Adrenal gland diseases,Cushing syndrome,Addison disease and Pheochromocytoma
1. ADRENAL GLAND DISEASES
Cushing syndrome
Addison disease
Pheochromocytoma
Presented by Jonathan Chikomele R,MD5
Supervised by Dr Paul Mwanyika, MD,Mmed-Ped.
Mbeya Zonal Referral Hospital
Tanzania
May 2018
2. The adrenal glands are the pair
endocrine gland, located above the
superior kidneys' poles. They are
against the interspace between the
first lumbar vertebra and eleventh
thoracic vertebra. They have triangular
form.
The weight of both adrenal glands is
6 to 12 g, the length is 4-6 cm, the
width is 2-3 cm, and the thickness is to
1 cm.
The external portion of the adrenal
gland is surrounded by the connective
tissue capsule.
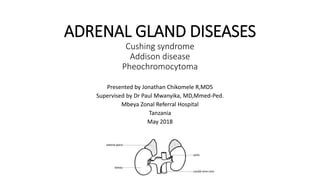
The adrenal gland consists of outer
cortex and an inner adrenal medulla.
Cortical substance
Medullary
substance
3. The adrenal cortex forms
three layers:
The zona glomerulosa
(external),
zona fasciculata, located in
the middle of these layers,
and zona reticularis,
adjoining to the adrenal
medulla.
1- capsule,
2- cortical substance
(а- zona glomerulosa,
б- zona fasciculata, в- zona reticularis),
3- medullary substance.
8. CUSHING SYNDROME
Definition
• Cushing’s syndrome: constellation of symptoms associated with
cortisol excess.
• Cushing's syndrome develops when the level of a glucocorticoid in the
body is too high over a long period of time.
• Too much glucocorticoid can occur from an exogenous or endogenous
source
• described by Harvey Cushing in 1932
12. Clinical presentations
Findings are more obvious in infants
• Children with adrenal tumors
Signs of abnormal masculinization
• Growth impairment
Short stature
• Decreased collagen cause purplish striae on soft tissues of the body
• They are prone to infections due to compromised immune system
• Decreased linear growth
13.
14.
15.
16.
17.
18. Diagnosis of Cushing’s Syndrome
• Obtain a careful history to exclude exogenous glucocorticoid use.
• Perform at least two first-line biochemical tests to obtain the
diagnosis:
• Urine free cortisol (UFC) (at least two measurements)
• Late-night salivary cortisol (two measurements)
• In +ve tests Morning and midnight plasma cortisol levels are elevated
• Serum ACTH level
• Bloods tests – which and why?
• FBC
• U/E – low K
19. Diagnosis
• Cortisol levels in blood are normally elevated at 8 A.M. and decrease
to less than 50% by midnight except in infants and young children in
whom a diurnal rhythm is not always established.
• In patients with Cushing syndrome this circadian rhythm is lost, and
cortisol levels at midnight and 8 A.M. are usually comparable.
• Urinary excretion of free cortisol is increased. This is best measured
in a 24-hr urine sample and is expressed as a ratio of micrograms of
cortisol excreted per gram of creatinine
20. Dexamethasone suppression test
• Dexamethasone is an exogenous steroid that provides negative feedback
to the pituitary to suppress the secretion of ACTH.
• This steroid is unable to pass the blood brain barrier which allows this
test to assess a specific part of the hypothalamicpituitary-adrenal axis.
Specifically, dexamethasone binds to glucocorticoid receptors in the
pituitary gland, which lies outside the blood brain barrier, resulting in
regulatory modulation
• A single-dose dexamethasone suppression test is often helpful a dose
of 25–30 μg/kg (maximum of 2 mg) given at 11 P.M. results in a plasma
cortisol level of less than 5 μg/dL at 8 A.M. the next morning in normal
individuals but not in patients with Cushing syndrome.
• A low dose dexamethasone suppresses cortisol in individuals with no
pathology in endogenous cortisol production. A high dose
dexamethasone exerts negative feedback on pituitary ACTH producing
cells but not on ectopic ACTH producing cells or adrenal adenoma.
21. Low-dose
• A normal result is decrease in cortisol levels upon administration of low-
dose dexamethasone.
