
Recommended
More Related Content
Similar to FROM THE ACADEMYSkin cancer and photoprotection in people of
Similar to FROM THE ACADEMYSkin cancer and photoprotection in people of (20)
More from JeanmarieColbert3
More from JeanmarieColbert3 (20)
Recently uploaded
Recently uploaded (20)
FROM THE ACADEMYSkin cancer and photoprotection in people of
- 1. FROM THE ACADEMY Skin cancer and photoprotection in people of color: A review and recommendations for physicians and the public Oma N. Agbai, MD, a Kesha Buster, MD, b Miguel Sanchez, MD, c Claudia Hernandez, MD, d Roopal V. Kundu, MD, e Melvin Chiu, MD, f Wendy E. Roberts, MD, g Zoe D. Draelos, MD, h Reva Bhushan, PhD, i
- 2. Susan C. Taylor, MD, j and Henry W. Lim, MD a Detroit, Michigan; Wichita, Kansas; New York, New York; Chicago and Schaumburg, Illinois; Los Angeles and Rancho Mirage, California; High Point, North Carolina; and Philadelphia, Pennsylvania From D D D m C D M C Ra A H
- 3. 748 Skin cancer is less prevalent in people of color than in the white population. However, when skin cancer occurs in non-whites, it often presents at a more advanced stage, and thus the prognosis is worse compared with white patients. The increased morbidity and mortality associated with skin cancer in patients of color compared with white patients may be because of the lack of awareness, diagnoses at a more advanced stage, and socioeconomic factors such as access to care barriers. Physician promotion of skin cancer prevention strategies for all patients, regardless of ethnic background and socioeconomic status, can lead to timely diagnosis and treatment. Public education campaigns should be expanded to target communities of color to promote self-skin examination and stress importance of photoprotection, avoidance of tanning bed use, and early skin cancer detection and treatment. These measures should result in reduction or earlier detection of cutaneous malignancies in all communities. Furthermore, promotion of photoprotection practices may reduce other adverse effects of ultraviolet exposure including photoaging and ultraviolet- related disorders of pigmentation. ( J Am Acad Dermatol 2014;70:748-62.) Key words: basal cell carcinoma; Bowen disease; dermatofibrosarcoma protuberans; dyspigmentation; melanoma; Merkel cell carcinoma; mycosis fungoides; people of color; photoprotection; radiation; skin cancer; skin of color; squamous cell carcinoma; sun protection; sunscreen; ultraviolet. DEFINITIONS Abbreviations used:
- 4. BCC: basal cell carcinoma DFSP: dermatofibrosarcoma protuberans MED: minimal erythema dose MF: mycosis fungoides MM: malignant melanoma NMSC: nonmelanoma skin cancer POC: people of color SCC: squamous cell carcinoma SEER: Surveillance, Epidemiology, and End Results SPF: sun-protection factor UV: ultraviolet Whites: Non-Hispanic individuals of European descent Blacks: Non-Hispanic individuals of African descent Hispanics: Individuals who trace their origin or descent to Mexico, Puerto Rico, Cuba, Spanish- speaking Central and South American countries, Spanish-speaking island nations of the Caribbean, and other Spanish cultures. Origin can be considered as the heritage, nationality group, lineage, or country of the person or the person’s parents or ancestors before their arrival in the United States. People who the Multicultural Dermatology Center, Department of ermatology, Henry Ford Hospital, Detroit a ; Department of ermatology, Via Christi Clinic, Wichita b
- 5. ; Department of ermatology, New York University Medical Centerc; Depart- ent of Dermatology, University of Illinois College of Medicine, hicago d ; Northwestern Center for Ethnic Skin, Department of ermatology, Northwestern University Feinberg School of edicine, Chicagoe; Division of Dermatology, University of alifornia Los Angeles Medical Centerf; Desert Dermatology ncho Mirage g ; Dermatology Consulting Services, High Point h ; merican Academy of Dermatology, Schaumburgi; and Society ill Dermatology and Cosmetic Center, Philadelphia.j Funding sources: None. The authors’ conflict of interest/disclosure statements appear at the end of the article. Accepted for publication November 26, 2013. Reprint requests: Reva Bhushan, PhD, Department of
- 6. Evidence-based Research, American Academy of Dermatology, 930 E Woodfield Rd, Schaumburg, IL 60173. E-mail: [email protected] Published online January 30, 2014. 0190-9622/$36.00 � 2014 by the American Academy of Dermatology, Inc. http://dx.doi.org/10.1016/j.jaad.2013.11.038 Delta:1_given name Delta:1_surname Delta:1_given name Delta:1_surname Delta:1_given name Delta:1_surname Delta:1_given name Delta:1_surname Delta:1_given name Delta:1_surname Delta:1_given name mailto:[email protected] http://dx.doi.org/10.1016/j.jaad.2013.11.038 J AM ACAD DERMATOL VOLUME 70, NUMBER 4 Agbai et al 749 identify their origin as Hispanic or Latino may be of any race. This definition of Hispanic fully excludes the Portuguese, Brazilians, or anyone from any other country that speaks Portuguese.1
- 7. Asians: Individuals having origins in any of the original peoples of East Asia, Southeast Asia, or the Indian subcontinent, including, for example, Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam.1 INTRODUCTION Malignant melanoma (MM) and nonmelanoma skin cancer (NMSC) account for 40% of all neoplasms in whites, making it the most common malignancy in the United States.2 Skin cancer is most common in whites and in people living in equatorial latitudes.3 The incidence of both MM and NMSC remains significantly lower in people of color (POC) when compared with whites as they are seen in about 5% of Hispanics, 4% of Asians, and 2% of blacks.4,5 Even so, multiple reports have demonstrated heightened morbidity and mortality in minority populations, 6-8 raising public health concerns in these groups. Although there are data detailing incidence of skin cancer in POC, these data are limited. In addition to skin cancer, factors such as photoaging, pigmentary disorders induced or exacerbated by ultraviolet (UV) exposure, and sunburn must be considered in POC. It is estimated that black, Hispanic, and Asian Americans will comprise approximately 50% of the US population by the year 2050.4 These evolving demographics, elevated rates of skin cancer morbidity and mortality in POC, and limited clinical
- 8. data on additional adverse effects of UV exposure in this population mandate that physicians develop familiarity with the concept of optimized photo- protection for POC. An understanding of the varying clinical presentations of UV-related skin cancers in POC, in addition to relevant topics in photoaging and UV-related disorders of pigmentation, is necessary for adequate management of photoprotection in POC. BIOLOGICAL BASIS OF SKIN CARCINOGENESIS AND PHOTOAGING IN POC Few studies have been performed to thoroughly evaluate biological differences between differing ethnic skin types. Skin color is primarily determined by the presence of melanin. Jimbow et al9 reported that dark skin has larger melanocytes that produce more melanin and melanosomes are distributed individually in keratinocytes rather than in aggre- gates. The rarity of cutaneous malignancy in populations of darker complexions is secondary to photoprotection from a higher amount of epidermal melanin, which filters at least twice as much UV radiation as the epidermis of whites.10 In an in vitro study performed by Kaidbey et al,11 the amount of UV radiation reaching the papillary dermis of whites was greater than that of blacks by approximately 5-fold. The authors proposed that larger and more melanized melanosomes observed in POC absorbed more energy than the melanosomes in white skin, which were smaller, less dense, and lightly mela- nized. Furthermore, the authors estimated that the epidermis of blacks has an intrinsic sun-protection factor (SPF) of 13.4, whereas light skin has an SPF of
- 9. 3.3.11 Therefore, exposure to UV radiation plays a lesser role in heightening the risk for skin cancer in populations of darker complexions. Damage to DNA secondary to UV radiation is a major factor in cutaneous photocarcinogenesis and photoaging. However, the correlation of ethnicity and degree of sensitivity to UV rays has not been elucidated. Tadokoro et al12 performed a study evaluating the correlations between melanin content and degree of UVA- and UVB-induced DNA damage in normal-appearing skin of various ethnic groups. DNA damage was found to be most severe in qualitatively light skin. Baseline skin pigmentation and extent of DNA damage were inversely related, as individuals of darker skin tones were able to repair UVA-/UVB-induced DNA damage more rapidly than subjects with fair skin. Even low exposure to UVA/UVB radiation induced some appreciable DNA damage in all skin types, dispelling the myth that those with very dark skin are completely im- mune to UVA-/UVB-induced DNA damage.12 Indeed, NMSC and MM do occur in POC, despite the low relative risk.13 Because of the limited research on skin cancer in POC, there are few resources providing insight on evaluating darkly pigmented lesions in POC. Frequently atypical presentations, together with constitutive dark pigmentation, pose diagnostic challenges in the identification of characteristics such as variation in color within the lesions. Furthermore, certain skin cancers that are pigmented in POC may not be pigmented in whites (such as basal cell carcinoma, which is more likely to be pigmented in darker skin types); therefore, a high index of suspicion in POC is
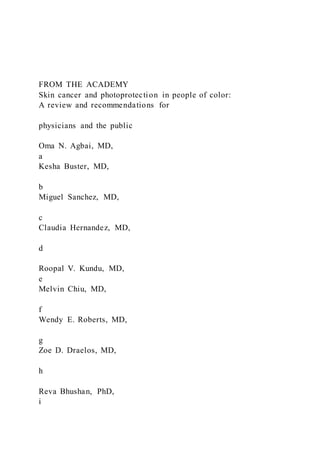
- 10. necessary in making the diagnosis. 5 BASAL CELL CARCINOMA Basal cell carcinoma (BCC) is the most prevalent skin cancer found in whites, Asians, and Hispanics.14 Hispanics are more likely to be given a diagnosis of multiple BCC rather than a single squamous cell Fig 1. Nonmelanoma skin cancers in people of color. Pigmented basal cell carcinoma in elderly Hispanic man (right lateral orbital rim) (A); middle- aged Asian woman (right cheek) (B); middle-aged Hispanic man (right forehead) (C); and middle-aged Hispanic man (left nasal ala) (D). Hypopigmented mycosis fungoides in Hispanic man (back) (E) and black man (lower aspect of back) (F). G, Metastatic squamous cell carcinoma in black man (right parietal scalp, courtesy of Dr Marc Silverstein, Sacramento, CA). J AM ACAD DERMATOL APRIL 2014 750 Agbai et al carcinoma (SCC).15 In contrast to Hispanic popula- tions, BCC is the second most common skin malig- nancy in blacks after SCC.4,5 The clinical spectrum of disease in BCC shows many parallels among blacks, whites, Asians, and
