
Recommended
More Related Content
Similar to Management lipids.pptx
Similar to Management lipids.pptx (20)
Recently uploaded
Recently uploaded (20)
Management lipids.pptx
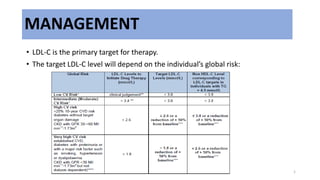
- 1. MANAGEMENT • LDL-C is the primary target for therapy. • The target LDL-C level will depend on the individual’s global risk: 1
- 2. TYPE OF MANAGEMENT THERAPEUTIC LIFESTYLE CHANGES 1) Dietary modification 2) Weight reduction 3) Regular physical activity 4) Cessation of smoking 5) Alcohol restriction DRUG THERAPY Lipid lowering drugs: a) Statin b) Fibrates c) Resins d) Niasin e) Cholesterol Absorption Inhibitors f) PCSK 9 inhibitors LDL-C APHERESIS
- 3. STATINS HMG CoA reductase inhibitor (rate limiting enzyme in hepatic cholesterol synthesis) Treatment of choice in reducing LDL-C Suitable first-line agents in familial hypercholesterolemia, for primary prevention of CVD, secondary prevention of CVD and CHD equivalents Starting dose with the evening meal or at bed time (except for long-acting statins that can be taken at any time) Serum lipids and alanine aminotransferase(ALT) should be measured at 6-8 weeks Contraindicated in pregnancy and lactation Adverse effects Liver function (elevation of ALT) Muscle symptoms (myalgia, myositis, rhabdomyolisis) Diabetes( new onset) Kidney problem (proteinuria) Neurocognitive function ( memory loss and confusion) 3
- 5. Fibrates (Fibric acid derivatives) Peroxisome Proliferator Activated Receptor (PPAR) –α agonist which in turn stimulates synthesis of fatty acid oxidation Reduce TG levels and increase HDL-C levels effectively Useful in individuals with combined (mixed) dyslipidaemia and hypertriglyceridaemia Alternatives for mild to moderate hypercholesterolaemia that has Statin intolerance Doses adjusted in patients with CKD 5
- 7. Resins Bile acid sequestrants bind to bile acids to promote their secretion into the intestines -- effective in lowering LDL-C May increase TG and HDL-C slightly Other medications should be taken 1 hour before and/or 4 hours after resins 7
- 8. Niacin (Nicotinic acid) Decrease mobilization of free fatty acids from adipose tissues Very effective in increasing HDL-C and lower both TC and TG levels Its side effects (particularly flushing and gastrointestinal side effects) tend to limit compliance 8
- 9. Cholesterol Absorption Inhibitors Selectively block intestinal absorption of both dietary and biliary cholesterols and other phytosterols -- reduction in hepatic cholesterol delivery Indicated as monotherapy for primary hypercholesterolemia patients who cannot tolerate statin or fibrate Used also in combination with statins to further lower LDL-C 9
- 10. PCSK9 inhibitors This is a new class of lipid-lowering drug that target the proprotein convertase subtilisin kexin type 9 (PCSK9). MOA by inhibiting the binding of PCSK9 to the LDL-receptors. Hence, it decreases the degradation of the LDL-receptors resulting in higher LDL-receptors causing an increased clearance with resulting decrease in LDL-C levels. Indication: individuals with high CV risk who have persistently elevated LDL-C despite optimum lipid- modifying therapy those with familial hypercholesterolemia – heterozygous FH and to a lesser extent those with homozygous FH Very High Risk and High-Risk patients with true statin intolerance and persistently high levels of LDL-C may also be candidates for PCSK9 inhibitors Recommended Dose: • Dose of evolocumab: 140 mg SC every two weeks or 420 mg SC monthly • Dose of alirocumab: 75-150 mg SC every two weeks
- 11. Summary of anti-lipid drugs
- 12. RECOMMENDED DRUG TREATMENT • If target lipid goals have not been achieved after 8-12 weeks of optimal monotherapy, combination therapy is suggested • Statin + Cholesterol absorption inhibitors ~ reduce CV events and renal outcomes in patients with CKD • Fibrates + Statins ~ potentially adverse effects especially myositis (incidence : 0.5-2.5%)
- 13. MONITORING AND THERAPY DURATION • After starting drug therapy, LDL-C level should be measured at 6-8 weeks • Drug doses titrated if necessary • Once target lipid levels are achieved, a 4-6 monthly follow up is recommended
- 14. Monitoring of ALT is necessary if statins and fibrates are used for treatment • Liver function tests should be carried out before and within 1-3 months of starting treatment • Statin is discontinued if ALT levels rise to at 3x upper limit of normal • If the levels are elevated between 2 to 3 times upper limit of normal, the trend should be monitored at monthly intervals • If myositis is suspected, then creatinine kinase levels should be measured. If the level is more than 10 times the upper limit of normal, then the drug should be discontinued
- 15. Pharmacoeconomics of Lipid Lowering Therapy LDL-C apheresis • indicated in patients with homozygous familial hypercholesterolemia (FH) who do not respond satisfactorily to maximum multiple drug therapy (high intensity statin at maximal dose with ezetimibe/PCSK9)