyoid bone anteriorly, contributing to pharyngeal dilation. Raising the larynx narrows the laryngeal inlet and moves it towards the pharyngeal surface of the epiglottis as the laryngeal cartilages move anteriorly. The interarytenoid, aryepiglottic and thyroepiglottic muscles all help to close the margin of the laryngeal aditus in the manner of a drawstring purse.
- 29. Pharyngial Phase – Epiglottis movement The movement of epiglotis is usually described as occurring in two distinct stages,with the first bringing the epiglottis from a vertical to a nearly horizontal position and the second moving the upper third of the epiglottis to below the horizontal to cover the narrowed laryngeal aditus.
- 30. Some authors state that both actions occur passively due to movements of adjacent structures and forces generated by compression of the pre-epiglottic adipose fat pad, and within the ligamentous attachments of the epiglottis, or by a combination of the two. Others claim that the second epiglottic movement is generated actively by the action of the thyroepiglottic and hyoepiglottic muscles. In favour of an entirely passive mechanism, it has been claimed that these muscles are too sparse to generate adequate force and that some of their attachments are not consistent with such an action.
- 31. Pharyngeal phase - pyriform sinuses As the food passes over the posterior part of the curved epiglottis, it is diverted into the lateral food channels and the pyriform fossae Early studies suggested that airway protection was further maintained by the bolus splitting after passing the base of tongue, moving laterally through the pyriform sinuses and rejoining to pass into the oesophagus. Recent evidence has shown that solids tend to go straight over the epiglottis, while liquids are diverted laterally.
- 32. The pharynx constricts behind the bolus as the superior constrictor muscle contracts. The bolus is carried down the pharynx by a coordinated peristaltic wave in which the three constrictor muscles contract in the appropriate sequence.
- 33. Oesophageal phase The cricopharyngeus relaxes and the anterior superior movement of the laryngohyoid complex acts to open the upper oesophageal sphincter. The bolus passes through the sphincter and moves along the oesophagus by peristalsis. The levator and tensor veli palatini relax lowering the soft palate. The laryngeal vestibule opens, the hyoid drops and the vocal cords open. This opening ofthe glottis at the very end of the oropharyngeal swallowsequence is part of the airway protection mechanism.
- 35. NEURAL CONTROL
- 36. NEURAL CONTROL Neural control of the complex activity of healthy swallowing involves a number of different regions of the central nervous system (CNS) This extends from motor neurons within motor neuclei of brainstem up to cortex. The act of swallowing is regulated by sensory feedback although its importance is only recently found. The initiation of swallowing can either be as a voluntary act or a reflex as the result of stimulation of the appropriate mucosa in the oral cavity
- 37. Neuronal control - Cortex The voluntary initiation of swallowing involves bilateral areas of the prefrontal, frontal and parietal cortices. These include the face areas of both the primary sensory and motor cortex, as well as the prefrontal swallowing areas which are located just anterior to the face region of the precentral gyrus in the primary motor cortex, corresponding to Brodman’s area 6.
- 39. Neuronal control - Cortex These studies show that the lower precentral gyrus and posterior inferior frontal gyrus control the oral phase of swallowing. The pharyngeal and oesophageal phases of swallowing are controlled from more rostromedial regions of the cortex within the anterior inferior and middle frontal gyri. In most people, swallowing control is asymmetrical with the projection from one hemisphere being larger than the other, independent of handedness. this explains both the prevalence of swallowing problems following stroke and the recovery that occurs in most patients over a period of weeks
- 41. Other cortical areas that have been implicated in swallowing include the frontal operculum, orbitofrontal cortex and the insula. The insula lies deep to the lateral fissure and is covered by the operculae of the frontal, parietal and temporal lobes and strokes here can induce dysphagia. This suggests that cortical control of swallowing is hierarchical with precentral areas of the cortex being influenced by deeper and more caudal centres
- 42. Neuronal control – Brain Stem There are important areas within the brainstem necessary for the control of swallowing and these are located particularly within the medulla. Descending pathways project to these medullary swallowing centres from the frontal swallowing areas within the cortex. These probably include pathways in both the dorsolateral and ventromedial descending systems through the ventral and lateral corticobulbar tracts.
- 43. Swallowing is initiated by touch sensation or pressure from the liquid or food within the posterior part of the oral cavity, epiglottis or oropharynx. Thus the nuclei receiving afferent input from these regions, which include the nucleus tractus solitarius and spinal trigeminal nucleus,
- 44. The efferent pathways from the medulla and pons to the muscles involved in swallowing involve several cranial motor nuclei. The most important are the Nucleus ambiguus for the muscles of the palate, pharynx and larynx the hypoglossal nucleus for the muscles of the tongue and the motor nuclei of the trigeminal and facial nerves for the muscles of the jaws and lips. In addition, motor neurones within the cervical spinal cord control the muscles of the neck including the infrahyoid.
- 48. Between these input and output pathways are interposed two main groups of neurones that appear to be essential for the coordination and regulation of swallowing by the medulla. The first lies in the dorsal region ofthe medulla above the nucleus of the solitary tract. A second group lies more ventrally around the nucleus ambiguus The dorsal group would appear to be the site of convergence of sensory input from the various nuclei and is probably important in the sequencing of swallowing. The ventral group distributes outputs to the various cranial nerve motor nuclei.
- 49. RESPIRATION AND SWALLOWING There appears to be an individual swallowing respiration pattern that matures in the teenage years and is remarkably consistent thereafter The existence of such an individual pattern may present a risk for aspiration if it is disturbed. Disease or injury may upset this delicate balance, whether due to neurological insult or common otolaryngological conditions such as posterior laryngitis
- 50. Aspiration into upper trachea. Reproduced by permission of the BMJ Publishing
- 51. Clearly, ventilation has to besuspended during pharyngeal transit of the bolus . This is known as the period of swallow apnoea and is typically less than one second in length, corresponding to the duration of the reflex part of the swallow in its pharyngeal phase. The duration of swallow apnoea is dependent upon bolus volume and possibly bolus consistency RESPIRATION TRACE SOUND TRACE Apnoeic period
- 52. In a study of 60 people, one of the largest to date, Hiss et al. reported that increasing the bolus volume over 15mL corresponded with increased swallow apnoea. The effect of bolus consistency is less clear. There is evidence to suggest that solids increase apnoea but sample numbers are too small to be unequivocal
- 53. Swallowing tends to occur during the expiration phase of respiration. Expiration occurs after 80–100 percent of healthy swallows. This is likely to be a protective mechanism: material left in the laryngeal vestibule post swallow will be moved to the pharynx rather than sucked into the lungs. Post-swallow inspiration is more common in populations with impaired swallowing. There does not seem to be an effect of bolus volume or gender on the exhale–swallow–exhale pattern.
Notas do Editor
- T