- 11. Hispanics. The classic clinical presentation of a solitary pearly papule with central ulceration and rolled borders may be seen in POC, but may pose challenges in the physical examination as the characteristic pearly borders and telangiectasia may not be clinically as apparent in dark skin types (Fig 1). In whites, the majority of patients presenting with BCC are of advancedage([50years),mostcommonlypresenting with asymptomatic solitary translucent nodules with central ulceration.14 Pigmentation is present in over 50% of tumors in POC,4,16 whereas only 5% of BCCs affecting whites have been shown to be pigmented. In Asians, BCCs frequently present as brown to black papules, or have a ‘‘black pearly’’ appearance.17 The clinical presentation of BCCs in Asian skin ranges from nodules to papules, plaques, and ulcers.18 With regards to anatomic distribution, there are significant similarities between POC and whites. Approximately 80% of BCCs in POC were found in the head and neck,19 as has been shown in whites.14 Differential diagnosis for BCC in POC includes seborrheic kera- tosis, blue nevus, trauma, lupus erythematosus, nevus sebaceous, sarcoidosis, and melanoma.20 Metastasis in BCC is rare in all skin types.14 BCC in blacks Although quite rare, BCC has been reported in the black population. In a report from Howard University (Washington, DC) from 1960 through 1986, most BCCs were seen in blacks of fairer skin complexion in comparison with those with darker complexions.19 From this, one may conclude that the incidence of BCC may correlate directly with the degree of skin pigmentation, as it is most frequently diagnosed in whites of fairer complexions, and more
- 12. rarely diagnosed in blacks. A study of skin cancer prevalence was conducted by Asuquo et al21 in a Nigerian teaching hospital between the years of 2000 and 2004. Of 63 cases of skin cancer, BCC was diagnosed in 8% (n = 5) of the cases; 66.7% of the BCC were on the head and neck, and 33.3% on the upper limb. All of these lesions were nodular. BCC was diagnosed only in albinos in this study.21 In a review of 128 black patients with 148 BCCs, Mora and Burris3 (New Orleans, LA) found that the average age of examination (not necessarily onset) was 59 years, with lesions most commonly located on head and neck. Only 2 of these patients had albinism. J AM ACAD DERMATOL VOLUME 70, NUMBER 4 Agbai et al 751 The incidence of BCC in non-sun-exposed skin is equal between whites and blacks.22 Diverse pre- sentations and locations of BCCs have been found in blacks, ranging from superficial BCC to perianal BCC.3,11 BCCs in blacks are often pigmented, and there are reports of BCCs that have arisen in scars, which rarely proceeded to metastasize.3,4,23 BCC in Hispanics One of the most common neoplasms diagnosed in Hispanics is pigmented BCC.16 Hispanics studied demonstrated significantly lower incidence rates of BCC than non-Hispanic whites regardless of gender.24 Still, a high index of suspicion should be
- 13. maintained in evaluating pigmented lesions in Hispanics, as BCCs have a propensity to be pig- mented in Hispanic populations and may be mis- diagnosed as melanomas.16 In a study performed by Bigler et al16 (Albuquerque, NM), the incidence of pigmented BCC in Hispanics was found to be twice that of white patients. Compared with whites, Hispanics with NMSC were shown to have fewer tumors per individual, and fewer Hispanics had more than 1 tumor.24 A registry of skin cancers in New Mexico between the years of 1964 and 1992 showed an average of 1.8 tumors per individual with NMSC among Hispanics, compared with 2.2 tumors per individual with NMSC in whites. Of these, BCC was more common than SCC by 6.6-fold in both Hispanics and whites.24 BCC in Asians Although NMSC is not common in Asians, it is not extremely rare. In a study by Cheng et al25 studying incidence of NMSC between 1990 and 1999 in Hong Kong, China, the incidence of BCC was 0.32 and 0.92 per 100,000 population. Pigmented BCC was the most common NMSC diagnosed, found in approxi- mately 60% of Chinese patients with skin cancer in the study.25 Multiple or subsequent skin cancers and subtypes of new cancers were seen less often in the Chinese group when compared with the white group.25 Similarly, Sng et al26 reported an increase of skin cancers including BCC, SCC, and MM, in Singapore between the years of 1998 and 2006. The extremities were the most common sites affected by Bowen disease (SCC in situ).27 There is an increased incidence of NMSC in Japanese living in Kauai,
- 14. Hawaii, which may be secondary to heightened intensity of year-round UV radiation and popularity of outdoor activities, as reviewed by Lee and Lim.28 SQUAMOUS CELL CARCINOMA SCC comprises approximately 20% of all skin cancers. With MM excluded, approximately 75% of all deaths from skin cancers are caused by SCC. 29 In blacks and Asian Indians, SCC is the most commonly diagnosed skin cancer. It is the second most commonly diagnosed skin cancer in Hispanics, East Asians (including Japanese and Chinese patients), and whites.5,30 Although actinic keratoses are most commonly diagnosed in white and Japanese pa- tients,31 they are very rare in blacks.32 Riskfactorsfor SCCinPOCincludechronicscarring and inflammatory processes including hidradenitis suppurativa, lupus erythematosus, scars caused by chemical and thermal burns, skin ulcers, and sites of previous radiation.33,34 Immunocompromised pa- tients, including organ transplant recipients, also demonstrate a heightened risk for SCC.35 Among blacks, the greatest predisposing factors for devel- oping SCC include chronic scarring and/or inflamma- tory processes that are observed in 20% to 40% of reported cases.4 In addition, the human papilloma- virus has been linked to the development of SCC, particularly in immunocompromised patients.36 One retrospective study detected human papillomavirus DNA in skin samples of 4.7% of controls, 90.5% of benign warts, 60.4% of precancerous lesions, 59.7% of
- 15. SCC, and 27.8% of BCC, suggesting a link between viral infection and the development of NMSC.37 Definitive studies have not been performed on the relationship between human papillomavirus infection and NMSC in POC. SCCs are characteristically firm, superficial, w ell- demarcated papules or plaques that emerge from a rounded, indurated, and elevated base.29 In POC, SCC is most commonly found in areas that are not typically exposed to the sun, such as the lower extremities and anus. In fact, lower extremity and anogenital SCCs were seen in 15% of SCCs in blacks in a study conducted by Halder and Bang19 in Washington, DC. This is a sharp contrast to the white population, in whom SCCs are characteristically seen in chronically sun-exposed skin.19 SCC in blacks Among black patients given the diagnosis of SCC, the peak incidence was shown to be in the fifth decade on the lower limbs, followed by the head and neck and then the genitals. The scalp and lip are more often implicated in black women than in men.38 Chronic trauma, ulcers, and scars are the most significant predisposing factors for SCCs in the lower limb and on the scalp, as reported by Amir et al38 (Dar es Salaam, Tanzania) in a study of SCC in Tanzanian patients, where UV radiation was found to be the primary factor predisposing pa- tients to increased risk of SCC in the head and neck. In a study done in Tanzania, smegma of the
- 16. J AM ACAD DERMATOL APRIL 2014 752 Agbai et al uncircumcised penis was also reported as a risk factor for the majority of cases of SCC developing on the penis in blacks.38 The majority of SCC on the penis were found to be SCC in situ upon histologic analysis in a study performed by Hubbell et al39 (New Orleans, LA). SCC was the most common skin cancer reported in a Nigerian teaching hospital between 2000 and 2004 by Asuquo et al, 21 where the lower limb was the most commonly affected anatomic site. SCC manifesting as Marjolin ulcer associated with trau- matic injury of the limb was diagnosed in 7 patients, and associated with a history of burn in 1 patient. SCC involved the external genitalia in 9 patients, 3 of whom had genital warts. The anus was affected in 4 female cases. There were no lesions involving the head and neck regions, and all patients in this study presented with chronic ulcers.21 Several cases of the emergence of SCC within scars of chronic discoid lupus erythematosus in black patients have been reported. Caruso et al40 reported a heightened propensity for SCC to metastasize in black Canadian patients with discoid lupus erythe-
- 17. matosus. Sun exposure of hypopigmented lesions of discoid lupus erythematosus may have been a predisposing factor. In blacks, Bowen disease (SCC in situ) typically presents as scaly hyperkeratotic pigmented pla- ques, and may be misdiagnosed as MM. In contrast, Bowen disease lesions are rarely pigmented outside of the groin in whites.41 Black women are affected twice as often as black men, and most frequently in skin that is not sun exposed.19 In a study performed by Mora et al42 in New Orleans, LA, evolution to SCC was noted in 5 of 19 black patients with Bowen disease, leading to death in 3 of these patients. The most common area affected was the lower extremity.42 Mortality of SCC in blacks is as high as 29%, secondary not only to delays in diagnosis and treatment, but also to more aggressive biologic behavior of SCC in this popu- lation.41,43 In blacks, SCC that develops within a chronic scarring process tends to be more aggres- sive and is associated with a 20% to 40% risk of metastasis. In contrast, the rate of metastatic trans- formation of sun-induced SCC in blacks is approx- imately 1% to 4%.4 In a case series on SCC in blacks performed by Mora and Perniciaro 33 (New Orleans, LA), the highest mortality was observed in cases of perianal SCC. Although most patients with primary SCC have a very good prognosis, the 10-year survival is less than 20% in patients with regional lymph node metastasis, and less than 10% in patients with distant metastasis.29
- 18. SCC in Asians Bowen disease and pigmented BCCs are not uncommonly diagnosed in Asians. Because of their pigmented appearance, as in blacks, these may be misdiagnosed as MM.25 Although NMSC is uncom- mon, it is not rare in the Chinese population in Hong Kong. Cheng et al25 (Hong Kong, China) reported that the incidence of SCC in 1990 was 0.16 per 100,000 population, and in 1999, 0.34. Similarly, in a case-control study performed by Chen et al44 in Taiwan evaluating the association between UV radi- ation exposure from the sun and risk for develop- ment of SCC by gender, exposure at a young age (15-24 years) and cumulative sun exposure were significantly associated with heightened risk of SCC in a dose-related pattern. Cumulative sun exposure was found to be more closely related to increased risk of SCC in women, whereas sun exposure at an early age showed more relevance to SCC risk in men.44 Skin reactions such as redness, burn, and suntan after 2 hours of sun exposure in childhood and adolescence were not associated with increased risk for SCC.44 In a study on skin cancer incidence between 1986 and 1997 among Asians living in Singapore, 2650 BCCs were reported. There was a general increase in skin cancer incidence from 6 per 100,000 person- years (from 1968-1972) to 8.9 per 100,000 person- years (1993-1997). The incidence of BCC increased approximately 3% yearly. Age-standardized inci- dence rates for BCC were greatest in fair-skinned Chinese, followed by Malays and Indians. This trend was also noted for SCC and cutaneous MM.
