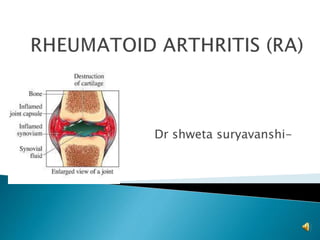
2. RA is a non suppurative, systemic,
inflammatory disease of unknown cause
characterized by polyarthritis of symmetrical
joints and involving the peripheral joints and
extra articular surface
4. Idiopathic
Abnormal immunological reaction
Antigenic agents, which probably act as
predisposing factors, are viruses: rubella,
Epstein-Barr, etc. genetic (common in people
with HLA DR4 60%), psychological stress,
allergic factors, endocrine factors and
metabolic factors.
9. Erosion of articular cartilage
Osteoporotic changes
Joint subluxation and deformity
a
10. Stage I. Inflammation of the synovial membrane spreads
to articular cartilage and other soft tissues. There occurs
limitation of joint movements with pain and muscle
spasm.
Stage II. Granulation tissue formation occurs within the
synovial membrane and spreads to the periarticular
tissues. The cartilage starts disintegrating and the joint is
filled with granulation tissue. There occurs thickening of
the joint capsule, tendons and their sheaths impairing the
joint movement permanently
11. Stage III. The granulation tissue fibrous
tissue adhesion formation between the
tendons, joint capsule and the articular
surfaces. The articular surfaces get partly
covered by cartilage and partly by fibrous
tissue gives rise to contractures and even
ankylosis of the joint, or secondary
osteoarthritis.
12. According to the American College of Rheumatology in 1987
revised criteria, at least 4 out of 7 criteria should be fulfilled
to make a diagnosis of rheumatoid arthritis.
• Morning stiffness for minimum one hour everyday, at
least for six weeks.
• Arthritis or swelling of three or more joints for > 6
weeks.
• Arthritis or swelling of hand joints (wrist, metacarpal)
for more than 6 weeks.
• Symmetrical swelling (arthritis of same joint areas) more
than 6 weeks.
• Serum rheumatoid factor present.
• Radiographic features of RA.
• Rheumatoid nodules.
13. Acute stage –
Joint pain
Swelling
Early morning stiffness
Loss of movements if small joints affected
Tenderness
Warmth and stiffness if large joints affected
14. Chronic stage
Joint deformities
Dislocation of small joints (if affected)
Restricted ROM
Pain and stiffness in cervical spine(if affected)
ADL affected
15.
16. Sub cutaneous nodules
Muscle wasting
Lungs – pleural effusion, bronchitis
Heart – pericarditis, endocarditis and
myocardial diseases
Neuropathies – mononeuritis multiplex
Mouth – dryness of mouth
Kidney and spleen can also be affected
17. Subjective –
Chief complaints:
• Pain in bilateral joints
• Morning stiffness
• Unable to do movements freely
• Difficulty in daily activities
• May complain of neck pain
18. Pain assessment:
• Onset – Gradual
• Site – body chart, UL more common than LL,
peripheral joints> vertebral joints
• Severity – VAS
• Nature – constant, dull aching or sharp
• Aggravating Factors – movements, cold
climate, pressure of clothes
• Relieving Factors – sometimes at rest
19.
20. Level of pain
1. Pain after specific activities
2. Pain during and after activities but it doesn't
affect performance
3. Pain affects performance
4. Pain present in ADL
5. Constant dull aching pain without
disturbing sleep
6. Pain disturbing sleep
25. • Feets – lateral deviation of toes, MT heads
prominent on plantar aspect, hallux valgus,
bunion, pes cavus, claw toes
External appliances – assistive devices, splints
can be present
Skin – papery, shiny and thin
26.
27. On Palpation –
Warmth – may or may not be present
Tenderness – can be present
Effusion – can be present in large joints
Swelling – will be present
28. On examination –
Deformities – will be present, check whether
it is fixed or correctable by passive methods
ROM – will be restricted
Limb length – may or may not be affected
Gait analysis – will be affected – limping gait/
antalgic gait can be present
36. Classification of Functional Capacity for RA
1. Complete functional capacity with ability to
carry on all normal duties
2. Functional capacity adequate to conduct
normal activities despite of discomfort or
limited mobility of one or more joints
3. Functional capacity adequate to perform
only a few or none of the duties of usual
occupation or self care
37. 4. Largely or wholly in capitated. Patient will be
bed ridden or confined to wheel chair,
permitting little or no self care
38. Criteria for diagnosis of RA- any 4 or more
symptoms should be present
1. Early morning stiffness
2. Involvement of more than 3 joints
3. Symmetrical involvement
4. Subcutaneous nodules
5. RH factor positive
6. X ray of hand and wrist involved for 6 weeks
or more
42. Aims-
To relieve pain and muscle spasm
To decrease the acute inflammation
To improve muscle strength
To train patient for independent ambulation
To increase endurance
To prevent and correct deformity
To maintain and improve muscle tone
To improve respiratory and circulatory conditions
To improve ADL
48. Acute or active phase of the disease the acute
symptoms - pain, erythema, tenderness and
swelling - are present.
