
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Interpretation of X-Ray and other imaging
Similar to Interpretation of X-Ray and other imaging (20)
More from drmainuddin
Recently uploaded
Recently uploaded (20)
Interpretation of X-Ray and other imaging
- 1. Imaging Dr Md Main Uddin Assistant Professor (Medicine) Cox’s Bazar Medical College
- 2. Modalities • X-Ray CXR Plain abdominal x-ray • Computed tomography • Magnetic resonance imaging • Ultrasound • Nuclear imaging
- 4. Points to note when assessing the chest X-ray • Name of patient and date (and time) of X-ray • Position of the patient • Position of the trachea • Outline of heart • Outline of mediastinum • Diaphragm • Lung fields • Bony skeleton
- 5. Assessing the chest X-ray • The position of the patient • Is the patient straight or rotated? If straight, the inner ends of the clavicles will be equidistant from the midline of the vertebral body. This is important because any rotation will tend particularly to alter the appearance of the mediastinum and the hilar shadows. • The outline of the heart and the mediastinum • Is this normal in size, shape and position? • The position of the trachea • This is seen as a dark column representing the air within the trachea. Is the trachea centrally placed or deviated to either side?
- 6. The Chest X-Ray Techniques – Projection •P-A (relation of x-ray beam to patient)
- 7. CXR Interpretation PA vs. AP views
- 9. Cardiac Silhouette 1. R Atrium 2. R Ventricle 3. Apex of L Ventricle 4. SVC 5. IVC 6. Tricuspid Valve 7. Pulmonary Valve 8. Pulmonary Trunk 9. R PA 10. L PA
- 10. Assessing the chest X-ray • The diaphragm • Can the diaphragm be seen on each side? Is it normal in shape and position? Normally, the anterior end of the sixth or seventh rib crosses the mid-part of the diaphragm on each side, although the diaphragm on the right is usually a little higher than on the left. Are the cardiophrenic angles clearly seen?
- 11. The lung fields • For radiological purposes, the lung fields are divided into three zones: • The upper zone extends from the apex to a line drawn through the lower borders of the anterior ends of the second costal cartilages. • The mid-zone extends from this line to one drawn through the lower borders of the fourth costal cartilages. • The lower zone extends from this line to the bases of the lungs.
- 12. • Each zone is systematically examined on both sides, and any area that appears abnormal is carefully compared with the corresponding area on the opposite side. The horizontal fissure, which separates the right upper and middle lobes, may sometimes be seen running horizontally in the third and fourth interspaces on the right side.
- 13. The bony skeleton • Is the chest symmetrical? • Is scoliosis present? • Are the ribs unduly crowded or widely spaced in any area? • Are cervical ribs present? • Are any ribs eroded or absent? • As well as the standard AP view, lateral views are sometimes carried out to help localize any lesion that is seen.
- 14. In examining a lateral view follow this plan: • Identify the sternum anteriorly and the vertebral bodies posteriorly. The cardiac shadow lies anteriorly and inferiorly. • There should be a lucent (dark) area retrosternally which has approximately the same density as the area posterior to the heart and anterior to the vertebral bodies. Check for any difference between the two, or for any discrete lesion in either area. • Check for any collapsed vertebrae. • The lowest vertebrae should appear darkest, becoming whiter as they progress superiorly. • Interruption of this smooth gradation suggests an abnormality overlying the vertebral bodies involved.
- 15. Figure 10.8 A lateral chest X-ray
- 16. The normal chest X-ray
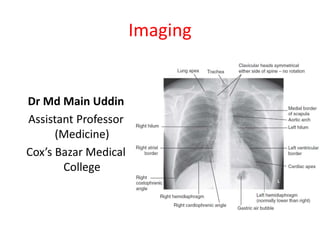
- 17. The normal chest X-ray • Chest X-ray PA view showing trachea is central, lung fields are clear, both hilum are normal, mediastinum is normal, cardiac shadow is normal in size and contour, both costophrenic and cardiophrenic angles are clear, diaphragm is normal in shape and position, bony skeleton and soft tissue shadows are normal.
- 19. Pneumonia (consolidation) of the right middle lobe • CXR PA view showing opacification beneath the horizontal fissure and loss of normal contrast between the right heart border and lung. Suggestive of Rt sided consolidation.
- 21. RML pneumonia
- 22. RLL pneumonia
- 23. LLL pneumonia
- 24. • Figure 10.18 • Chest X-ray showing a right basal pneumonia in a previously fit 40-year-old man with fever, breathlessness, central cyanosis and pleuritic pain. Chest signs included bronchial breathing and a pleural rub in the right lower zone. The cyanosis was due to the shunting of deoxygenated blood through the consolidated lung, the increased respiratory rate leading to a low PaCO2 because of increased clearance of carbon dioxide by the unaffected alveoli. Streptococcus pneumoniae was grown on blood cultures.