- 19. 45 MALIGNANT MELANOMA MM is the deadliest type of skin cancer found across all races and ethnicities. Many melanoma cases are diagnosed in nonhospital settings and thus may be underreported to central cancer registries, which traditionally collect the majority of cases from hospi- tals.46 This could lead to significant underreporting of MM and resultant underestimation of the incidence of melanoma.47 The National Cancer Institute, Division of Cancer Control and Population Sciences, Surveillance Research Program, Cancer Statistics Branch (Bethesda, MD) reports that the incidence of cutaneous MM increased by approximately 6% yearly in the 1970s, slowed to a 3% yearly increase between 1981 and 2000, and has since stabilized.48 Since the late 1980s, the incidence of MM has increased significantly among Hispanics in California, increasing an average of 1.8% yearly in male Hispanics between 1988 and 2001, and 7.3% average yearly between 1996 and 2001.49 In a study conducted by Bergfelt et al,50 the incidence of MM Fig 2. Melanomas in people of color. A, Lentigo maligna in middle-aged Hispanic woman (vermilion upper and lower lips). Melanoma in middle-aged black woman (right fourth toe) (B); Hispanic woman (left fifth toe) (C); middle-aged Hispanic man (left plantar foot) (D); elderly Hispanic man (right cheek) (E); and Asian woman (side of left leg) (F).
- 20. J AM ACAD DERMATOL VOLUME 70, NUMBER 4 Agbai et al 753 among Hispanics in Puerto Rico and New Mexico (race not specified) was greater than in US blacks by 1.6- to 3.7-fold. There was a close correlation in anatomic distribution of MM among whites and Hispanics in New Mexico in both men and women. The most common MM distribution in Hispanics from Puerto Rico was the leg, as was seen in black Americans.50 In another study, Vazquez-Botet et al51 reported that nearly half of MM in Hispanic patients in Puerto Rico were found on the extremities, especially the feet, similar to black and Japanese patients. Superficial spreading melanoma was the most com- mon histologic type, followed by acral lentiginous, nodular, and lentigo maligna melanomas.51 More recently, Wu et al52 (New Orleans, LA) reported that incidence rates of MM in the United States were notably higher in females than males in white and Hispanic populations younger than 50 years, and in Asian/Pacific Islanders younger than 40 years. The median age of white and black patients was greater (59-63 years) when compared with Hispanics, Asian/ Pacific Islanders, and American Indians/Alaskan Natives (52-56 years).52 Histologically, acral lentigi- nous melanoma was the most common subtype in blacks, whereas superficial spreading melanoma was most commonly diagnosed in all other ethnic groups studied.52 Incidence rates of acral lentiginous melanoma were, however, highest in Hispanics. Non-whites demonstrated an increased propensity to present with more advanced MM when compared
- 21. with whites.52 Typically, MM presents as a dark macule or patch and may have a history of rapid spreading. Suspicion for subungual melanomas is raised when a pig- mented band wider than 3 mm is observed on the nail, extension of pigment to proximal nail fold (Hutchinson sign) and there is pigment variation, rapid growth in size, and the observation of solitary lesions.4 Subungual melanoma is most common on the thumb and first toe. In populations of color, the plantar foot is most commonly affected (Fig 2),53 as it is implicated in 30% to 40% of cases.54 Melanomas found in the oral cavity comprise approximately 7.5% of all melanomas in Asians, where approximately 60% of these develop from lesions of oral melanosis. The greatest risk factors for the development of MM in whites include periods of high intermittent sunlight exposure (as in sunbathing and indoor tanning), and large cumulative doses of UV radiation from chronic exposure (as seen in outdoor workers).55 Factors in the host that may increase susceptibility to develop- ment of melanoma include a large number of nevi, the presence of dysplastic nevi, freckles, fair complexion, red or blonde hair, and family history of MM.55 J AM ACAD DERMATOL APRIL 2014 754 Agbai et al Contrarily, in blacks and Asians, UVradiation does not appear to be a major risk factor, as the majority of melanomas are found in skin that is not typically sun
- 22. exposed, including palmar, plantar, and subungual skin, and mucous membranes.56 In POC, the risk factors for MM have not been identified, but may be unrelated to sun exposure.57 Specifically, as acral melanomas are identified with similar rates at different latitudes and in varying racial groups, and as they tend to be diagnosed in anatomic sites that are not typically sun exposed, their origin may be unrelated to sun exposure.28 MM in blacks In black Americans, acral lentiginous melanoma is the most common and deadly form of MM.56,58 Not uncommonly it is misdiagnosed and managed as a tinea nigra, or even talon noir. In a retrospective study performed at Tulane University School of Medicine (New Orleans, LA)58 from 1958 to 1990, 82 patients (including 27 white men, 29 white women, 18 black men, and 8 black women) with a diagnosis of acral lentiginous melanoma were fol- lowed up, and the study showed a trend toward reduced survival in black men. A direct correlation between decreased survival and increased Clark level was also observed. As previously mentioned, the overall incidence of melanoma in the black population is lower than that of whites. Additional types of melanoma found in black Americans include superficial spreading and nodular types. 13 Acral lentiginous melanoma has a poor prognosis secondary to its propensity for deep invasion at presentation, with 5-year survival lower than 50%.59
- 23. In a study of skin cancers in a teaching hospital in Nigeria between 2000 and 2004, MM of the skin represented 8% (n = 5) of the 63 histologically diagnosed cutaneous malignancies. All of these MMs were plantar. Three of the 5 cases were clinically advanced nodular melanomas, whereas 2 were ulcerated superficial spreading melanomas.21 MM in Hispanics Pipitone et al60 (Maywood, IL) proposed that Hispanics had a propensity to present with more advanced disease secondary to the combination of a belief that they are not at risk to sunburn and/or develop skin cancer. Skin cancer prevention mea- sures are typically directed toward non-Hispanic whites, where skin self-examination and sun protec- tion are emphasized.13 Feun et al61 (Miami, FL) reviewed 54 melanoma cases in Hispanic patients; the majority of melanomas were located on the trunk, arm, shoulder, leg, and hip. Although 70% of these patients presented with local disease, 26% presented with regional and distant lesions. In this study, Hispanics given the diagnosis of melanomas had better treatment outcomes and survival than non-Hispanics.61 This contradicts a handful of other studies that have demonstrated poorer survival in Hispanic populations.57,62,63 MM in Asians In Asian populations, the sole of the foot is the most common site for MM.28 This is typically acral lentiginous melanoma.28 As in blacks and Hispanics, MMs in Asians have a propensity to be diagnosed at a late stage in comparison with whites.57 In a study
- 24. done in Taiwan, factors such as age over 55 years, male gender, tumor thickness, and tumor ulceration were generally predictive of a poorer prognosis.64 In a study done in Japan, loss of the p53 gene though deletion mutation was associated with more aggres- sive subtypes of MM.65 Although in whites, number of melanocytic nevi is directly proportional to risk of developing MM,66 this may not be the case in POC. The density of melanocytic nevi is significantly lower in POC than in whites.66 Gallagher et al66 (Vancouver, British Columbia, Canada) found that nevus density in Asians was unrelated to skin color or tendency to burn. These findings may indicate a lack of correla- tion between nevi density and MM in POC; however, further research is needed to clarify this point. Survival in MM across ethnicities The 5-year survival for melanoma in Hispanic and black populations has been shown to be consistently lower than in whites.6,53,67 When compared with whites, black and Hispanic populations have a pro- pensity to present with thicker tumors that are more advanced, therefore leading to a worse prognosis. In reviewing several melanoma cases in California, Cockburn et al49 demonstrated that diagnosis of tumors with a thickness greater than 1.5 mm upon presentation increased at 11.6% yearly and 8.9% yearly in Hispanic males and females, respectively. Hu et al62 performed a retrospective analysis of case series in the Florida Cancer Data System, showing that late-stage melanomas were most commonly diagnosed in black and Hispanic patients, at rates of 52% and 26%, respectively. In contrast, late-stage
