Novel tools for immune quiecense monitoring in kidney transplanation poster abstract 14 wtc-2376-roedder et al._.pdf
•Download as PPT, PDF•
2 likes•297 views

Organ transplant patients face life-long immunosuppression (IS) with increased morbidity. Currently unknown numbers of kidney transplant recipients develop a state of targeted immune quiescence (Operational Tolerance, TOL) allowing them to withdraw IS while retaining stable graft function and continuing immune responses against 3rd party antigens. Transcriptional Profiling Peripheral Blood is a means to provide a gene signature to monitor this state of TOL, to titrate IS in patients with this signature, and to better understand the underlying biology.
Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Novel tools for immune quiecense monitoring in kidney transplanation poster abstract 14 wtc-2376-roedder et al._.pdf
Similar to Novel tools for immune quiecense monitoring in kidney transplanation poster abstract 14 wtc-2376-roedder et al._.pdf (20)
More from Kevin Jaglinski
More from Kevin Jaglinski (14)
Recently uploaded
Recently uploaded (20)
Novel tools for immune quiecense monitoring in kidney transplanation poster abstract 14 wtc-2376-roedder et al._.pdf
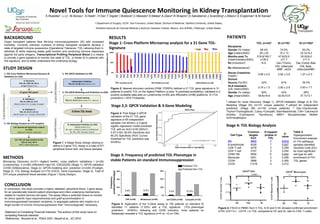
- 1. Novel Tools for Immune Quiescence Monitoring in Kidney Transplantation S.Roedder1 , L.Li2 , M.Alonso2 , S.Hsieh1 , H.Dai1 ,T.Sigdel1 ,I.Bostock3 ,C.Macedo4 ,D.Metes4 ,A.Zeevi4 ,R.Shapiro4 ,O.Salvatierra2 ,J.Scandling2 ,J.Alberu3 ,E.Engleman2 & M.Sarwal1 1 Department of Surgery, UCSF, San Francisco, United States; 2School of Medicine, Stanford University, United States; 3Instituto Nacional de Ciencias Medicas y Nutricion Salvador Zubiran, Mexico, and 4UPMC, Pittsburgh, United States. Table 1 BACKGROUND Organ transplant patients face life-long immunosuppression (IS) with increased morbidity. Currently unknown numbers of kidney transplant recipients develop a state of targeted immune quiescence (Operational Tolerance, TOL) allowing them to withdraw IS while retaining stable graft function and continuing immune responses against 3rd party antigens. Transcriptional Profiling Peripheral Blood is a means to provide a gene signature to monitor this state of TOL, to titrate IS in patients with this signature, and to better understand the underlying biology. STUDY DESIGN Figure 1: 4-Stage Study Design utilizing to define a 3-gene TOL Assay in a total of 571 peripheral blood-/cell- and tissue samples. Cell-Type Common targets fc≥3 # mapped probes in TOL p- value DC 3922 7 0.013 B-lymphocyte 5028 7 0.047 CD8+ T-cell 3278 3 0.259 CD4+ T-cell 3157 3 0.254 CD56+ NK 3802 6 0.042 Monocyte 3241 3 0.258 CD34+ 3898 3 0.265 CD33+ 11218 4 0.212 Figure 4: FACS in PBMC from 5 TOL, 6 SI and 5 HC showed confirmed enrichment of DC (CD11c+, CD14lo ) in TOL compared to HC and SI; ratio to CD4- T-cells) Stage 4: TOL Biology Analysis METHODS Microarray Discovery (n=31) (Agilent 4x44k), cross platform validations I (n=29) (Lymphochip), II (n=58) (Affymetrix HgU133, GSE22229) (Stage 1); QPCR-validation (n=59) (SABioscience, Stage 2); QPCR-modeling and- prediction (n=220) (Fluidigm, Stage 3); TOL Biology Analysis (n=174) (FACS, Gene Expression, Stage 4). Total of 574 unique peripheral blood samples (Figure 1 Study Design). Figure 3: Post Stage 2 QPCR validation of the 21 TOL gene signature in 65 independent samples (not shown), a 3-gene logistic regression model predicted TOL with an AUC=0.95 (95%CI: 0.97-0.92); 84.6% Sensitivity and 90.2% Specificity (ROC Curve); threshold for TOL prediction was Θ=25%) Stage 2,3: QPCR Validation & 3-Gene Modeling TOL (n=43)A SI (n=78)A SI (n=150)B Recipients Gender (% males) 68.4% 74.0% 63.3% Age (mean±StdD) 28 ± 20 15 ± 13 33.3±19.2 Months post Tx (mean/median±StdD) 216.8/195.7 ±139.2 47.6/23.5 ±71.7 25.5/29.0 ±11.4 Rx (Induction)C N.A. Dac./Thymo. Dac./Camp./Bas. Rx (Maintenance)C - CNI, ±Steroids/ MMF, ±AZA CNI, Bela., ±Steroids/MMF Serum Creatinine (mg/dL) 0.95 ± 0.2 2.92 ± 2.9 1.27 ± 0.3 Donors Source (%LRD) 32% 67% 59.3% HLA mismatch (x/6; mean±StdD) 0.75 ± 1.5 2.92 ± 2.9 2.93 ± 1.7 Gender (% males) 50% 42% 48% Age (mean±StdD) 39.8±16.6 42.9±10.8 37.7±13.1 PATIENTS A utilized for novel Discovery (Stage 1), QPCR-Validation (Stage 2) & TOL Modeling (Stage 3A) (n=121 unique patients); B utilized for independent prediction (Stage 3B) (n=150 unique patients); C Dac.=Daclizumab, Thymo=Thymoglobulin, Camp.=Campath, Bas=Basiliximab, CNI= Calcineurin Inhibitor (Cyclosporin, Tacrolimus); MMF= Mycophenolate Mofetil; AZA=Azathioprin Stage 3: Frequency of predicted TOL Phenotype in stable Patients on standard Immunosuppression Figure 3: Application of the 3-Gene assay to 150 patients on standard IS identified 11 patients (7.33%) with a TOL signature (TOL-phenotype prediction Θ=60%); following anti CD25 induction, more patients on Belatacept revealed a TOL signature (n=5 vs. =2 on CNI). 60% 40% 20% 0% 60% 40% 20% 0% Frequency predictedPhenotype Predicted TOL Predicted Non-TOL CONCLUSION In conclusion, this study provides a highly validated, peripheral blood, 3 gene assay for an operationally tolerant patient phenotype and infers underlying mechanisms related to myeloid derived cell types. The assay offers a potential means to monitor for donor specific hypo responsiveness and graft accommodation in immunosuppressed transplant recipients, to segregate patients who maybe on a larger burden of chronic immunosuppression than “immunologically” necessary. Statement of Competing Financial Interests: The authors of this study have no competing financial interests; References.: Brouard et al., PNAS 2007, Newell et al., JCI 2010 Figure 2: Nearest shrunken centroid (PAM, FDR5%) defined a 21 TOL gene signature in 31 patients to predict TOL on the Agilent Platform (y-axis: % predicted probability); validated in 2 publicly available data-sets on Lymphochip (n=29) and Affymetrix (n=58) platforms. Θ (TOL prediction) = 50% Probability . RESULTS Stage 1: Cross Platform Microarray analysis for a 21 Gene TOL- Signature Table 2: Hypergeometric Enrichment analysis of 174 cell/tissue samples identified Dendritic Cells (DC) as most significant cell type for with enrichment of 7/21 TOL genes