- 25. 25154 slides Right Middle Lobe Pneumonia 25
- 26. 26154 slides Left Lower Lobe Pneumonia 26
- 29. • Chest X-ray PA view showing the sharply defined edge of the deflated lung with complete translucency (no lung markings, no vascular markings) between this and the chest wall in the Rt side with shifting of mediastinum to left. • Suggestive of Rt Tension Pneumothorax
- 30. Pneumothorax
- 32. 32154 slides Collapsed Right Lung Tension Pneumothorax: Requires chest tube Tracheal Deviation What would you do with this patient? 32
- 33. 34
- 37. • Chest X-ray PA view showing dense homogenous opacity at the Rt lung base with curved upper border, blunting the costophrenic angle and ascending towards the axilla. Suggestive of Rt Pleural Effusion • Around 200 mL of fluid is required in order for it to be detectable on a PA chest X-ray.
- 38. Pleural Effusion
- 39. • Figure 10.17 • Chest X-ray showing a large left pleural effusion in a young man with a 4- month history of malaise, fever, night sweats and weight loss. The diagnosis of tuberculosis was confirmed on histology of a pleural biopsy and culture of the pleural fluid.
- 41. 42154 slides Large Pleural Effusion 42
- 43. Emphysema
- 44. Emphysema • Chest X-ray PA view showing hypertransluscencs lung fields, low flat diaphragm and widening of rib space, suggestive of Emphysema.
- 45. 46154 slides Enlarged Retrosternal Air Space Flattened Diaphragms Bullous Emphysema 46
- 48. Figure 11.32 Left atrial dilatation. This is a penetrated PA chest X-ray in a patient with mitral stenosis. The dilated left atrium causes a bulge on the left heart border below the pulmonary artery which is also dilated, widening of the carina and the double density sign at the right heart border.
- 49. Figure 11.31 Pericardial effusion with tamponade: There is a left hilar mass caused by carcinoma. Pericardial infiltration has produced effusion and tamponade, evidenced by the severely enlarged and globular cardiac silhouette. Malignant disease is now the most common cause of tamponade in most developed countries.
- 50. Figure 11.35 Chest X-ray in acute left ventricular failure: the patient had severe pulmonary oedema caused by acute myocardial infarction. The heart is not yet enlarged, but there is prominent alveolar pulmonary oedema in a perihilar (‘bat’s- wing’) distribution. Note the bilateral pleural effusions.
- 61. Hilar mass
- 62. Multiple Masses
- 63. Hilar Lymphadenopathy - BL
- 65. Air under the diaphragm
- 67. 68154 slides Multiple Nodules: Diagnosis? Metastases 68
- 68. 69154 slides NormalHilar and Mediastinal Lymphadenopathy Diagnosis? 69
- 69. 70154 slides Hilar Lymphadenopathy on lateral 70 Normal
- 75. Chest X-ray An approach to interpreting the chest X-ray • Name, date, orientation • Films are postero-anterior (PA) unless marked AP to denote that they are antero-posterior • Lung fields • Equal translucency? • Check horizontal fissure from right hilum to sixth rib at the anterior axillary line • Masses? Consolidation? Cavitation? • Lung apices • Check behind the clavicles: Masses? • Consolidation? Cavitation?
- 76. An approach to interpreting the chest X-ray • Trachea • Central? (Midway between the clavicular heads) • Paratracheal mass? Goitre? • Heart • Normal shape? • Cardiothoracic ratio should be < half the intrathoracic diameter) • Retrocardiac mass? • Hila • Left should be higher than right • Shape? (Should be concave laterally; if convex, consider mass or lymphadenopathy) • Density?
- 77. Interpreting the chest X-ray • Diaphragm • Right should be higher than left • Hyperinflation? (No more than 10 ribs • should be visible posteriorly above the diaphragm) • Costophrenic angles • Acute and well defined? (Pleural fluid or thickening, if not) • Soft tissues • Breast shadows in females • Chest wall for masses or subcutaneous emphysema • Bones • Ribs, vertebrae, scapulae and clavicles • Any fracture visible at bone margins or lucencies?
- 78. Interpreting the chest X-ray • This is useful for determining the size and shape of the heart, and the state of the pulmonary blood vessels and lung fields. Most information is given by a posteroanterior (PA) projection taken in full inspiration. • Anteroposterior (AP) projections are convenient when patient movement is restricted but result in magnification of the cardiac shadow.
- 79. Interpreting the chest X-ray • ‘Cardiomegaly’ is the term used to describe an enlarged cardiac silhouette where the ‘cardiothoracic ratio’ is greater than 0.5. • It can be caused by chamber dilatation, especially left ventricular dilatation, or by a pericardial effusion.