- 25. MM was diagnosed at a rate of 16% in white populations.62 In reviewing MM cases in California, blacks are have a higher rate of death in comparison with their white counterparts after adjusting for sex, age, stage, histology, anatomic site, socioeconomic status, and treatment.68 Therefore, the lower survival for blacks with MM is not fully accounted for by discrepancies in socioeconomic standing or access to J AM ACAD DERMATOL VOLUME 70, NUMBER 4 Agbai et al 755 adequate medical care. This leads to a conclusion that more aggressive primary and secondary preven- tion measures are needed for the diagnosis and control of MM across all races, including groups that have a lower risk of developing MM.69 MYCOSIS FUNGOIDES Mycosis fungoides (MF) is more commonly diag- nosed in whites than in POC. However, incidence and prognosis vary significantly based on race. Weinstock and Gardstein70 used the US Surveillance, Epidemiology, and End Results (SEER) program of the National Cancer Institute to study the incidence of MF in blacks, whites, and Asians in the United States from 1973 to 1992. After adjusting for age, blacks had a higher incidence of MF than whites, with an incidence rate ratio of 1.6. The incidence of MF in Asians was lower than that of whites, with an incidence rate ratio of 0.6. Furthermore, blacks with MF had a worse prognosis than whites, with a
- 26. mortality ratio of 2.4 compared with whites. In contrast, the mortality ratio of Asians compared with whites was 0.5. The cause for these differences in incidence and mortality are unknown.70 In a more recent study, Criscione and Weinstock71 used the SEER database to study incidence of cutaneous T-cell lymphoma in whites and blacks between 1973 and 2002. The incidence was 9.0 per 1 million person- years in blacks, whereas incidence of cutaneous T-cell lymphoma was 6.1 per 1 million person-years in whites. MF typically presents as erythematous or hyperpigmented patches in individuals of darker complexion.13 Hypopigmented MF is diagnosed almost exclusively in POC. It typically presents as poorly defined hypopigmented patches (Fig 1).20,72,73 Distribution is typically more central than acral, and mild pruritus is often present.13 Differential diagnosis includes pityriasis alba, tinea versicolor, vitiligo, postinflammatory hypopigmenta- tion, and tinea corporis. Biopsy should be done in cases unresponsive to treatment for the aforemen- tioned conditions, or in patients who exhibit wors- ened disease despite treatment. Multiple biopsy specimens are often needed to confirm the diag- nosis.20 Immunohistochemical analysis often reveals a relative loss of the CD7 antigen. 74 OTHER SKIN CANCERS There is limited information on other skin cancers diagnosed in POC. Dermatofibrosarcoma protuber-
- 27. ans (DFSP) is a slow-growing spindled cell neoplasm located in the dermis or subcutaneous tissue. It can present as a rare pigmented form that comprises up to 5% of DFSP. The pigmented variant occurs primarily in blacks. DFSP most commonly presents on the trunk, followed by the upper and lower extremities and the head and neck. Clinically it may resemble a keloid, raising suspicion for keloidlike lesions in blacks that have no clear history of trauma.41 One study conducted in Nigeria reported 5 DFSP in 63 skin cancers diagnosed between 2000 and 2004. Three of these presented with recurrent lesions, and positive margin in 1 patient after initial excision. 21 Pigmented DFSP may be histologically distinguished from the common variant through the presence of a dendritic cells containing melanin. DFSP tend to have a high local recurrence rate, though there have been reports of distant metastases. Wide excision and close clinical follow-up are indicated.13 Merkel cell carcinoma occurs at a rate of 0.2 and 0.01 per 100,000 in whites and blacks, respectively. Increased sun exposure corresponds with increased incidence, as the face is the most commonly affected site.75 Merkel cell carcinoma is rarely seen in Asians, though there have been case reports associating Merkel cell carcinoma with other skin cancers such as Bowen disease.76 PHOTOAGING AND UV-RELATED DYSPIGMENTATION IN POC
- 28. Although skin cancers pose the greatest mortality risk when discussing the need for photoprotection in POC, additional adverse effects of UVexposure, such as photoaging and UV-related exacerbation of pigmentation disorders, must be considered. Up to 95% of the visible signs of aging are a result of exposure to the sun, which starts in childhood and persists throughout life. Clinical signs of photoaging apparent in white skin may be less noticeable in POC of comparable age groups, implying a role of skin color in photoprotection.77 Despite the protective effects of darker skin on photoaging, signs of pho- toaging are still prevalent in POC. Dyspigmentation is more commonly seen in POC, whereas wrinkling is more prevalent in whites. As pigmentation disor- ders such as postinflammatory hyperpigmentation and melasma are generally more prevalent in POC, photoprotection may prevent worsening and recur- rence of these conditions.77 Kotrajaras and Kligman78 (Bangkok, Thailand) reported that significant photodamage manifested as dermal collagen and elastin damage, epidermal atypia and atrophy, and disorders of pigmentation are not uncommonly seen in POC. Similarly, other studies have observed that pigmentary changes may be more common than skin wrinkling with regards to photoaging among Asians.79,80 Chan et al81 (Hong Kong, China) observed that moderate to severe wrinkling becomes evident at around 50 years in J AM ACAD DERMATOL APRIL 2014
- 29. 756 Agbai et al Asians, 1 or 2 decades later than in age-matched whites. Chung et al82 (Seoul, South Korea) performed a study evaluating the type and severity of photo- damage in Koreans and observed that women had a propensity to have more wrinkles than men. Seborrheic keratosis was the major pigmentary lesion observed in sun-exposed skin of men, whereas hyperpigmented macules were more often seen in women. Although cigarette smoking was found to be an independent risk factor for wrinkles, this was not so for dyspigmentation.82 There was no correlation between constitutive skin color and development of wrinkles or dyspigmentation. The authors concluded that wrinkling and pigmentary changes are significant manifestations of photoaging in Koreans. 82 Additional cutaneous manifestations of photoag- ing in ethnic skin include development of benign lesions such as solar lentigines and dermatosis papulosa nigra.81,83 SUN-PROTECTION BELIEFS AND PRACTICES IN POC Although POC are most commonly categorized into skin phototypes IV to VI, it should be noted that ethnic skin colors can span the entire spectrum of skin phototypes.84 Skin examination and photo- protection practices differ between ethnic groups as whites and Hispanics have a greater propensity to
- 30. use sunscreen than blacks.69 In addition, whites are more likely to perform skin self-examinations than Hispanics. Although blacks and Hispanics show similar practices in performance of skin self- examinations, blacks tend to follow up with derma- tologists less frequently.13 One survey study showed that blacks who self-reported experiencing severe sunburns were 7 times less likely to use sunscreen than their white counterparts who reported experi- encing severe sunburns. Among those surveyed who had severe sunburns in other ethnic groups (eg, Mexican American, other Hispanic, and other races), there was no such difference in sunscreen use.85 Although UV radiation exposure continues to become a more significant causative factor for skin cancer in blacks, discussion of their UV radiation- protection practices remains inadequate. Hall and Rogers86 (Atlanta, GA) analyzed the National Health Interview Survey performed in 1992 (n = 1583), in which approximately 6% of blacks reported marked sensitivity to sunlight with occurrence of severe sunburn, whereas 9% reported mild burning. Of the subjects studied, 53% self-reported a high likeli- hood of wearing protective clothing, sunscreens, or seeking shade. Factors such as educational background, age, and sunburn history contributed to a tendency toward better photoprotection habits with sunscreens.86 Similarly, Buster et al87 (Birmingham, AL) evaluated a cross-sectional survey data from the National Cancer Institute to evaluate cancer-related knowledge, attitudes, and behaviors. There were 1246 respondents, including whites, blacks, and Hispanics. Blacks perceived their likeli- hood of developing skin cancer in the future as low,