• Cushing's disease involve no change in cortisol on low-dose
dexamethasone, but inhibition of cortisol on high-dose dexamethasone
Large dose DX suppression test
• D.X 2mg q6h P.O 2 days Urinary free cortisol reduced 50%: Cushing’s
disease (Pituitary adenoma)
• Urinary free cortisol NOT reduced 50%:Adrenal tumor, carcinoma, ectopic
ACTH Syndrome
23. • Dx of Cushing syndrome has been established then,the next step is to
find out the cause
↓
Serum ACTH level
• If low or undetectable– ACTH independent cause [Adrenal cause
likely]
• If high– Cushing’s disease or Ectopic ACTH syndrome
• Two differentiate between these two: High dose DST is to be done
24. High dose DST
• 2 mg 6 hrly for 2 days
• Cortisol level measured at 8 AM on Day 0 and Day 2
• Partial suppression of cortisol (>50%) confirms Pituitary cause
(Cushing disease)
• Failure to suppress suggest Ectopic ACTH syndrome
28. Medical therapy
Purpose
• Correct metabolic abnormalities before attempted surgical cure
• Palliate surgically non curable disease
• Achieve remission in patients for whom surgery is unlikely to achieve
satisfactory long term results
30. Surgical tx
Cushing’s disease
◦ Trans sphenoidal microadenomectomy
◦ Pituitary radiation
◦ Bilateral total adrenolectomy
Adrenal adenoma and carcinoma
◦ Surgical removal
Ectopic ACTH Syndrome
◦ Surgical removal of the ectopic tumor
◦ Radiotherapy
31. Adrenal Insufficiency
• Primary Adrenal Insufficiency is also known as Addison’s Disease in
honor of Dr. Thomas Addison
• Dr. Addison is also credited with the discovery of Pernicious Anemia
• Addison's diseaseis serious chronic disease, caused by partial or
absolute abnormality of hormonal function of the adrenal cortex due
to its two-sided disorder (first it was described by Tomas Addison in
1855).
32. Epidemiology
• Addison’s disease is a rare and chronic disease.
6-110 cases diagnosed per 100,000 in the world per year.
1.4 million deaths per year around the world.
Usually effects 30-50 year-olds, but can be seen in all ages.
33. Adrenal Insufficiency
• Arises when cortisol levels are not sufficient to meet the needs of the
body
• May be primary or secondary
• May be congenital or acquired
• It develops at the age of 20-40 years old
• Can be fatal if left untreated
36. Etiology
• Most commonly is of an autoimmune etiology, resulting from chronic
destruction of the adrenal cortex
• Typical histologic feature is lymphocytic infiltration
• Antibodies to adrenal cortical antigens are present early in the disease
process
• Patients with autoimmune adrenal disease are more likely to have
polyglandular autoimmune systems causing deficiency of other
endocrine glands
37. Cont..
• Several Other Mechanisms Exist:
• Bilateral adrenal hemorrhage
• Infection: Tuberculosis, CMV, Histoplasmosis,syphylis
• Metastatic Disease
• Deposition Diseases: Hemochromatosis, Amyloidosis, Sarcoidosis
• Drug Induced: Ketoconazole, Etomidate, Rifampin, Anticonvulsants
• Congenital Adrenal Hyperplasias
idiopathic atrophy of adrenal cortex (antigens to mitochondrion
and microsomal fraction);
adrenal glands hemorrhage;
38. Secondary Adrenal Insufficiency
• Caused by pituitary failure of ACTH secretion
• Etiologies include:
• any cause of primary or secondary hypopituitarism
• Exogenous Glucocorticoid Therapy
• Megestrol, which has some glucocorticoid therapy
39. The pathogenesis
The deficiency of clucocorticoids leads to adynamia, the
cardiovascular and gastrointestinal disorders:
the sugar level in the blood is decreased;
the development of eosinophilia, leukocytosis, and
granulopenia;
hyponatremia, hypochloremia, hyperkaliemia, which lead to
dehydration and hypotonia;
the decreasing of sex hormones production leads to the
impotence in male, or the menstrual cycle disorder in female;
the bronze color of the skin is caused by the melanin pigment
deposit in the papillary layer of the dermis and mucous
membranes.
40. Clinical Presentation
• Symptoms may include weakness, weight loss,
nausea, vomiting, anorexia, and postural
hypotension,Hyperpigmentation,Hypotension,O
rthostatic changes,Weak pulses,Shock
• Loss of axillary/pubic hair (women)
• Increased skin pigmentation can be seen with
primary adrenal insufficiency secondary to
melanocyte stimulating activity associated with
ACTH
• Hyponatremia and Hyperkalemia may develop
secondary to a lack of aldosterone
41. LABORATORY DIAGNOSTICS
In the blood analysis: lymphocytosis, eosinophilia, erythrocyte
sedimentation rate is decreased, when the active tuberculosis
is present this rate is increased;
The electrolyte: hyponatremia, hypochloremia, hyperkaliemia;
Baseline Cortisol and ACTH levels should be obtained in the
early morning
The content of ACTH is increased;
The content of cortisol is decreased;
The concentration of glucose in the blood is decreased;
The glucose tolerance test – flat with marked hypoglycemic
phase in three hours;
The potassium flow with urine is decreased, the natrium and
chlorine flow is increased.