1. Positioning - of the involved joints and
correct bed posture.
Firm mattress or occasional back support
minimizes the effects of malpositioning and
preserves the integrity of the affected joints.
The limb is positioned in level of minimal
discomfort.
Contracture Prone positions should be
avoided.
49. 2. Splints and sand bags provide
additional support to the limb.
Special attention is needed for the knee and
elbow joints prone to develop flexion
contractures.
The use of casts minimum. The splints or
the casts should be checked regularly to
avoid complications.
50. 3. Deep breathing exercises to improve the
vital capacity.
4. The joints and muscles free from
immobilization and the active disease full
ROM and progressive resistive exercise (PRE).
5. The functional mobility should be
encouraged and maintained.
51. 6. Postural guidance and the methods of
performing activities without putting extra-
strain on the affected joints are taught.
7. In cases with involvement of the weight
bearing joints the upper extremities should
be prepared for future crutch walking.
52. 8.Isometrics: Isometric exercises do not
involve the movements of the joints and are
therefore relatively painless.
Should be started early.
The muscles like quadriceps and deltoid are
susceptible to disuse atrophy and hence need
repeated sessions of isometrics.
The other functional muscles concerned with
weight bearing and body balance need
strengthening and improved endurance.
53. 9. Speedy isometrics to the affected limb in
elevation reduce swelling and effusion
(especially of the knee).
10.No heat therapy should be given to the
joints which are already warm.
11.TENS, pulsed ultrasound for longer
periods offer reduction in the muscle spasm
and pain.
54. 13.Properly guided pool therapy for the
whole body provides an ideal medium for
exercises.
55. 14. Splinting
WHO
Splinting should be given in functional
position of hand – 5-10 degrees of wrist
flexion, 10-20 degrees of MCP flexion and
10-15 degrees of PIP flexion
For swan neck deformity – double ring flexion
splint
For boutonniere deformity – double ring
extension splint
56. Wax therapy – – relieves morning stiffness
HWF – 5-10 mins
Correction of deformity
Patient education by joint protection and
energy conservation techniques
Four Ps
1. Pacing
2. Priority
3. Planning
4. Positioning
57. It is a phase of vigorous activity to train the
patient to use the involved joints to the greatest
extent for physical independence.
By 4-5 weeks of the onset independent sitting by
the use of hands can be started.
If pain permits, active and functional therapeutic
programs should be initiated include standing
and walking.
weight bearing should be deferred till pain and
discomfort subside
58. Before allowing weight bearing it is absolutely
essential to provide the necessary orthotic support or
walking aid to relieve compressive forces on the
affected joints.
This should be done between the parallel bars to
judge the effects of weight bearing on the diseased
joints.
Sustained or intermittent stretching for muscles
which have developed tightness or contractures
during the acute phase.
Deep heat , ultrasound, TENS and other adjuncts may
be used to relieve pain.
59. Efforts should be made to improve the
strength and endurance of the muscles
related to the affected joints.
Job-oriented performance to be imparted in
the exercise regime.
Relapse
Relapse is common RA. It should be treated
on the same lines as detailed for the acute
phase.
Usual sites of contractures and their
prevention
Since it is a systemic disease, it is usually
accompanied by early fatigue. Therefore,
exercise sessions should be brief.
60.
61.
62.
63.
64.
65. The prognosis of the disease is very much
unpredictable. There may be:
(a) Partial or total remission;
(b) Remaining as a mild disease;
(c) Insidious progressive in nature;
(d) Progressive, but the progress of the
disease may be (i) rapid (ii) slow or (iii)
intermediate.
66. Synovectomy
Soft tissue release
Osteotomy
Arthroplasty
Arthrodesis
Tendon repair or transfer
Editor's Notes
Wind swept – one knee in severe valgus and another in severe valgus