- 31. and were less likely than whites to recognize that behavior and lifestyle influence the risk of devel- oping skin cancer. Furthermore, blacks and Hispanics were more likely to believe that skin cancer is associated with pain or another symptom. Blacks less frequently viewed regular skin examina- tions as necessary for early detection of skin cancer, and both blacks and Hispanics were more likely to believe that little can be done to decrease the risk of developing skin cancer.87 In a survey performed by the Skin of Color Center in New York, NY, blacks and Hispanics self-reported low sunscreen use, secondary to misconceptions that it is unnecessary to use sun protection to prevent photoaging or skin cancers.77 If used at all, sun- screens were generally insufficiently applied and not reapplied frequently enough. Sanclemente et al88 (Medellin, Colombia) performed a study evaluating sun-protection behavior, skin phenotype , and min- imal erythema dose (MED) in 911 high school students in Colombia. There was significant vari- ability in MEDs among the different phototypes represented in the population, as individuals with fairer skin appeared to respond to UV radiation similar to their darker-skinned colleagues, and some students with darker skin responded similar to what would be expected from someone of lighter skin. This suggested a lack of predictability of MEDs based on skin phototype. In this population, only 10% of students who completed the associated questionnaire reported use of sunscreens or prac- ticed photoprotection. 88
- 32. Studies have shown that educational intervention may be helpful in improving photoprotection prac- tices. In a study performed by Kundu et al89 (Chicago, IL), POC (n = 93) were given instruction on how to identify potentially abnormal moles in cutaneous self-examination. Races represented in the study included Asian/Pacific Islander (21.5%), black American (59.1%), Hispanic (15.1%), and multiracial or ‘‘mixed’’ (4.3%). The investigators used self-report questionnaires evaluating attitudes, practices, and beliefs before, immediately after, and 3 months after the educational intervention.89 In all, 21% self-reported a skin phenotype that sometimes burns, and 32% reported at least 1 blistering sunburn Table I. Recommendations for photoprotection and early detection of skin cancer in people of color n Seek shade whenever possible. n Wear sun-protective clothing. n Wear a wide-brimmed hat to shade the face and neck, and shoes that cover the entire foot. n Wear sunglasses with ultraviolet-absorbing lenses. n Apply broad-spectrum sunscreen with a sun-protection factor of 30 or greater. Sunscreens without inorganic filters (titanium dioxide and zinc oxide) are generally better accepted by people of color because of their better cosmesis on dark skin. n Apply sunscreen to dry skin 15 to 30 minutes before going outdoors. When outdoors, reapply every 2 hours to all exposed
- 33. skin, and after perspiring or swimming. n Avoid exposure to indoor tanning beds/lamps. n Take vitamin D supplement. n Perform monthly self-skin examinations, paying close attention to subungual skin, palms, soles, mucous membranes, groin. and perianal area. Table II. Recommendations for physicians for people of color n Educate patients: People of color are at risk for developing skin cancer. Practice sun-protective behaviors. Perform monthly self-skin examinations for those with multiple nevi, or history of skin cancers. Avoid tanning salons. Obtain regular skin examination by a dermatologist. n Perform a thorough skin examination including areas infrequently exposed to the sun, such as palms, soles, oral mucosa, groin, and perianal area. Regularly ask patients to remove shoes and socks for skin examination. n Monitor changes in pigmented lesions, including those of mucosal, palmar, plantar, interdigital spaces, and subungual surfaces. n Advise vitamin D supplementation as indicated. n Refer to dermatologists: Changing pigmented lesions. Nonhealing ulcers. Hyperkeratotic or poorly healing lesions in chronic lesions such as those of discoid lupus erythematosus, or in scars. Atypical appearing keloidal plaques, or those with
- 34. growth/development with no history of trauma. J AM ACAD DERMATOL VOLUME 70, NUMBER 4 Agbai et al 757 in the past. Of the original 93 subjects, 71 returned for follow-up evaluation after 3 months. Improved knowledge of MM as a skin cancer, and of concern- ing signs for melanoma was observed after the educational intervention. Furthermore, awareness of MM risk was shown to improve and was main- tained at 3 months. Practices such as performance of monthly self-skin checks, particularly of palms, soles, and periungual skin, dramatically improved after the intervention.89 VITAMIN D AND PHOTOPROTECTION Vitamin D has been shown to be beneficial for bone health, and has been reported to have other potential health effects, including reduction of colo- rectal cancer, and reduction in cardiovascular dis- ease.90 Therefore, the question of whether or not rigorous photoprotection increases the risk of vitamin D deficiency is an important one. Individual variables such as amount of skin pigmen- tation play a role in determining vitamin D produc- tion. There has been an emergence of vitamin D deficiency and rickets in dark-skinned patients in northern latitudes of the United States and United Kingdom. Meanwhile, similar populations in their countries of origin did not have this problem, which has led to suspicion that increased skin pigmentation may predispose dark-skinned patients to have vitamin D deficiency in certain geographic loca- tions.91 Because POC, especially those of darker
- 35. skin, may have a higher risk for vitamin D insuffi- ciency secondary to higher skin melanin content,92 vitamin D supplementation should be recommen- ded as part of a photoprotection regimen for POC. Although there have been studies demonstrating decreased serum vitamin D levels in patients with photosensitivity practicing rigorous photoprotec- tion,93-95 regular use of sunscreens did not result in inadequate serum vitamin D level.95-97 It should be Table III. Melanoma, basal cell carcinoma, squamous cell carcinoma, and Bowen disease in people of color Skin cancer Pertinent demographics Physical presentation Differential diagnosis in POC Anatomic distribution Major risk factors in POC Melanoma Median age of diagnosis in all races ranges from 52-63 y Skin: Dark macules or patches with history of rapid spreading Nail: Pigmented band [3 mm on the nail Oral mucosa: Oral melanomas can rise from lesions of oral melanosis Tinea nigra palmaris, talon noir, pigmented BCC
- 36. Commonly in lower extremities and plantar feet UV radiation NOT a major risk factor Risk factors for melanoma in POC unknown BCC Most prevalent skin cancer in Hispanics14; second most common in blacks (in whom SCC is the most common)4,5 Typical: Asymptomatic solitary translucent nodules with pearly borders, rolled borders, and telangiectasia14 POC: Pigmentation in over half of cases; brown/black papules can also present as nodules, plaques, and ulcers 4,16,18 Seborrheic keratosis, blue nevus, trauma, lupus erythematosus, nevus sebaceous, sarcoidosis, and melanoma5,18
- 37. Head and neck most common in both whites and POC 15,19 Family history of skin cancer, Fitzpatrick skin type I, and the presence of actinic keratoses, solar lentigines, leukoderma, and elastosis rhomboidalis nuchae, UV radiation SCC Most common skin cancer in blacks and Asian Indians; second most common in Hispanics, East Asians, and whites (second to BCC); in blacks: peak incidence in forties Range between well- demarcated scaling pink plaques; firm, superficial, well-demarcated papules/ nodules emerging from round, indurated elevated base; granulomatous or verrucous lesions; and nonhealing ulcers Lesions can be hypopigmented or hyperpigmented
- 38. Actinic keratosis, nummular eczema, inflamed seborrheic keratosis, verruca vulgaris Typically on the face in white skin; in POC, not uncommon in areas not typically exposed to the sun, including lower extremities and anus Lower limb/scalp SCC: Chronic scarring and inflammatory processes including hydradenitis suppurativa, lupus erythematosus, chemical/ thermal burns, chronic skin ulcers, chronic trauma sites of previous radiation; immunocompromised patients also at risk Head/neck SCC: UV radiation Bowen disease Black women affected twice as often as black men Scaly hyperkeratotic pigmented plaques resembling seborrheic keratoses Seborrheic keratoses, pigmented BCC, superficial
- 39. BCC, malignant melanoma, or nonspecific pigmented hyperkeratotic lesions Areas not typically exposed to the sun: including groin and extremities See SCC BCC, Basal cell carcinoma; POC, people of color; SCC, squamous cell carcinoma; UV, ultraviolet. J A M A C A D D E R M A T O L A P R IL