43. Treatment
• Replacement ( always need glucocorticoids and usually mineralcorticoid
therapy)
• Hydrocortison orally 15 mg at morning and 5 mg at evening
• Doses change according to lifestyle:
- doubling the routine oral dose in the case of intercurrent illness
with fever
- IV hydrocortisone injection at a daily dose of 100 mg in cases of prolonged
vomiting, surgery, or trauma
• Have to carry emergency injection of hydrocortisone and card/bracelet
indentifying their condition
44. Cont..
• Mineralocorticoid replacement in primary AI (100–150 g fludrocortisone). The
adequacy of treatment can be evaluated by measuring BP, sitting and standing
to detect a postural drop indicative of hypovolemia, serum Na, k, and plasma
renin should be measured regularly.
• Adrenal androgen replacement is an option in patients with lack of energy, and
in women with loss of libido.
- It can be achieved by once-daily administration of 25–50 mg DHEA. Treatment
is monitored by measurement of DHEAS, androstenedione, testosterone.
45. Treatment
Special precautions
• During intercurrent illness,trauma,surgery, esp in fever, the dose of
hydrocortisone should be doubled
• Increase the dose of fludrocortisone and to add salt in strenuous
exercise with sweating, extremely hot weather, gastrointestinal upsets
such as diarrhea
•Pts receiving long term steroid therapy have two deficits
1.adrenal atrophy secondary to the loss of endogenous ACTH
2.failure of pituitary ACTH release have low blood cortisol, ACTH levels,
and abnormal ACTH stimulation test
46. Complications
• Gastritis
• hypokalemia,
• sodium retention lead to hypertension,cardiac enlargement, and
even congestive heart failure
• So Periodic measurements of body weight,serum potassium level,
and blood pressure
47. ADDSONIAN CRISIS
• Addisonian Crisis:
• Severely low blood pressure (shock)
• Hyperkalemia
• Hyponatremia
• Hypoglycemia
• Hypercalcemia
• Unexplained fever, diarrhea, vomiting
• Coma and death
• Precipitated by infection, surgery or intercurrent disease
48. Management
• It is a medical emergency
• IV fluid (normal saline 1 L/h with continuous cardiac monitoring
and 10% dextrose)
• Hydrocortisone 100 mg bolus followed by 100–200 mg
hydrocortisone over 24 h infusion or i.v doses until GI symptoms
improve then start oral therapy
• Mineralocorticoid replacement can be initiated once the daily
hydrocortisone dose has been reduced to <50 mg
• Treat precipitating cause
49. Pheochromocytoma
• Is a are neuroendocrine tumor of the medulla of the adrenal glands
(originating in the chromaffin cells), or extra-adrenal chromaffin
tissue that secretes excessive amounts of Catecholomines
(epinephrine and norepinephrine) --hormones that regulate heart
rate and bloodpressure
50. • May occur as a single tumor or as more than one growth. It usually
develops in the center (medulla) of one or both adrenal glands.
• Sometimes this kind of tumor occurs outside the adrenal gland but
90% are in the adrenal glands .The extramedulary sites are;
• Within the sympathetic nervechain along the spinal cord
• Overlying the distal aorta
• Within the ureter
• Within the urinary bladder
51. Factors associated with pheochromocytoma
include
• A family history of pheochromocytoma
• Tumors in other glands of the body
• Other hormonal disorders
• Genetic diseases including:
Von Hippel-Lindau disease
Multiple endocrine neoplasia type 2
Neurofibromatosis type 1
Paraganglioma syndromes
60. Prognosis
• •1/3 Patients continue to be hypertensive:
1)Not all tissue removed
2)Recurrence
3)Blood vessels damaged by severe & prolonged hypertension
•The tumors come back in less than 10% of these patients.
• Release of the hormones norepinephrine and epinephrine returns
to normal after surgery.
•Less than 50% of patients who have cancerous tumors that spread
to the bones, liver, or lung are alive after 5 years.
61. Assessments
• Blood sugar
- Hypoglycemia (after surgery)
- Hyperglycemia (before and during surgery)
• Blood pressure
- Hypertension (before and during surgery)
- Hypotension (after surgery)
LDDST: increased specificity than other screening tests.
All initial screening tests have good sensitivity but poor specificity. Therefore risk of false positive results.
DST: Dexamethasone Suppression test
Physiologic causes: see slide 6