Ischemic Colitis, Acalculous Cholecystitis And Catastrophic Longitudinal Transverse Myelopathy In Antiphospholipid Syndrome And Sjogrens Vasculitis
•
2 gostaram•585 visualizações

Recomendados

Recomendados
Mais conteúdo relacionado
Mais de Bassel Ericsoussi, MD
Mais de Bassel Ericsoussi, MD (20)
Último
Último (20)
Ischemic Colitis, Acalculous Cholecystitis And Catastrophic Longitudinal Transverse Myelopathy In Antiphospholipid Syndrome And Sjogrens Vasculitis
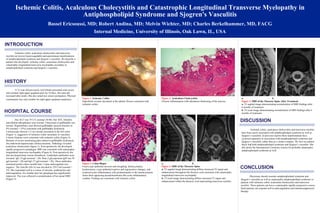
- 1. Ischemic Colitis, Acalculous Cholecystitis and Catastrophic Longitudinal Transverse Myelopathy in Antiphospholipid Syndrome and Sjogren's Vasculitis Bassel Ericsoussi, MD; Robert Andina, MD; Melvin Wichter, MD; Charles Berkelhammer, MD, FACG Internal Medicine, University of Illinois, Oak Lawn, IL, USA Ischemic colitis, acalculous cholecystitis and transverse myelitis are known hypercoagulable and autoimmune manifestations of antiphospholipid syndrome and Sjogren’s vasculitis. We describe a patient who developed ischemic colitis, acalculous cholecystitis and catastrophic longitudinal transverse myelopathy secondary to antiphospholipid syndrome and Sjogren’s vasculitis. HOSPITAL COURSE INTRODUCTION Her ALT was 74 U/L (normal 10-40). Her AST, bilirubin and alkaline phosphatase were normal. Ultrasound of gallbladder was normal. Hepatobiliary scan showed gallbladder ejection fraction of 4% (normal < 35%) consistent with gallbladder dyskinesia. Colonoscopy showed 1-2 cm circular ulceration in the left colon (Figure 1), suggestive of ischemic colitis secondary to vasculitis. Colonic biopsies were consistent with ischemic colitis (Figure 2). Because of severe unrelenting pain related to gallbladder dyskinesia, she underwent laparoscopic cholecystectomy. Pathology revealed acalculous cholecystitis (figure 3). Post-operatively she developed rapidly progressive paraplegia. MRI was consistent with catastrophic longitudinal transverse myelopathy (Figure 4). Post-operatively she also developed deep venous thrombosis. Cardiolipin antibodies were elevated: IgG 34 gpl (normal < 20). Beta-2-glycoprotein IgM was 95 gpl (normal < 20) and IgG 57 gpl (normal < 20). These antibodies remained positive three months later. Lupus anticoagulant was negative. The Anti-Ro (SS-A) was elevated at 129 U/ml (normal < 25). She responded well to a course of steroids, azathioprine and anticoagulation. Six months later her paraplegia has significantly improved. This was reflected in normalization of her spinal MRI (Figure 5). A 52 year old previously well female presented with severe and constant right upper quadrant pain for 10 days. Her pain did increased after meals. She also noted new onset constipation. Physical examination was only notable for right upper quadrant tenderness . a. b. Figure 4. MRI of the Thoracic Spine a. T2 sagittal image demonstrating diffuse increased T2 signal and enhancement throughout the thoracic cord consistent with catastrophic longitudinal transverse myelopathy. b. T2 axial image demonstrating diffuse increased T2 signal and enhancement within the thoracic cord representing transverse myelitis. DISCUSSION Ischemic colitis, acalculous cholecystitis and transverse myelitis have been rarely associated with antiphospholipid syndrome as well as Sjogren’s vasculitis. In previous reports these manifestations have occurred separately in association with antiphospholipid syndrome and Sjogren’s vasculitis, rather than as a cluster complex. We feel our patient likely had both antiphospholipid syndrome and Sjogren’s vasculitis. She did satisfy the International Consensus criteria for probable catastrophic antiphospholipid syndrome as well. CONCLUSION Physicians should consider antiphospholipid syndrome and Sjogren’s vasculitis as well as catastrophic antiphospholipid syndrome in patients with ischemic colitis, acalculous cholecystitis and transverse myelitis. These patients can have a catastrophic rapidly progressive course. Such patients can respond well to anticoagulation and immunosuppressive therapy. HISTORY a. b. Figure 4. MRI of the Thoracic Spine After Treatment a. T2 sagittal image demonstrating normalization of MRI findings after 6 months of treatment. b. T2 axial image demonstrating normalization of MRI findings after 6 months of treatment. Figure 1. Ischemic Colitis Superficial circular ulceration at the splenic flexure consistent with ischemic colitis. Figure 2. Colon Biopsy Focal crypt epithelial necrosis and sloughing, lamina propria hyalinization, crypt epithelial reactive and regenerative changes, and scattered acute inflammatory cells predominantly in the lamina propria. Some thick appearing pseudomembrane-like acute inflammatory exudate. Findings are consistent with ischemic colitis. Figure 3 . Acalculous Cholecystitis Chronic inflammation with edematous thickening of the mucosa.