- 40. 2 0 14 7 5 8 A g b a i et a l J AM ACAD DERMATOL VOLUME 70, NUMBER 4 Agbai et al 759 noted that most of the vitamin D photoprotection studies were done in predominantly white popula- tion, raising a question to their applicability to the broader population. A guideline to follow would be Institute of Medicine recommendations of 400 IU of vitamin D daily for infants up to 1 year old, 600 IU for individuals between 1 and 70 years old, and 800 IU for those older than 70 years.98 The National Institutes of Health provided a listing of food sources of vitamin D, including but not limited to cod liver oil, salmon, tuna, swordfish, and vitamin Defortified
- 41. dairy products.99 THE SPF AND RECOMMENDATIONS FOR CLINICAL PRACTICE A recent survey performed by Pourciau et al100 demonstrated a general belief among leaders in photodermatology that photoprotection counseling is warranted in POC. Still, there is a general lack of strong data supporting recommendations on SPF requirements for specific skin phototypes. It is known that a given sunscreen may demonstrate different SPF value in varying skin colors, as demon- strated by Damian et al101 (Sydney, Australia) in 1999. Using a xenon arc lamp with an emission spectrum simulating the UVA and UVB wavelengths of natural sunlight, the investigators found testing a sunscreen product in fair-skinned individuals (who had low MED) yielded higher SPF values compared with testing the same product in dark-skinned sub- jects (with higher MEDs). Because commercial testing of SPF is mandated to be done in fair- skinned individuals,102 SPF values of sunscreens on dark skin therefore may be lower that the SPF values stated in the label.101 Similar to the message on photoprotection for the general population, POC should also be advised to use a daily broad-spectrum sunscreen of at least SPF 30, and practice sun-protective behavior such as seeking shade and use of protective clothing, wide- brimmed hat, and sunglasses (Table I). Sunscreens should be applied liberally and reapplied every 2 hours while outdoors. Furthermore, patients should be advised to avoid tanning salons and intentional
- 42. tanning with natural sunlight. A thorough skin examination, including examination of nails, oral cavity, gums, palms, soles, groin, and perianal area should be performed regularly by a dermatologist; for those older than 50 years, yearly examination is appropriate. Pigmented lesions on gums and streaks in nails are normal in POC, but should be monitored regularly for changes as malignant transformation can occur. For patients with history of skin NMSC or melanoma, or multiple nevi, monthly self-skin ex- amination is appropriate. Primary care physicians should be educated on high-risk sites for MM, such as palms and soles (Tables II and III). Efforts are needed to take the diversity in culture, beliefs, and language across ethnicities into account so that photoprotec- tion education can reach the target population of color. Wendy E. Roberts, MD, serves as a consultant for Allergan Medical, L’Oreal, La Roche-Posay, and NeoStrata, for which she receives honoraria. She also sits on the advisory board and consults for SkinMedica, for which she receives honoraria. She receives stock options from TopMD. She consults for Theraplex, for which she receives no compensation. In 2013, Susan Taylor, MD, held seats on the advisory boards of Allergan, Beiersdorf, Inc, Excaliard Pharmaceuticals, and Unilever, for which she receives honoraria. She serves as a consultant for Curel Skincare, Pfizer, Schlesinger Associates, and Viviscal. Dr Taylor founded T2 Skincare for which she receives other financial benefit and serves in other roles. She receives grants as an investigator for Hisamitsu Pharmaceutical, Medicis Pharmaceuticals, Noven Pharmaceuticals, and Pfizer. Dr Taylor has received honoraria as a speaker
- 43. from Allergan, Johnson & Johnson, Kao USA, Merz Pharmaceuticals, and Neostrata. 2012 found Dr Taylor serving as a consultant for Schlesinger Associates and Pfizer for which she received honoraria. She sat on the advisory board for Allergan, Beiersdorf and Excaliard Pharmaceuticals, for which she received honoraria. Dr Taylor founded T2 Skincare for which she received other financial benefit and served in other roles. She is an investigator for Pfizer, Medicis, Noven, and Hisamitsu, for which she receives honoraria. She contracted for Medscape/ WebMD for which she received honoraria. She served as a speaker for Merz Pharmaceuticals and Allergan for which she received honoraria. She receives no compen- sation for her role at the Philadelphia Life Sciences Institute. In 2011, Dr Taylor was awarded grants as an investigator for Medicis and Noven Pharmaceuticals. She received honoraria for speaking from Elsevier and Johnson & Johnson. Dr Taylor sat on the advisory board for Merz Pharmaceuticals and Beiersdorf and received honoraria for her support. She served as a consultant and received a consulting fee from Tria Beauty and Johnson & Johnson Dr. Taylor has received honoraria as researcher from Johnson & Johnson and Beiersdorf. Henry W. Lim, MD, serves as a consultant for Ferndale and La Roche-Posay for which he receives honoraria. Roopal V. Kundu, MD, had no relevant conflict of interest to disclose. Her department receives compensa- tion for pharmaceutical sponsored research that does not benefit her directly.
- 44. Oma N. Agbai, MD, Kesha Buster, MD, Miguel Sanchez, MD, Claudia Hernandez, MD, Melvin Chiu, MD, FAAD, Zoe D. Draelos, MD, and Reva Bhushan, PhD, had no relevant conflicts of interest to disclose. J AM ACAD DERMATOL APRIL 2014 760 Agbai et al REFERENCES 1. US Census Bureau. 2010 Census. Available from: URL:http:// www.census.gov. Accessed April 5, 2012. 2. Ridky TW. Nonmelanoma skin cancer. J Am Acad Dermatol 2007;57:484-501. 3. Mora RG, Burris R. Cancer of the skin in blacks: a review of 128 patients with basal-cell carcinoma. Cancer 1981;47: 1436-8. 4. Gloster HM Jr, Neal K. Skin cancer in skin of color. J Am Acad Dermatol 2006;55:741-60;quiz 61-4. 5. Halder RM, Bridgeman-Shah S. Skin cancer in African Americans. Cancer 1995;75:667-73.
- 45. 6. Byrd KM, Wilson DC, Hoyler SS, Peck GL. Advanced presen- tation of melanoma in African Americans. J Am Acad Dermatol 2004;50:21-4;discussion 142-3. 7. Hu S, Parmet Y, Allen G, Parker DF, Ma F, Rouhani P, et al. Disparity in melanoma: a trend analysis of melanoma incidence and stage at diagnosis among whites, Hispanics, and blacks in Florida. Arch Dermatol 2009;145:1369-74. 8. Cormier JN, Xing Y, Ding M, Lee JE, Mansfield PF, Gershen- wald JE, et al. Ethnic differences among patients with cutaneous melanoma. Arch Intern Med 2006;166:1907-14. 9. Jimbow K, Quevedo WC Jr, Fitzpatrick TB, Szabo G. Some aspects of melanin biology: 1950-1975. J Invest Dermatol 1976;67:72-89. 10. Montagna W, Carlisle K. The architecture of black and white facial skin. J Am Acad Dermatol 1991;24:929-37. 11. Kaidbey KH, Agin PP, Sayre RM, Kligman AM. Photoprotec-
- 46. tion by melaninea comparison of black and Caucasian skin. J Am Acad Dermatol 1979;1:249-60. 12. Tadokoro T, Kobayashi N, Zmudzka BZ, Ito S, Wakamatsu K, Yamaguchi Y, et al. UV-induced DNA damage and melanin content in human skin differing in racial/ethnic origin. FASEB J 2003;17:1177-9. 13. Halder RM, Ara CJ. Skin cancer and photoaging in ethnic skin. Dermatol Clin 2003;21:725-32, x. 14. Rubin AI, Chen EH, Ratner D. Basal-cell carcinoma. N Engl J Med 2005;353:2262-9. 15. Byrd-Miles K, Toombs EL, Peck GL. Skin cancer in individuals of African, Asian, Latin-American, and American-Indian descent: differences in incidence, clinical presentation, and survival compared to Caucasians. J Drugs Dermatol 2007;6:10-6. 16. Bigler C, Feldman J, Hall E, Padilla RS. Pigmented basal cell carcinoma in Hispanics. J Am Acad Dermatol 1996;34:751-2.
- 47. 17. Kikuchi A, Shimizu H, Nishikawa T. Clinical histopathological characteristics of basal cell carcinoma in Japanese patients. Arch Dermatol 1996;132:320-4. 18. Bradford PT. Skin cancer in skin of color. Dermatol Nurs 2009; 21:170-7, 206; quiz 178. 19. Halder RM, Bang KM. Skin cancer in African Americans in the United States. Dermatol Clin 1988;6:397-407. 20. Jackson BA. Nonmelanoma skin cancer in persons of color. Semin Cutan Med Surg 2009;28:93-5. 21. Asuquo ME, Ngim O, Ugare G, Omotoso J, Ebughe G. Major dermatologic malignancies encountered in a teaching hos- pital surgical department in South Nigeria. Am J Clin Dermatol 2008;9:383-7. 22. Chorun L, Norris JE, Gupta M. Basal cell carcinoma in blacks: a report of 15 cases. Ann Plast Surg 1994;33:90-5.
