
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Hydrocele by tlali
Semelhante a Hydrocele by tlali (20)
Último
Último (20)
Hydrocele by tlali
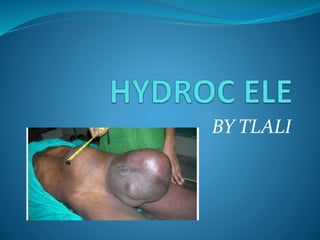
- 1. BY TLALI
- 3. WHAT IS HYDROCELE A hydrocele is a collection of fluid in the scrotum. OR A hydrocele is a collection of fluid in a sac in your scrotum next to a testicle (testis). It usually occurs on one side but sometimes a hydrocele forms over both testicles (testes).
- 5. PATHOPHYSIOLOGY The normal testis is surrounded by a smooth protective tissue sac. You cannot normally feel this. It makes a small amount of 'lubricating' fluid to allow the testis to move freely. Excess fluid normally drains away into the veins in your scrotum. If the balance is altered between the amount of fluid that is made and the amount that is drained, some fluid accumulates as a hydrocele.
- 6. In infants it is usually the result of incomplete closure of the processus vaginalis.
- 7. CAUSES AND PREDISPOSING FACTORS Most hydroceles are present at birth (congenital), and babies who are born prematurely have a higher risk of having a hydrocele. Incidence : 3.5 to 5.0% in full term infants and 44 to 55% in premature and Low birth weight babies (Groff D, Nagaraj HS, Pietsch JB, Inguinal hernias in premature infants who were operated on before their discharge from the neonatal intensive care unit Arch Surgery 1985)
- 8. Risk factors for developing a hydrocele later in life include: Scrotal injury (Traumatic/Iatrogenic), Infection including sexually transmitted infections, Tumours.
- 9. EXCESS ALCOHOL USE OR ABUSE
- 10. CLINICAL PRESENTATION In the early stages hydroceles are usually asymptomatic. As they enlarge they bulge out and can become a cosmetic problem. Symptoms can develop, as the swelling increases in size, which include: Heaviness, fullness, or dragging sensations due to an enlarged scrotum. There may be mild discomfort radiating along the inguinal area to the mid portion of
- 11. If pain develops in a Hydrocele it is usually an indication of acute epididymal infection or due to overstretched scrotal skin in huge hydroceles. The size may decrease with recumbency or increase in the upright position. Fever, chills, nausea, or vomiting indicate an infection of a hydrocele.
- 12. DIAGNOSTIC TECHNIQUES AND LAB TESTS
- 13. PHYSICAL ASSESSMENT Smooth, cystic mass completely surrounding the testis and not involving the spermatic cord(Possible to get above the swelling) is characteristic of a hydrocele. The consistency of hydroceles can vary with position. Sometimes a hydrocele can become smaller and softer on lying down and become larger and tenser after prolonged standing. Getting above the Swelling
- 14. TESTIS MAY BE PALPABLE SOFT,FLUCTUANT, MAYBE TENSE IN CASE OF FILARIAL SCROTUM CAN GET ABOVE SWELLING
- 15. TRANSLLUMINATION When the fluid in the hydrocele is clear, Transillumination is positive. Transillumination may be negative in filarial hydrocele due to prescence of chyle, calcification or in complicated hematocele/pyocele
- 16. LAB TESTING Laboratory evaluation is generally not essential to the evaluation of hydroceles. Leukocytosis with a higher percentage of neutrophils suggests an infectious and/or inflammatory process (eg, epididymo-orchitis).
- 17. IMAGING STUDIES Uncomplicated hydroceles do not require radiographic studies. Findings from USG can help evaluate for an underlying process, such as a tumour or torsion.
- 18. DIFFRENTIAL DIAGNOSIS Hydroceles are generally painless. The presence of pain, redness and edema with loss of the normal scrotal rugae is suggestive of an inflammatory lesion like epididymitis or epididymo-orchitis or filarial relapses.
- 19. MEDICAL MANAGEMENT In infancy, Hydrocele usually resolves spontaneously by the time the child reaches the age of 1 year. A hydrocele that persists longer than 12 to 18 months is usually requires Herniotomy In Adults, Treatment depends upon the age of the patient and the degree of discomfort caused by the hydrocele. Surgical excision forms the definitive therapy for hydroceles. When they are small and asymptomatic, hydroceles require no treatment other than reassurance.
- 20. Surgical intervention Indications for surgery – Scrotal discomfort or pain Cosmetic - disfigurement due to the sheer size of the hydrocele.
- 21. Techniques include – LORDS PLICATION used for small to medium hydroceles with thin sac. Benefits - reduced risk of hematoma.. Some articles suggest a slight incidence of recurrence of the hydrocele following this procedure. JABOULEYS OPERATION the sac & everted and sutured behind the testis, associated with a reduced risk of recurrence, may have an increased risk of hematoma. SUBTOTAL EXCISION or HYDROCELECTOMY In cases of large sac, where there is risk of a large redundant swelling post operatively, excision of the sac with 1 cm margin around the testis & epididymis. ?Filarial Sac SHARMA & JHAWERS TECHNIQUE ASPIRATION WITH/WITHOUT INJECTION OF SCLEROSING AGENT HERNIOTOMY.
- 22. INJURY TO VAS DEFERENS INJURY TO URETHRA INJURY TO TESTIS/EPIDIDYMIS REACTIONARY HAEMORRHAGE INFECTION SINUS FORMATION RECURRENT HYDROCELE COMPLICATIONS OF SURGERY
- 23. PHARMACOLOGICAL HELP No pharmacological management directed directly to Hydrocele, But can be indicated towards problems arising However ANTIBIOTIC THERAPY IS NECESSARY specifically Pre – and Post-surgical invasion
- 24. NURSING DIAGNOSIS TO BE DISCUSSED WITH THE COLLEGUES
- 25. NURSING MANAGEMENT TO BE DISCUSSED WITH THE CLASS
- 26. 1. INFECTION 2. PYOCELE,HEMATOCELE/CLOTTED HEMATOCELE 3. CALCIFICATION OF SAC (D/D FOR TESTICULAR TUMOUR) 4. INFERTILITY 5. ATROPHY OF TESTIS 6. HERNIATION OF HYDROCELE SAC (rare) 7. RUPTURE (rare) COMPLICATIONS OF HYDROCELE