- 48. 23. Abreo F, Sanusi ID. Basal cell carcinoma in North American blacks: clinical and histopathologic study of 26 patients. J Am Acad Dermatol 1991;25:1005-11. 24. Hoy WE. Nonmelanoma skin carcinoma in Albuquerque, New Mexico: experience of a major health care provider. Cancer 1996;77:2489-95. 25. Cheng SY, Luk NM, Chong LY. Special features of non-melanoma skin cancer in Hong Kong Chinese patients: 10-year retrospective study. Hong Kong Med J 2001;7:22-8. 26. Sng J, Koh D, Siong WC, Choo TB. Skin cancer trends among Asians living in Singapore from 1968 to 2006. J Am Acad Dermatol 2009;61:426-32. 27. Chuang TY, Reizner GT, Elpern DJ, Stone JL, Farmer ER. Nonmelanoma skin cancer in Japanese ethnic Hawaiians in Kauai, Hawaii: an incidence report. J Am Acad Dermatol 1995; 33:422-6. 28. Lee CS, Lim HW. Cutaneous diseases in Asians. Dermatol Clin
- 49. 2003;21:669-77. 29. Alam M, Ratner D. Cutaneous squamous-cell carcinoma. N Engl J Med 2001;344:975-83. 30. Dhir A, Orengo I, Bruce S, Kolbusz RV, Alford E, Goldberg L. Basal cell carcinoma on the scalp of an Indian patient. Dermatol Surg 1995;21:247-50. 31. Suzuki T, Ueda M, Naruse K, Nagano T, Harada S, Imaizumi K, et al. Incidence of actinic keratosis of Japanese in Kasai City, Hyogo. J Dermatol Sci 1997;16:74-8. 32. Hale E. Current concepts in the management of actinic keratoses. J Drugs Dermatol 2004;3(Suppl):S3-16. 33. Mora RG, Perniciaro C. Cancer of the skin in blacks, I: a review of 163 black patients with cutaneous squamous cell carci- noma. J Am Acad Dermatol 1981;5:535-43. 34. Copcu E, Aktas A, Sisman N, Oztan Y. Thirty-one cases of Marjolin’s ulcer. Clin Exp Dermatol 2003;28:138-41. 35. Harwood CA, Surentheran T, McGregor JM, Spink PJ, Leigh
- 50. IM, Breuer J, et al. Human papillomavirus infection and non-melanoma skin cancer in immunosuppressed and immu- nocompetent individuals. J Med Virol 2000;61:289-97. 36. Karagas MR, Nelson HH, Sehr P, Waterboer T, Stukel TA, Andrew A, et al. Human papillomavirus infectio n and incidence of squamous cell and basal cell carcinomas of the skin. J Natl Cancer Inst 2006;98:389-95. 37. Iftner A, Klug SJ, Garbe C, Blum A, Stancu A, Wilczynski SP, et al. The prevalence of human papillomavirus genotypes in nonmelanoma skin cancers of nonimmunosuppressed in- dividuals identifies high-risk genital types as possible risk factors. Cancer Res 2003;63:7515-9. 38. Amir H, Mbonde MP, Kitinya JN. Cutaneous squamous cell carcinoma in Tanzania. Cent Afr J Med 1992;38:439-43. 39. Hubbell CR, Rabin VR, Mora RG. Cancer of the skin in blacks, V: a review of 175 black patients with squamous cell
- 51. carcinoma of the penis. J Am Acad Dermatol 1988;18:292-8. 40. Caruso WR, Stewart ML, Nanda VK, Quismorio FP Jr. Squamous cell carcinoma of the skin in black patients with discoid lupus erythematosus. J Rheumatol 1987;14:156-9. 41. Johnson BL, Moy RL, White GM. Ethnic skin: medical and surgical. Toronto (Ontario, Canada): Mosby; 1998. 42. Mora RG, Perniciaro C, Lee B. Cancer of the skin in bl acks, III: a review of nineteen black patients with Bowen’s disease. J Am Acad Dermatol 1984;11:557-62. 43. Fleming ID, Barnawell JR, Burlison PE, Rankin JS. Skin cancer in black patients. Cancer 1975;35:600-5. 44. Chen YC, Christiani DC, Su HJ, Hsueh YM, Smith TJ, Ryan LM, etal.Early-lifeorlifetimesunexposure,sunreaction,andtherisk of squamous cell carcinoma in an Asian population. Cancer Causes Control 2010;21:771-6. 45. Koh D, Wang H, Lee J, Chia KS, Lee HP, Goh CL. Basal cell
- 52. carcinoma, squamous cell carcinoma and melanoma of the skin: analysis of the Singapore cancer registry data 1968-97. Br J Dermatol 2003;148:1161-6. 46. Watson M, Johnson CJ, Chen VW, Thomas CC, Weir HK, Sherman R, et al. Melanoma surveillance in the United States: http://www.census.gov http://www.census.gov http://refhub.elsevier.com/S0190-9622(13)01296-6/sref1 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref1 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref2 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref2 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref2 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref3 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref3 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref4 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref4 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref5 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref5 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref5 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref6 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref6 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref6 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref6 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref7 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref7 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref7 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref8 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref8 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref8 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref9 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref9
- 56. Agbai et al 761 overview of methods. J Am Acad Dermatol 2011;65(Suppl): S6-16. 47. Cartee TV, Kini SP, Chen SC. Melanoma reporting to central cancer registries by US dermatologists: an analysis of the persistent knowledge and practice gap. J Am Acad Dermatol 2011;65(Suppl):S124-32. 48. Surveillance, Epidemiology, and End Results (SEER) Program: SEER*Stat Database. National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch. Available at: http://www.seer.cancer.gov. Accessed April 5, 2012. 49. Cockburn MG, Zadnick J, Deapen D. Developing epidemic of melanoma in the Hispanic population of California. Cancer 2006;106:1162-8. 50. Bergfelt L, Newell GR, Sider JG, Kripke ML. Incidence and anatomic distribution of cutaneous melanoma among
- 57. United States Hispanics. J Surg Oncol 1989;40:222-6. 51. Vazquez-Botet M, Latoni D, Sanchez JL. Malignant mela- noma in Puerto Rico [in Spanish]. Bol Asoc Med P R 1990; 82:454-7. 52. Wu XC, Eide MJ, King J, Saraiya M, Huang Y, Wiggins C, et al. Racial and ethnic variations in incidence and survival of cutaneous melanoma in the United States, 1999-2006. J Am Acad Dermatol 2011;65(Suppl):S26-37. 53. Rahman Z, Taylor SC. Malignant melanoma in African Americans. Cutis 2001;67:403-6. 54. Collins RJ. Melanoma in the Chinese of Hong Kong: emphasis on volar and subungual sites. Cancer 1984;54:1482-8. 55. Tucker MA, Goldstein AM. Melanoma etiology: where are we? Oncogene 2003;22:3042-52. 56. Bradford PT, Goldstein AM, McMaster ML, Tucker MA. Acral lentiginous melanoma: incidence and survival patterns in the
- 58. United States, 1986-2005. Arch Dermatol 2009;145:427-34. 57. Cress RD, Holly EA. Incidence of cutaneous melanoma among non-Hispanic whites, Hispanics, Asians, and blacks: an analysis of California cancer registry data, 1988-1993. Cancer Causes Control 1997;8:246-52. 58. Sutherland CM, Mather FJ, Muchmore JH, Carter RD, Reed RJ, Krementz ET. Acral lentiginous melanoma. Am J Surg 1993; 166:64-7. 59. Stevens NG, Liff JM, Weiss NS. Plantar melanoma: is the incidence of melanoma of the sole of the foot really higher in blacks than whites? Int J Cancer 1990;45:691-3. 60. Pipitone M, Robinson JK, Camara C, Chittineni B, Fisher SG. Skin cancer awareness in suburban employees: a Hispanic perspective. J Am Acad Dermatol 2002;47:118-23. 61. Feun LG, Raub WA Jr, Duncan RC, Moffat F, Savaraj N, Nemeth A, et al. Melanoma in a southeastern Hispanic population. Cancer Detect Prev 1994;18:145-52.
- 59. 62. Hu S, Soza-Vento RM, Parker DF, Kirsner RS. Comparison of stage at diagnosis of melanoma among Hispanic, black, and white patients in Miami-Dade County, Florida. Arch Dermatol 2006;142:704-8. 63. Black WC, Goldhahn RT Jr, Wiggins C. Melanoma within a southwestern Hispanic population. Arch Dermatol 1987;123: 1331-4. 64. Chen YJ, Wu CY, Chen JT, Shen JL, Chen CC, Wang HC. Clinicopathologic analysis of malignant melanoma in Taiwan. J Am Acad Dermatol 1999;41:945-9. 65. Satoh S, Hashimoto-Tamaoki T, Furuyama J, Mihara K, Namba M, Kitano Y. High frequency of tetraploidy detected in malignant melanoma of Japanese patients by fluorescence in situ hybridization. Int J Oncol 2000;17:707-15. 66. Gallagher RP, Rivers JK, Yang CP, McLean DI, Coldman AJ, Silver HK. Melanocytic nevus density in Asian, Indo-Pakistani, and white children: the Vancouver mole study. J Am Acad
- 60. Dermatol 1991;25:507-12. 67. Reintgen DS, McCarty KM Jr, Cox E, Seigler HF. Malignant melanoma in black American and white American popula- tions: a comparative review. JAMA 1982;248:1856-9. 68. Zell JA, Cinar P, Mobasher M, Ziogas A, Meyskens FL Jr, Anton-Culver H. Survival for patients with invasive cutaneous melanoma among ethnic groups: the effects of socioeco- nomic status and treatment. J Clin Oncol 2008;26:66-75. 69. Friedman LC, Bruce S, Weinberg AD, Cooper HP, Yen AH, Hill M. Early detection of skin cancer: racial/ethnic differences in behaviors and attitudes. J Cancer Educ 1994;9:105-10. 70. Weinstock MA, Gardstein B. Twenty-year trends in the reported incidence of mycosis fungoides and associated mortality. Am J Public Health 1999;89:1240-4. 71. Criscione VD, Weinstock MA. Incidence of cutaneous T-cell lymphoma in the United States, 1973-2002. Arch Dermatol 2007;143:854-9.
- 61. 72. Di Landro A, Marchesi L, Naldi L, Motta T, Cainelli T. A case of hypopigmented mycosis fungoides in a young Caucasian boy. Pediatr Dermatol 1997;14:449-52. 73. Akaraphanth R, Douglass MC, Lim HW. Hypopigmented mycosis fungoides: treatment and a 6(1/2)-year follow-up of 9 patients. J Am Acad Dermatol 2000;42:33-9. 74. Whitmore SE, Simmons-O’Brien E, Rotter FS. Hypopigmented mycosis fungoides. Arch Dermatol 1994;130:476-80. 75. Miller RW, Rabkin CS. Merkel cell carcinoma and melanoma: etiological similarities and differences. Cancer Epidemiol Biomarkers Prev 1999;8:153-8. 76. Anzai S, Sato T, Takayasu S, Asada Y, Terashi H, Takasaki S. Postoperative hyponatremia in a patient with ACTH-producing Merkel cell carcinoma. J Dermatol 2000;27:397-400. 77. Taylor SC. Enhancing the care and treatment of skin of color, part 2: understanding skin physiology. Cutis 2005;76:302-6.
- 62. 78. Kotrajaras R, Kligman AM. The effect of topical tretinoin on photodamaged facial skin: the Thai experience. Br J Dermatol 1993;129:302-9. 79. Griffiths CE, Wang TS, Hamilton TA, Voorhees JJ, Ellis CN. A photonumeric scale for the assessment of cutaneous photo- damage. Arch Dermatol 1992;128:347-51. 80. Larnier C, Ortonne JP, Venot A, Faivre B, Beani JC, Thomas P, et al. Evaluation of cutaneous photodamage using a photo- graphic scale. Br J Dermatol 1994;130:167-73. 81. Chan HHL, Jackson B. Laser treatment on ethnic skin. In: Lim HW, Hoenigsmann H, Hawk JLM, editors. Photoderma- tology. New York: Informa Healthcare; 2007. 82. Chung JH, Lee SH, Youn CS, Park BJ, Kim KH, Park KC, et al. Cutaneous photodamage in Koreans: influence of sex, sun exposure, smoking, and skin color. Arch Dermatol 2001;137: 1043-51.
- 63. 83. Chan HH, Manstein D, Yu CS, Shek S, Kono T, Wei WI. The prevalence and risk factors of post-inflammatory hyper- pigmentation after fractional resurfacing in Asians. Lasers Surg Med 2007;39:381-5. 84. Kim M, Boone SL, West DP, Rademaker AW, Liu D, Kundu RV. Perception of skin cancer risk by those with ethnic skin. Arch Dermatol 2009;145:207-8. 85. Summers P, Bena J, Arrigain S, Alexis AF, Cooper K, Bordeaux JS. Sunscreen use: non-Hispanic blacks compared with other racial and/or ethnic groups. Arch Dermatol 2011;147:863-4. 86. Hall HI, Rogers JD. Sun protection behaviors among African Americans. Ethn Dis 1999;9:126-31. 87. Buster KJ, You Z, Fouad M, Elmets C. Skin cancer risk perceptions: a comparison across ethnicity, age, education, gender, and income. J Am Acad Dermatol 2012;66:771-9. http://refhub.elsevier.com/ S0190-9622(13)01296-6/sref45 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref45
- 67. http://refhub.elsevier.com/S0190-9622(13)01296-6/sref80 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref82 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref82 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref82 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref82 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref83 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref83 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref83 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref84 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref84 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref84 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref85 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref85 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref86 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref86 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref86 J AM ACAD DERMATOL APRIL 2014 762 Agbai et al 88. Sanclemente G, Zapata JF, Garcia JJ, Gaviria A, Gomez LF, Barrera M. Lack of correlation between minimal erythema dose and skin phototype in a Colombian scholar population. Skin Res Technol 2008;14:403-9. 89. Kundu RV, Kamaria M, Ortiz S, West DP, Rademaker AW, Robinson JK. Effectiveness of a knowledge-based interven- tion for melanoma among those with ethnic skin. J Am Acad
- 68. Dermatol 2010;62:777-84. 90. Vanchinathan V, Lim HW. A dermatologist’s perspective on vitamin D. Mayo Clinic Proc 2012;87:372-80. 91. Diehl JW, Chiu MW. Effects of ambient sunlight and photoprotection on vitamin D status. Dermatol Ther 2010; 23:48-60. 92. Nesby-O’Dell S, Scanlon KS, Cogswell ME, Gillespie C, Hollis BW, Looker AC, et al. Hypovitaminosis D prevalence and de- terminants among African American and white women of reproductive age: third National Health and Nutrition Examination Survey, 1988-1994. Am J Clin Nutr 2002;76: 187-92. 93. Cusack C, Danby C, Fallon JC, Ho WL, Murray B, Brady J, et al. Photoprotective behavior and sunscreen use: impact on vitamin D levels in cutaneous lupus erythematosus. Photo- dermatol Photoimmunol Photomed 2008;24:260-7. 94. Holme SA, Anstey AV, Badminton MN, Elder GH. Serum
- 69. 25-hydroxyvitamin D in erythropoietic protoporphyria. Br J Dermatol 2008;159:211-3. 95. Linos E, Keiser E, Kanzler M, Sainani KL, Lee W, Vittinghoff E, et al. Sun protective behaviors and vitamin D levels in the US population: NHANES 2003-2006. Cancer Causes Control 2012; 23:133-40. 96. Sollitto RB, Kraemer KH, DiGiovanna JJ. Normal vitamin D levels can be maintained despite rigorous photoprotection: six years’ experience with xeroderma pigmentosum. J Am Acad Dermatol 1997;37:942-7. 97. Norval M, Wulf HC. Does chronic sunscreen use reduce vitamin D production to insufficient levels? Br J Dermatol 2009;161:732-6. 98. Ross AC, Manson JE, Abrams SA, Aloia JF, Brannon PM, Clinton SK, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab 2011;96:53-8. 99. National Institutes of Health Office of Dietary Supplements.
- 70. Dietary supplement fact sheet: Vitamin D. Available at: http:// ods.od.nih.gov/factsheets/VitaminD-QuickFacts/. Accessed April 2, 2012. 100. Pourciau CY, Eide MJ, Mahan M, Lim HW. Photoprotection counseling of non-white ethno-racial groups: a survey of the practice of expert dermatologists. Photodermatol Photo- immunol Photomed 2012;28:335-7. 101. Damian DL, Halliday GM, Stc Barnetson R. Sun protection factor measurement of sunscreens is dependent on minimal erythema dose. Br J Dermatol 1999;141:502-7. 102. Wang SQ, Lim HW. Current status of the sunscreen regulation in the United States: 2011 Food and Drug Administration’s final rule on labeling and effectiveness testing. J Am Acad Dermatol 2011;65:863-9. http://refhub.elsevier.com/S0190-9622(13)01296-6/sref87 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref87 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref87 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref87 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref88
- 72. http://ods.od.nih.gov/factsheets/ VitaminD-QuickFacts/ http://ods.od.nih.gov/factsheets/VitaminD-QuickFacts/ http://refhub.elsevier.com/S0190-9622(13)01296-6/sref98 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref98 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref98 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref98 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref99 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref99 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref99 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref100 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref100 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref100 http://refhub.elsevier.com/S0190-9622(13)01296-6/sref100Skin cancer and photoprotection in people of color: A review and recommendations for physicians and the publicDefinitionsIntroductionBiological basis of skin carcinogenesis and photoaging in POCBasal cell carcinomaBCC in blacksBCC in HispanicsBCC in AsiansSquamous cell carcinomaSCC in blacksSCC in AsiansMalignant melanomaMM in blacksMM in HispanicsMM in AsiansSurvival in MM across ethnicitiesMycosis fungoidesOther skin cancersPhotoaging and UV-related dyspigmentation in POCSun-protection beliefs and practices in POCVitamin D and photoprotectionThe SPF and recommendations for clinical practiceReferences Unit 5 Assignment Contract Terms Template LAW204 – Business Law I Quoted Definition with Citation Definition (in your own words) Example Offer
- 73. Acceptance Bilateral Contract Unilateral Contract Promissory Estoppel References Due Date: 11:59 p.m. EST, Sunday of Unit 5 Points: 100 Overview:
- 74. Regardless of whether you own a business or are a stakeholder in a business, understanding basic contract terms is important. Businesses enter into contracts with many areas, from shipping to suppliers to customers. As a business owner or manager knowledge of these basic terms will assist you in the day to day operations of the business, regardless of the field. Instructions: • Fill in the attached template. • For each term, define the term with citation to authority, define the term in your own words and provide an example of each term. Requirements: • Use APA format for non-legal sources such as the textbook. Use Bluebook citation format for any legal citations. • Submit a Word document using the template. • Maximum two pages in length, excluding the Reference page. Be sure to read the criteria below by which your work will be evaluated before you write and again after you write. LAW204 – Business Law I
- 75. Contract Terms Evaluation Rubric for Contract Terms Assignment CRITERIA Deficient Needs Improvement Proficient Exemplary 0 – 44 Points 45 – 59 Points 60 – 74 Points 75 Points Contract Terms Does not concisely and clearly defines most terms. Somewhat concisely and clearly defines some terms. Mostly concisely, succinctly, and clearly defines most
- 76. terms. Concisely, succinctly, and clearly defines each term. 0 – 5 points 6 – 7 points 8 – 9 points 10 points Paper Length More than 2 pages n/a n/a 2 pages or less 0 – 8 points 9 – 11 points 12 – 14 points 15 points Clear and Professional Writing and APA/Bluebook Format Errors impede professional presentation; guidelines not followed. Significant errors that do not impede professional
- 77. presentation. Few errors that do not impede professional presentation. Writing and format are clear, professional, APA/Bluebook compliant, and error free. Overview:Instructions:Requirements:Evaluation Rubric for Contract Terms Assignment